
Abstract
This study sought to evaluate the candidacy of plasma osteopontin (OPN) as a biomarker of COVID-19 severity and multisystem inflammatory condition in children (MIS-C) in children. A retrospective analysis of 26 children (0–21 years of age) admitted to Children’s Healthcare of Atlanta with a diagnosis of COVID-19 between March 17 and May 26, 2020 was undertaken. The patients were classified into three categories based on COVID-19 severity levels: asymptomatic or minimally symptomatic (control population, admitted for other non-COVID-19 conditions), mild/moderate, and severe COVID-19. A fourth category of children met the Centers for Disease Control and Prevention's case definition for MIS-C. Residual blood samples were analyzed for OPN, a marker of inflammation using commercial ELISA kits (R&D), and results were correlated with clinical data. This study demonstrates that OPN levels are significantly elevated in children hospitalized with moderate and severe COVID-19 and MIS-C compared to OPN levels in mild/asymptomatic children. Further, OPN differentiated among clinical levels of severity in COVID-19, while other inflammatory markers including maximum erythrocyte sedimentation rate, C-reactive protein and ferritin, minimum lymphocyte and platelet counts, soluble interleukin-2R, and interleukin-6 did not. We conclude OPN is a potential biomarker of COVID-19 severity and MIS-C in children that may have future clinical utility. The specificity and positive predictive value of this marker for COVID-19 and MIS-C are areas for future larger prospective research studies.
Impact statement
To date, biomarkers correlating with severity of COVID-19 disease and multisystem inflammatory syndrome (MIS-C) remain elusive. The management of patients with SARS-CoV-2 infection would be facilitated with a reliable biomarker that is biologically stable, easily accessible, and can be rapidly and inexpensively measured at point of care. Osteopontin (OPN), a matricellular protein with diverse physiologic and pathologic functions in a variety of inflammatory and immune processes, has these features. This study demonstrates that OPN is significantly upregulated in the plasma of hospitalized children with SARS-CoV-2 infection and MIS-C versus mild/asymptomatic children. Further, OPN levels correlate with clinical severity of COVID-19, also with statistical significance. These new data suggest that OPN is a putative biomarker to guide risk stratification, prognostication, and clinical management of children with COVID-19 and MIS-C. The clinical utility of OPN as a COVID-19 biomarker requires validation in larger studies.
Introduction
The COVID-19 pandemic has resulted in significant morbidity and mortality and has been a significant, disrupting force in the global community. According to the U.S. Centers for Disease Control and Prevention (CDC), as of 3 August 2021, there have been total of 35,171,679 confirmed COVID-19 cases and 611,791 COVID-19-related deaths in the United States, 1 including 4.2 million COVID-19 cases in children as of 29 July 2021. 2
We have a limited understanding of why some infected individuals remain asymptomatic with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection while others develop severe or lethal disease. In many severe cases, COVID-19 is not localized to the respiratory tract but appears to be a multisystem disease with activation of inflammatory and coagulative cascades.3,4 While fewer children have been affected by severe COVID-19 compared to adults, children can have severe COVID-19 sequelae, including a rare, but serious condition associated with systemic hyperinflammatory responses following SARS-CoV-2 infection—multisystem inflammatory syndrome in children (MIS-C).5,6 Although the pathogenesis of MIS-C is poorly understood, it is clinically characterized by systemic hyperinflammation, which can be severe and require intensive care, and multiorgan involvement including myocardial involvement, shock, and Kawasaki disease-like features.7–9 MIS-C has some overlapping features with Kawasaki Disease and macrophage activation syndrome; however, the clinical and immune phenotypes appear to be distinct. 10
Timely diagnosis, hospitalization, therapy selection, and effective allocation of intensive care services could all be improved with early risk stratification of both COVID-19 and MIS-C. 11 Biomarkers correlating with severe COVID-19, MIS-C, and organ-specific disease, including those associated with pulmonary, cardiac, hepatic, renal, and neurologic systems, have proven elusive.12–14
Osteopontin (OPN) has received less attention as a biomarker of COVID-19 but may make an attractive candidate. OPN, first identified in bone, has been demonstrated in multiple epithelial surfaces.15,16 OPN belongs to the small integrin-binding ligand N-link glycoprotein family and is highly stable in blood and exists in low quantities in healthy individuals.17,18 OPN exists as part of the extracellular matrix and as a soluble cytokine. 19 OPN is ubiquitous and multifunctional.20–22 Although OPN is known to play a role in both physiologic and pathophysiologic processes, the exact mechanisms of action still requires elucidation.16–18,23–27 OPN is known to be involved in a number of normal biological processes including bone remodeling and immune modulation, but it is unclear if these effects are beneficial or detrimental (or both) to health.20,22 Pathologically, OPN has known roles in cancer, diabetes, kidney stones, lung, and cardiovascular diseases.20–23 While not a specific marker, levels of OPN have been used to follow disease progression, response to treatment, and guide prognosis in diverse pathologies, including tumor progression, atherosclerosis, and diabetic nephropathy.20,28,29
Although the pathophysiologic basis for the overexpression of OPN in these diverse pathologies is not yet fully elucidated, OPN is implicated in both inflammation and immune responses.20–23 A recent study suggests that OPN predicts severity of illness in adult patients with COVID-19. 22
The purpose of this retrospective study was to compare levels of plasma OPN obtained at a single time point in children hospitalized with COVID-19 and MIS-C and to correlate OPN levels with severity of illness and clinical presentation.
Materials and methods
Study population
This study was approved by the Children’s Healthcare of Atlanta (Children's) Institutional Review Board (IRB). Samples were collected through a pediatric specimen collection protocol from 17 March 2020 to 26 May 2020. Blood samples were collected from hospitalized children and young adults (0–21 years of age), who were eligible if they had a known or suspected disease of public health importance (e.g. COVID-19 or MIS-C). OPN measurements were obtained from residual plasma following clinical laboratory diagnostics. Demographic, clinical, laboratory, treatment, and outcome data were abstracted from the electronic medical record and were recorded on a standardized case report form.
Participants were classified into categories based on COVID-19 severity levels, including mild or asymptomatic, moderate, severe, and children meeting the CDC case definition of MIS-C. Children designated as mild or asymptomatic were those admitted to the hospital for other conditions (e.g. psychiatric) who subsequently tested positive for SARS-CoV-2 by nasopharyngeal real-time polymerase chain reaction (RT-PCR) upon screening. Children designated as moderate included any child hospitalized with symptomatic COVID-19 who were not classified as severe. Children designated as severe had symptomatic COVID-19 and either respiratory insufficiency requiring >/= high-flow nasal cannula or shock requiring vasopressors. Children were classified as having MIS-C if they met the CDC case definition. 30
An independent committee, the COVID-19 Feasibility & Optimization of Research at Children’s committee, allocates participants to each of the 76 ongoing, IRB-approved COVID-19 studies at Children’s and Emory University. Additional information about study protocol and design has been published. 31 Twenty-six randomly selected patients with sufficient available specimens within the disease severity groups were allocated to this pilot study.
Laboratory tests
The DiaSorin Molecular Simplexa COVID-19 Direct RT-PCR assay, which has an analytical sensitivity or limit of detection of 500 viral copies per mL when specimens are collected by using a nasopharyngeal swab, with near-perfect specificity for distinguishing from endemic human coronaviruses was utilized. 32
Osteopontin assay
Plasma was collected at the time of enrollment in the study. Viral inactivation of the plasma was performed by incubation with Triton X-100 to a final concentration of 1% for 1 h prior to use. 33 Human plasma samples were analyzed in duplicate using commercial ELISA kits (R&D). According to the manufacturer’s protocol, the inactivated plasma samples were diluted 1:25 with the dilution buffer provided in the kit.
Statistical analysis
Descriptive statistics for the study were reported as medians and ranges for continuous data and counts and percentages for categorical data. Normality of continuous data was assessed using Shapiro-Wilk tests. Given the four groups of interest (mild/asymptomatic COVID-19, moderate COVID-19, severe COVID-19, and MIS-C), comparisons of continuous data were conducted using Kruskal-Wallis tests for non-normally distributed data or analysis of variance (ANOVA) tests for normally distributed data. Categorical data were compared using chi-squared tests or Fisher’s exact tests for cell counts <5. All statistical tests were assessed at the 0.05 significance level. Statistical analysis was conducted using SAS 9.4 (Cary, NC) and SPSS 27.0 (IBM, 2020).
Results
Patient demographics
Demographic and clinical variables are presented in Table 1. Days of symptom onset, characterized by number of days from parent-reported symptom onset to collection of blood, were variable but did not differ between groups (range 1–33 days). No differences were found across severity groups on demographic variables. Differences were noted between groups for ICU duration (P < .001) and treatment received (P = .007).
Patient demographic and medical characteristics, median and range.
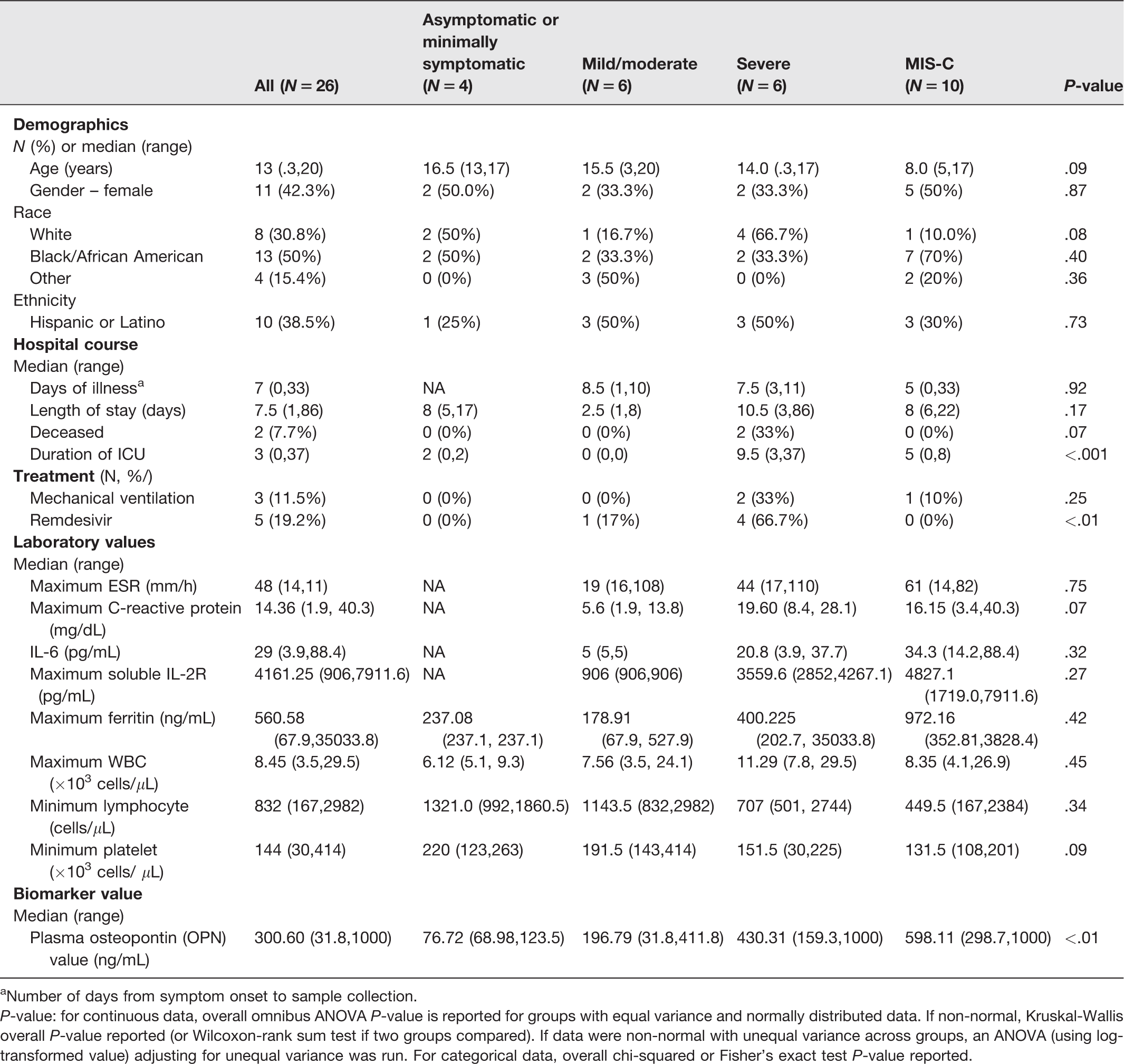
aNumber of days from symptom onset to sample collection.
P-value: for continuous data, overall omnibus ANOVA P-value is reported for groups with equal variance and normally distributed data. If non-normal, Kruskal-Wallis overall P-value reported (or Wilcoxon-rank sum test if two groups compared). If data were non-normal with unequal variance across groups, an ANOVA (using log-transformed value) adjusting for unequal variance was run. For categorical data, overall chi-squared or Fisher’s exact test P-value reported.
OPN levels
Plasma OPN levels significantly differed across the groups (P < .05; see Table 1 and Figure 1). The severe COVID-19 and MIS-C groups had significantly higher levels of OPN at time of collection (median = 430.31 and 598.11 ng/mL, respectively) compared to the other two groups.
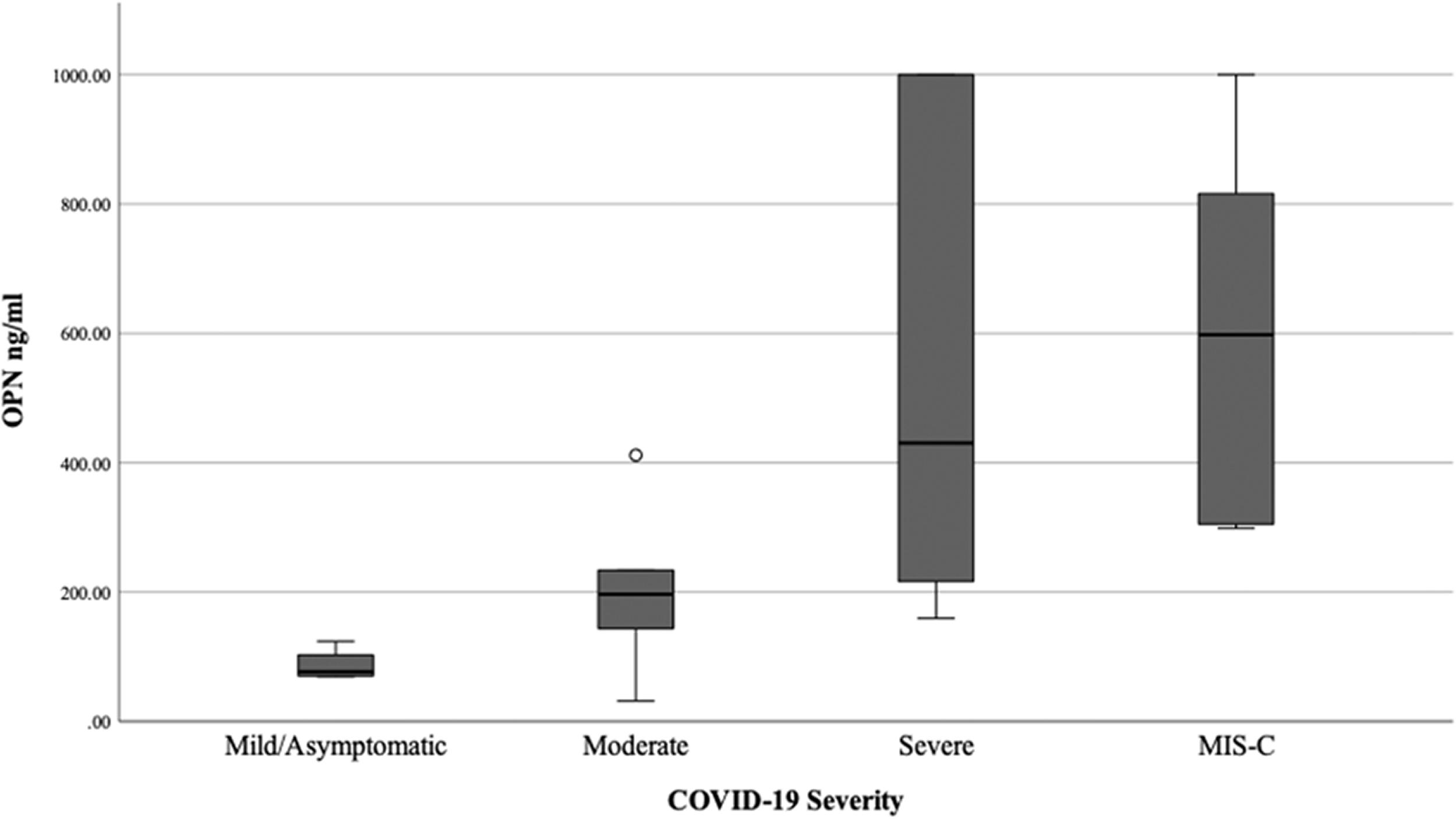
Osteopontin levels by disease severity.
Laboratory tests
Laboratory values across severity group are summarized in Table 1. No statistically significant differences were found across severity groups.
Discussion
Although the incidence of severe COVID-19 is higher in older adults, children are also at risk for severe COVID-19 disease course. 5 In the United States, 340 children have died from COVID-19 (as of 29 July 2021), 34 4196 have been diagnosed with MIS-C, with an additional 37 dying from MIS-C (as of 28 June 2021). 35 Additionally, given that COVID-19 vaccines have been authorized for emergency use in adults and children down to 12 years of age in the United States, younger children may be increasingly vulnerable to new infection. Children are increasingly accounting for a larger proportion of new cases (14.3% of total cumulative U.S. cases, but for the week of 22–29 July 2021, children accounted for 19.0% of new reported weekly COVID-19 cases). 2
Given that more than one in 10 children seeking emergency department care for COVID-19 is hospitalized, and that nearly one-third of children hospitalized with COVID-19 have severe disease (requiring admission to the intensive care unit, mechanical ventilation), identifying those most at-risk is critical to timely care and proper allocation of resources.36,37 While rare, with an estimated incidence of 2 per 100,000 children, more than three-quarters of children with MIS-C require a pediatric intensive care unit admission (77%). 38 Although the pathogenesis of COVID-19 and MIS-C in children are distinct, both disease processes may involve systemic hyperinflammatory response with end-organ involvement.39,40 We therefore hypothesized that OPN may be a biomarker for severe COVID-19 and MIS-C.
Since currently there is no reliable clinical, laboratory, or radiographic marker that can identify early in the hospital course which children with COVID-19 will have progressive disease severity,11,41 this study sought to evaluate the utility of plasma OPN levels to serve as a biomarker for severity in children admitted to a tertiary care pediatric hospital with COVID-19 or MIS-C. In addition, we sought to examine whether these levels are related to severity of illness. Results show elevated levels of OPN in all hospitalized children with moderate or severe COVID-19. It is noteworthy that OPN levels are negligible in healthy children.42,43
Further, OPN levels relate to disease severity with higher OPN levels in the more severe compared to moderate disease groups. OPN levels were highest among children with MIS-C. These findings are consistent with the conclusions of Varim et al. that found that OPN was related to disease severity in a cohort of 84 adult patients diagnosed with COVID-19. 22
OPN is a multifunctional and ubiquitous glycoprotein.20–22 OPN is highly stable in blood and exists in low quantities in healthy individuals making it an attractive candidate biomarker.17,18 The feasibility of point-of-care measurement would facilitate OPN’s clinical utility. While OPN is known to be released in many tissues and cell types, physiologically, OPN is implicated in both inflammation and immune responses.20,22 Previous studies have demonstrated immune cells release OPN and that OPN plays a role in early T lymphocyte activation; as a chemotactic factor for neutrophils, mast cells, and macrophages; and in immunoglobulin production.19–22
While Varim et al. reported a statistically significant increase in OPN level in adults with COVID-19 the observed OPN level and magnitude of difference between the two groups studied, non-critically ill and critically ill groups, was 9.98 vs. 13.75 ng/mL, respectively. 22 This was much lower compared to our results in this report of children with COVID-19, in which we found the median OPN levels in asymptomatic or minimally symptomatic, mild/moderate, severe, and MIS-C groups to be 76.72, 196.79, 430.31, and 598.11 ng/ml, respectively, which is much lower than the reported mean plasma OPN (23.56 ± 19.73 ng/mL) level of healthy adult subjects. 43 We observed a greater than five-fold increase in the OPN level between the asymptomatic and MIS-C patients and several folds higher than the reported OPN level (median value of 54.5 ng/mL) in a healthy pediatric population. 42 This wide difference in OPN values range between Varim et al. 22 and our study may be attributed to age (adult versus pediatric) or methodological difference in the assay performed in serum versus inactivated plasma samples.
Although this study examined the relationship between plasma OPN levels and COVID-19 disease severity, we and others have been previously evaluating OPN as a measure of brain inflammation associated with traumatic brain injury prior to the COVID-19 pandemic.44,45 Given the inflammatory processes and neurological manifestations associated with severe COVID-19 and MIS-C,46–48 we considered whether OPN, a marker of neuroinflammation, has the potential to assist in the prognosis or monitoring of neurological manifestations of COVID-19. It is noteworthy that coronaviruses are known to infect the central nervous system and there is evidence of neurological deficits, including brain injury, in some COVID-19 patients.11,12 Recent reports suggest glial fibrillary acidic protein, neurofilament light polypeptide, and tau biomarkers may be useful as biomarkers for COVID-19.11,12 Further study is needed to determine if these markers alone or in combination with OPN can serve as markers of neuroinflammation in COVID-19 afflicted children.
In our prior translational studies that examined OPN levels in pediatric TBI, we found that both admission and the trajectory of subsequent serial OPN levels were predictive of clinical severity and prognosis.36,37 In this study of pediatric COVID-19 patients, only a single OPN value was investigated. Future investigation should examine the relationship between serial measures of OPN and COVID-19 disease course, as the trajectory of OPN levels may have more significance than any isolated OPN measurement, including monitoring response to any medical treatments.
In this pilot study, it appears that OPN may be a more sensitive marker of COVID-19 severity in children compared to other markers examined. Unlike in Varim's study of adult COVID-19 patients, which found higher white blood cell (WBC), neutrophil, D-dimer, C-reactive protein (CRP), and ferritin levels and lower lymphocyte and albumin levels, in critically ill patients, 22 in this pediatric study, only OPN was related to COVID-19 severity and MIS-C. No other markers evaluated (erythrocyte sedimentation rate, CRP, intrleukin-6, soluble interleukin-2R, ferritin, WBC, lymphocyte, or platelet) demonstrated significant differences between COVID-19 severity groups, which may in part be attributed to the sample size.
This study has limitations. First, the study included only 26 children from a single institution with small numbers in each COVID-19 severity group. Second, this study only measured OPN at the single time point of study enrollment. Serial measurements will facilitate a better understanding of the relation to OPN levels to disease progression and the utility of OPN as a biomarker of COVID-19 infections, including early risk stratification and monitoring efficacy of therapeutic interventions. Lastly, the current data do not indicate whether elevated OPN levels are reflective of overall systemic disease burden or are organ specific. The specificity and positive predictive value of this marker for COVID-19 and MIS-C are areas for future larger prospective research studies.
In conclusion, this study demonstrates with statistical significance that OPN levels obtained on hospital admission are related to the clinical severity of COVID-19 in children, with the highest levels noted in children with MIS-C. Further, OPN was able to differentiate levels of severity in COVID-19 infection, while other commonly used inflammatory markers, including maximum ESR, CRP and ferritin, minimum lymphocyte and platelet counts, as well as soluble interleukin-2R and interleukin-6, were not. Further study with a larger cohort is needed to assess the performance of OPN as a biomarker of COVID-19 severity and MIS-C in children.
Footnotes
AUTHORS' CONTRIBUTIONS
All authors made substantial contributions to the study, analyzed the data and interpreted the final result. In addition, all authors reviewed or edited the manuscript, and gave final approval of the submitted manuscript. AR, LSB, IS, EJA, ALS, and CAR conceptualized the project; AR, SH, and CAR provided supervision and oversight; AR and SH garnered funding and resources; ALS, EJA, CAR, AL, and LH curated clinical data of clinical COVID patient database; IS and BW analyzed plasma samples; statistical analysis done by LSB, SH, JF, and HEM.
ACKNOWLEDGMENTS
We thank clinical research coordinators Beena Desai, Kerry Dibernardo, Felicia Glover, Vikash Patel, Maureen Richardson, Amber Samuel, and clinical research nurses Lisa Macoy and Kathy Stephens for their assistance enrolling patients and collecting specimens. We thank Nadine Rouphael and the Hope Clinic laboratory, Theda Gibson, Wensheng Li, Hui-Mien Hsiao, Stacey A. Lapp, and the Emory Children’s Center Vaccine Research Center laboratory for their assistance processing specimens. We thank the Children’s Healthcare of Atlanta research laboratory for their assistance in collecting residual specimens. And lastly, we thank the study participants and their families for generously donating their time and blood to further our understanding of COVID-19 in children.
DECLARATION OF CONFLICTING INTERESTS
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Evan J Anderson (EJA) has received personal fees from AbbVie, Pfizer, Janssen, and Sanofi Pasteur for consulting, and his institution receives funds to conduct clinical research unrelated to this manuscript from MedImmune, Regeneron, PaxVax, Pfizer, GSK, Merck, Novavax, Sanofi-Pasteur, Janssen, and Micron. He also serves on a safety monitoring board for Sanofi-Pasteur and Kentucky BioProcessing, Inc.
Christina A Rostad (CAR)’s institution has received funds to conduct clinical research unrelated to this manuscript from the National Institutes of Health, BioFire Inc, GSK, MedImmune, Micron, Janssen, Merck, Moderna, Novavax, PaxVax, Pfizer, Regeneron, and Sanofi-Pasteur. She is co-inventor of patented RSV vaccine technology unrelated to this manuscript, which has been licensed to Meissa Vaccines, Inc.
FUNDING
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by the Elaine and John C. Carlos Fund at Children's Healthcare of Atlanta.