
Abstract
Whole-body vibration (WBV), which is widely used as a type of exercise, involves the use of vibratory stimuli and it is used for rehabilitation and sports performance programmes. This study aimed to investigate the effect of WBV treatment in a chronic pain model after 10 WBV sessions. An animal model (chronic pain) was applied in 60 male Wistar rats (±180 g, 12 weeks old) and the animals were treated with low intensity exercise (treadmill), WBV (vibrating platform), and a combined treatment involving both. The controls on the platform were set to a frequency of 42 Hz with 2 mm peak-to-peak displacement, g ≈ 7, in a spiral mode. Before and after the vibration exposure, sensitivity was determined. Aβ-fibers-mediated mechanical sensitivity thresholds (touch-pressure) were measured using a pressure meter. C-fibers-mediated thermal perception thresholds (hot pain) were measured with a hot plate. After each session, WBV influenced the discharge of skin touch-pressure receptors, reducing mechanical sensitivity in the WBV groups (P < 0.05). Comparing the conditions “before vs. after”, thermal perception thresholds (hot pain) started to decrease significantly after the third WBV session (P < 0.05). WBV decreases mechanical hyperalgesia after all sessions and thermal sensitivity after the third session with the use of WBV.
Impact statement
Whole-body vibration (WBV) exercise, low intensity exercise (walking), and a combined protocol were used in this study to treat a chronic pain model in Wistar rats. To our knowledge, the presumed beneficial effect of WBV on chronic pain reduction in lower limbs based on its interaction and the comparison with low intensity exercise has not yet been documented. This study concluded that WBV exercise mediates the decrease in mechanical hypersensitivity through Aβ-fiber and thermal sensation (hot pain) through C-fiber in rats subjected to a chronic pain model. These findings can influence therapeutic interventions, in cases that hypersensitivity negatively affects an exercise session. Pain prevents the patient from adequately performing the rehabilitation movement and a reduction in sensitivity and the consequent reduction in pain might be helpful. Rehabilitation programmes can benefit from knowledge about the correct parameter settings of the exposure to WBV.
Introduction
Locomotor system dysfunctions are the most common causes of chronic pain, 1 presenting a prevalence between 20% and 60% in adults and elderly.2–4 It is estimated that chronic pain affects at least 116 million US adults and, annually, it cost up to $560 billion. 1 The lack of predictability in the behavioral response to a noxious stimulus to the development of chronic pain after physical damage has been discussed by researchers and clinicians for decades.
A pH tissue decrease has been detected following inflammation, bruising, and pain.5,6 There is a positive correlation between pain and local acidification. 5 In humans, the decrease in pH increases the activity of nociceptors leading to painful response. 7 Decreases in local pH can be considered one of the multiples stressors that can induce long-lasting and widespread hyperalgesia. Decreased pH activates nociceptors to produce hyperalgesia and contributes to the chronic widespread pain development, including the locomotor system. 8
In the management of painful conditions, exercise is an important component.9,10 Protocols including low intensity exercise are used in the rehabilitation of patients with musculoskeletal chronic conditions such as myalgia 2 and fibromyalgia.11,12
Animal studies have found that physical exercise (running) is related to neuroprotection, apoptosis suppression, and neurotrophic factors, which generate neurogenesis and regeneration.13,14 However, due to the presence of pain, a limited capacity to expend energy and/or impaired movement coordination, numerous diseases prevent the affected subjects from performing exercises by themselves, thus hindering the rehabilitation process.
Whole-body vibration (WBV) intervention platforms have been widely used as a modality of exercise. Research on the responses to WBV can contribute to produce safe recommendations for the equipment’s use.15–18 The use of external vibratory mechanical stimuli, which decreases the deficit in voluntary muscle activation by neuromuscular stretch reflex, has been shown to be an efficient method for persons with severe disability. Considering that reflexes with similar patterns have been identified during running exercise, 19 one can speculate that vibratory stimuli may provide other beneficial effects.
Vibratory stimulus can also be used to decrease the pain perception.20,21 Pain can be attenuated by the large-diameter afferents activation, which may change transmission in the central nervous system.22,23 The impact of vibration stimulation on large-diameter afferents was found by touch-pressure sensitivity measurements directly after WBV17,24,25 and the perception of vibration at 30 Hz 25 and 200 Hz25,26 with sensitivity reduction. Following WBV, it has been shown to take between 2 and 3 h for sensitivity to return to the baseline condition. 25
Nociceptors are responsible for conducting pain information. Their nerve conduction pathway to the encephalic region is different from that of the myelinated Aα and Aβ mechanoreceptors. Thus, a question that arises is whether WBV also influences the role of nociceptors in the control of painful conditions. However, in afferent modulation, pain can be reduced by simultaneous activity in low-threshold receptors (Aβ-fibers). 27 Considering that WBV affects the firing of mechanoreceptors,17,24–26 causing decreased skin sensitivity, a question remains regarding the influence of WBV on afferent pain modulation. 28
To the best of our knowledge, the presumed beneficial impact of WBV on pain reduction has not yet been reported. Thus, this study aimed to investigate the effects of WBV treatment in Wistar rats submitted to a chronic pain model through the Aβ-fiber mediated mechanical hyperalgesia and C-fiber mediated thermal stimulation (hot pain). Our hypothesis is that the afferent discharges from touch-pressure mechanoreceptors will be impaired; as well thermal sensitivity (hot pain) will decrease after WBV training in a chronic pain model.
Materials and methods
Animals
Male Wistar rats (n = 60; 12 weeks old, weighing 180 to 200 g), from a local breeding colony of Federal University of Rio Grande do Sul (UFRGS) were accommodated under environmental standard laboratory conditions, respecting a 12/12 h light/dark cycle, and food/water available ad libitum. Efforts were made to avoid the animals suffering and to decrease the sample size. The study followed the recommendations of the Sociedade Brasileira de Neurociências, the International Brain Research Organization, and the Arouca Brazilian Law (11794/2008) to the animals’ care. The study was approved, under protocol number 2012-062, by the Ethical Committee for the use of Animals. The methods complied with the National Institute of Health’s Guidelines for the Care and Use of Laboratory Animals (publication no. 85-23, revised 1985). Data collection was made at the Comparative Neurohistophysiology Laboratory of the Federal University of Rio Grande do Sul.
Sample size estimation (12 animals per group) was established considering an expected difference between groups, as suggested by previous study with similar analyses. 9 Sample size was calculated through the software nQuery Advisor 3.0 (Núcleo de Auxílio Estatístico-NAE, UFRGS), with P ≤ 0.05 and power of 90%.
Experimental design
The animals were divided into five groups: control saline sedentary (SS), control chronic pain sedentary (PS), chronic pain subjected to low intensity exercise training group (PE), chronic pain treated with whole-body vibration group (PV), and chronic pain treated with low intensity exercise plus vibration training group (PE + V) during a 15-day protocol (Figure 1).
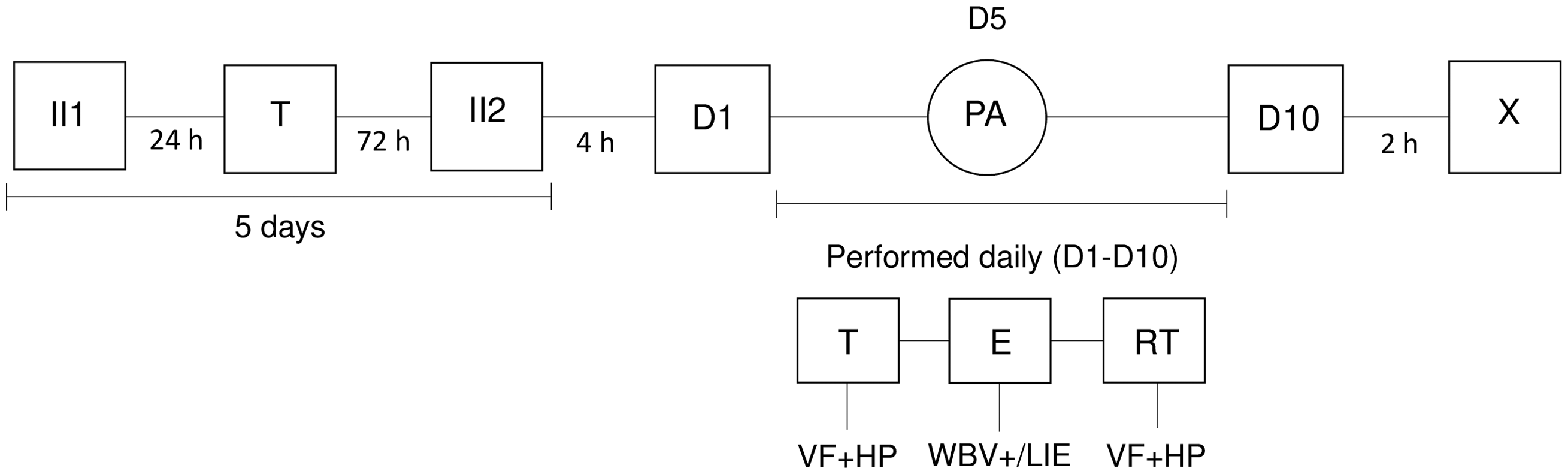
Experimental design. First intramuscular injection (II1); test (T); second intramuscular injection (II2); day 1 (D1); day 5 (D5); exercise parameter adjustment (PA); day 10 (D10); exercise (E); Von Frey + hot plate (VF + HP); WBV and or low intensity exercise (WBV+/LIE); retest (RT); animal sacrifice (X).
Animals with chronic pain that were able to walk on the treadmill were included in the experiment and randomly assigned to the experimental groups. Animals that did not develop hyperalgesia (∼15%) after the two low pH saline injections were excluded from the study and other eight animals were added to the experiment. The animals were tested 4 h after the second injection, as explained below.
Chronic pain model
Two injections with 100 µL of low pH preservative-free sterile 0.9% NaCl (pH 4.0) were administered on separate days in the left gastrocnemius when the animals were anesthetized briefly with halothane (2–4%). 6 It is a muscular and non-inflammatory pain model with long-lasting, widespread mechanical hyperalgesia production without motor deficits or significant tissue damage. There was no apparent mechanical hyperalgesia after the 1st intramuscular injection, therefore a 2nd injection was necessary after five days 6 as shown in Figure 1.
Animals from the SS were submitted to the same injections protocol, however with 100 µL of preservative-free sterile saline solution 0.9%.
WBV and low intensity exercise training
On the first day, the animals underwent habituation to the training and evaluation instruments. The platform and the treadmill were turned off and each animal was placed inside the specific cages for 10 and 30 min, respectively. On the following four days, to accustom the animal to walking, only the treadmill was turned and set to a speed of 3.05 m/min during 10 min.
The three different training groups started training 4 h after the 2nd injection with intramuscular acid. The groups were placed in separate cages.
To verify the frequency of the vibration platform, a 3D gyroscope (model 3DM-GX2, MicroStrain® Sensing Systems, USA) by a fast Fourier transform analysis was used. The amplitude of the equipment was determined through an ink pen attached to the platform at the cage position. The acceleration peak (aPeak) was calculated through the formula: D = aPeak/(2 × π2 × f 2), where “D” is the peak-to peak displacement and “f ” is the frequency. 29
WBV. The WBV training groups were subjected to WBV (TBS100A, Total Image Fitness®, Canada), on the vibrating platform for 10 days, 5 min on days one to five and 10 min on the other days. The vibration platform settings used for the protocol were 42 Hz, 2 mm peak-to-peak displacement, spiral mode, and peak acceleration, as a multiple of standard gravity, g ≈ 7.1g; they were chosen based on a pilot study with two rats in which, employing the same settings, the rats showed a greater decrease in mechanical hyperalgesia sensitivity after 10 min WBV exposure (compared with 20 and 30 Hz, also measured). The animals stood on a 3-mm foam pad (ethylene vinyl acetate) inside cages firmly attached to the platform.
Low intensity exercise training. Four hours after chronic pain induction (second injection), all animals underwent adaptation to a treadmill, originally designed for human use (Electronic Athletic, Athletic Runner®, Brazil), and adapted for use by rats. The 10-day exercise protocol consisted of placing the animal to walk on a treadmill set at a speed of 6.1 m/min for 15 min on the first five consecutive days and for 30 min on the other days. This low intensity exercise was adapted from the study of Bement and Sluka. 9
WBV + low intensity exercise training. Four hours after the chronic pain induction (second injection), all animals underwent adaptation to a treadmill. The 10-day exercise protocol consisted of two steps: first, for the first five consecutive days, placing the animal to walk on a treadmill set at a speed of 6.1 m/min for 15 min and combined with 5 min exposure to the WBV; second, for the next five days placing the animal to walk on a treadmill set at a speed of 6.1 m/min for 30 min combined with 10 min of WBV exposure, with the same settings already described for both machines.
Control groups (SS and PS) were placed on the treadmill or platform, for the same amount of time; however, the devices were turned off. Animals that were unable to walk on the treadmill were excluded from the experiment.
The sensitivity of the foot to mechanical and thermal hyperalgesia (hot pain) before versus after exposure to WBV were measured. The tests were carried out in a quiet room, with a controlled temperature between 20°C and 23°C.
Mechanical sensitivity
Mechanical sensitivity was measured with a calibrated pressure-meter (Electronic von Frey EFF 301, Insight®, Brazil). This is a hand-held force transducer fitted with a 1 mm2 polypropylene tip. The equipment reaction time is 1 ms and the transducer capacity is between 0.1 and 1000 g. The values are given in mV. The paw vertical elevation immediately upon removal of the testing tip was understood as a positive response. To confirm the response, the test was performed three times and the mean of the three values were determined. A trained examiner applied perpendicularly the tip to one of the five distal footpads and the pressure was increased gradually. A tilted mirror located below the grid, provides a clear view of the animal’s hind-paw. 30 Tests were performed by poking the hind-paw, provoking a flexion reflex, and a clear flinch response after paw withdrawal. The left paw stimulation continued until the rat showed three similar results (the difference between the maximum and the minimum result should be less than 10 g). 30 The electronic pressure-meter is one of the methods to measure mechanical allodynia, evaluating mechanical withdrawal threshold to a stimulus that is not normally unpleasant. 31 With the goal to increase data collection reliability, the sensitivity tests were applied by the same investigator before and immediately after the training, for the training groups.
Pain and thermal sensitivity
The Hot Plate device (DS37, Socrel®, Italy) measures the degree of sedation in relation to the time response. This test is widely used to study thermal (anti)nociception in rats and mice, since pain can only be estimated through their responses.
Each animal was individually placed on a hot plate (set at 52 ± 0.5°C) for a maximum of 20 s, 32 or until it displayed a nocifensive reaction of either hind-paw. The temperature of the hot plate was maintained constant. Each animal was only tested once until the presence of typical responses as hind-paw licking, shaking, and/or lifting. 33 The response latency time was manually recorded with a chronometer connected to the device with a pedal.
The same investigator measured the sensitivity tests to increase the reliability of the results. The temperature sensitivity was measured immediately after the mechanical sensitivity (about 40 minutes after training), for all groups.
Statistics
The control measurements were registered before exposure to WBV with the mean and the standard deviation calculation. Each animal’s specific control value was used to normalize data to decrease subject specific differences. Shapiro-Wilk’s test was used to test normal distribution of the changes in sensitivity in relation to the control group. Two-way repeated measures ANOVA was used to compare the pre- and post-condition on the same group, due to the parametric nature of the data. Two-factor mixed ANOVA compared the delta (difference between pre- and post-condition of each animal) between groups over time (during the 10 days of data collection).
Results
The sensitivity thresholds and time latencies for each animal were measured prior to any intervention and the mean values and the standard deviation (SD) were calculated.
Mechanical sensitivity
The mean values (±SD) for the pressure sensation were 36.1 (±5.4) mV for the left paw, under normal conditions.
In Figure 2, the vertical axis shows the rise in force required to produce a response to the pressure meter. A rise in force is equal to a decrease of mechanical (touch-pressure) sensitivity. Negative values represent hypersensitivity and positive values hyposensitivity. Considering subject differences from the control measurement (taken before application of the chronic pain model), the changes were calculated for each individual animal.
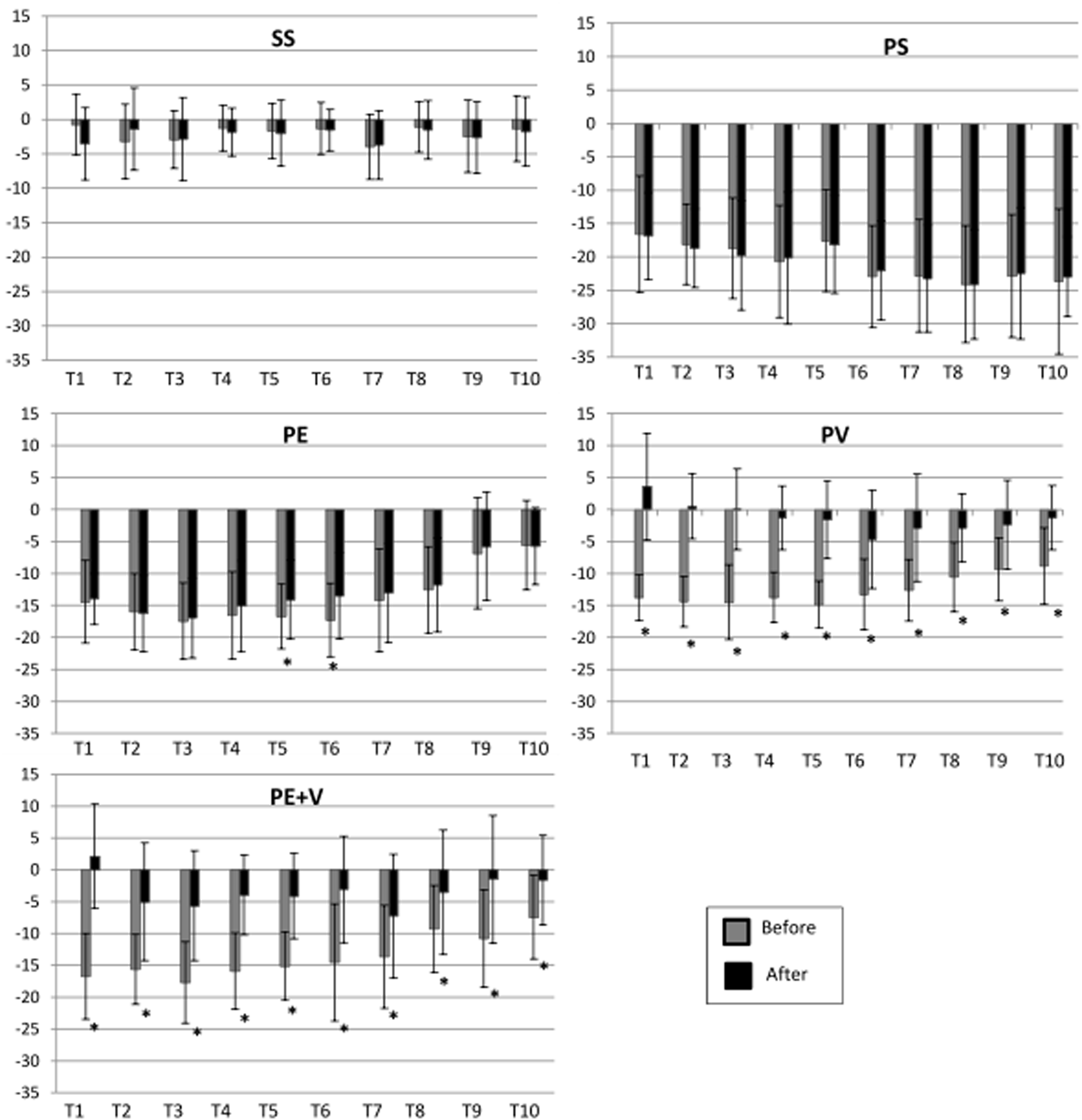
Mean and SD for the change in touch-pressure sensitivity force for the five groups with respect to the control condition (*P = 0.05). (SS) control saline sedentary group; (PS) control chronic pain sedentary group; (PE) chronic pain group treated with low intensity exercise; (PV) chronic pain group treated with whole body vibration; (PE + V) chronic pain group treated with whole body vibration plus vibration training. The values from the left paw were normalized by the baseline measurements (“before any procedures”) and individually for each animal (n = 60, 12 per group). The “y” axis represents the changes in touch-pressure sensitivity (mV); the “x” axis represents the training days 1 to 10 (T1 until T10).
In the SS, no significant differences for all comparisons were found between before and after “training” for the left paw during the 10 days (P > 0.05; Figure 2(a)). In the PS, no difference (P > 0.05) was found between before and after “training” considering the left paw, during the 10 days (Figure 2(b)).
Observing the chronic PE, following sessions 5 and 6, decreased mechanical sensitivity was found in the left paw (P < 0.05).
A significant loss of sensation after 5 or 10 min vibration exercise was found for mechanical sensitivity in the tested places of the left paw (between “before” and “after” treatment, mainly in the WBV groups. The left paw showed significantly decreased touch pressure sensitivity (P < 0.01) directly after WBV groups (Figure 2(d) and (e)) during the training days. It is interesting to note that, at around the 8th session, sensitivity starts approximating the control condition in all the treated groups.
PV and PE + V were significantly different of SS and PS over the 10 days of treatment (Figure 4(a)). Moreover, both groups PV and PE + V were significantly different of PE (Figure 4(a)).
Pain and thermal sensitivity
A significant change in thermal perception 40 min after WBV exposure was found mainly in the groups treated with vibration procedures (Figure 3).
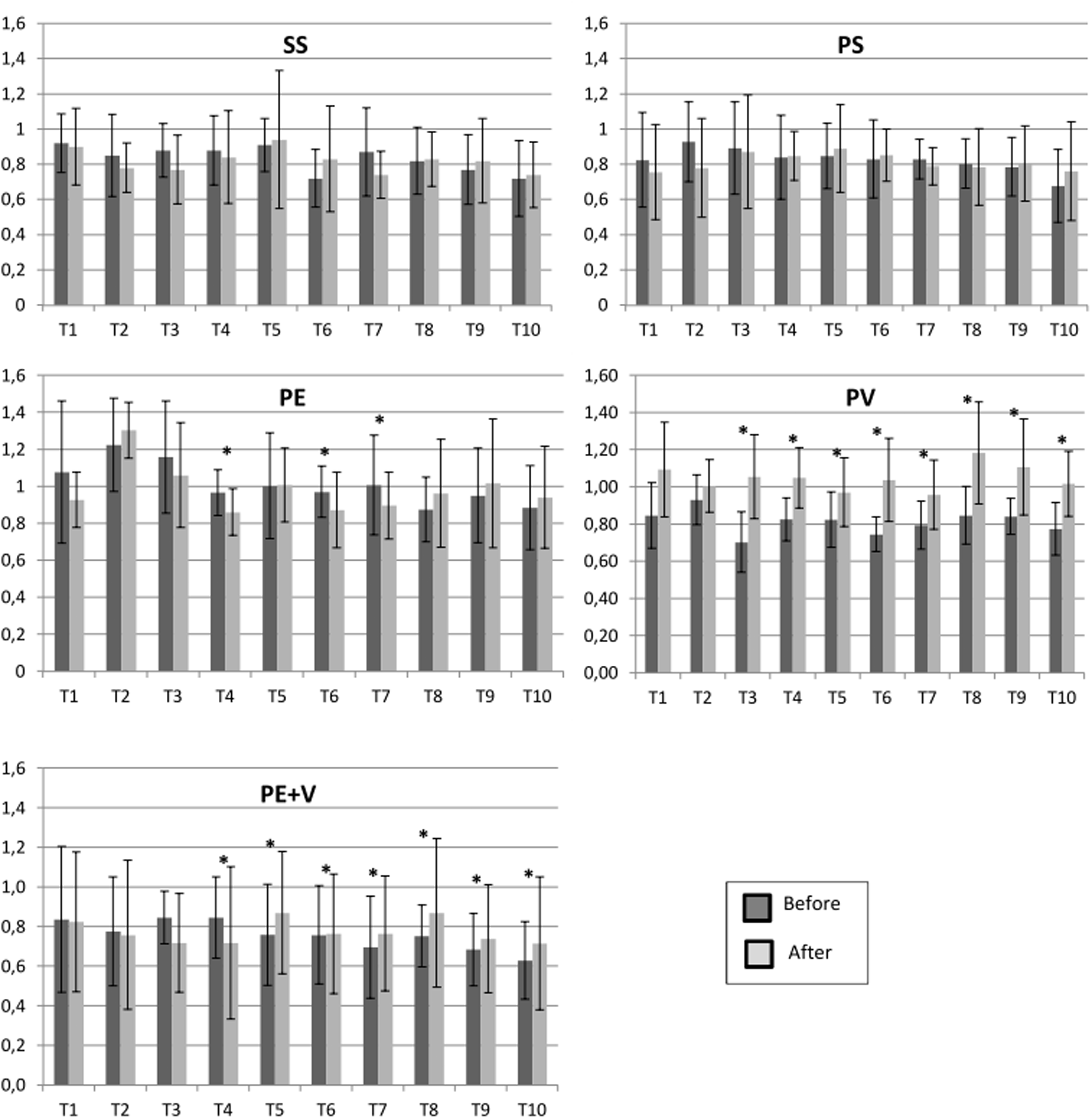
Mean and SD for all five groups. Time latency change in pain sensitivity (*P = 0.05). Y axis represents the normalized time latency (s) and X axis represents the training days T1–T10. The values were normalized by the baseline measurements (“before any procedures”) and individually for each animal. Hot plate measurement for the five different groups: control groups saline sedentary (SS) and chronic pain sedentary (PS), chronic pain groups treated with low intensity exercise (PE), vibration training (PV), and with low intensity exercise plus vibration training (PE + V; n = 60, 12 per group).
The low intensity exercise group presented increased thermal perception (latency time was shorter) in treatment sessions four, six, and seven. In the WBV only group, after the third treatment day, the time latency for thermal perception was significantly higher (P < 0.05; Figure 3, PV).
In the combined treatment (WBV and low intensity exercise) group, comparing ‘before’ and ‘after’ treatment, the latency was longer after the fourth session, i.e. the thermal perception decreased (Figure 3, PE + V).
The difference between all groups by time, pre- and post-treatment showed no significant results (P > 0.05) as Figure 4(b) shows.
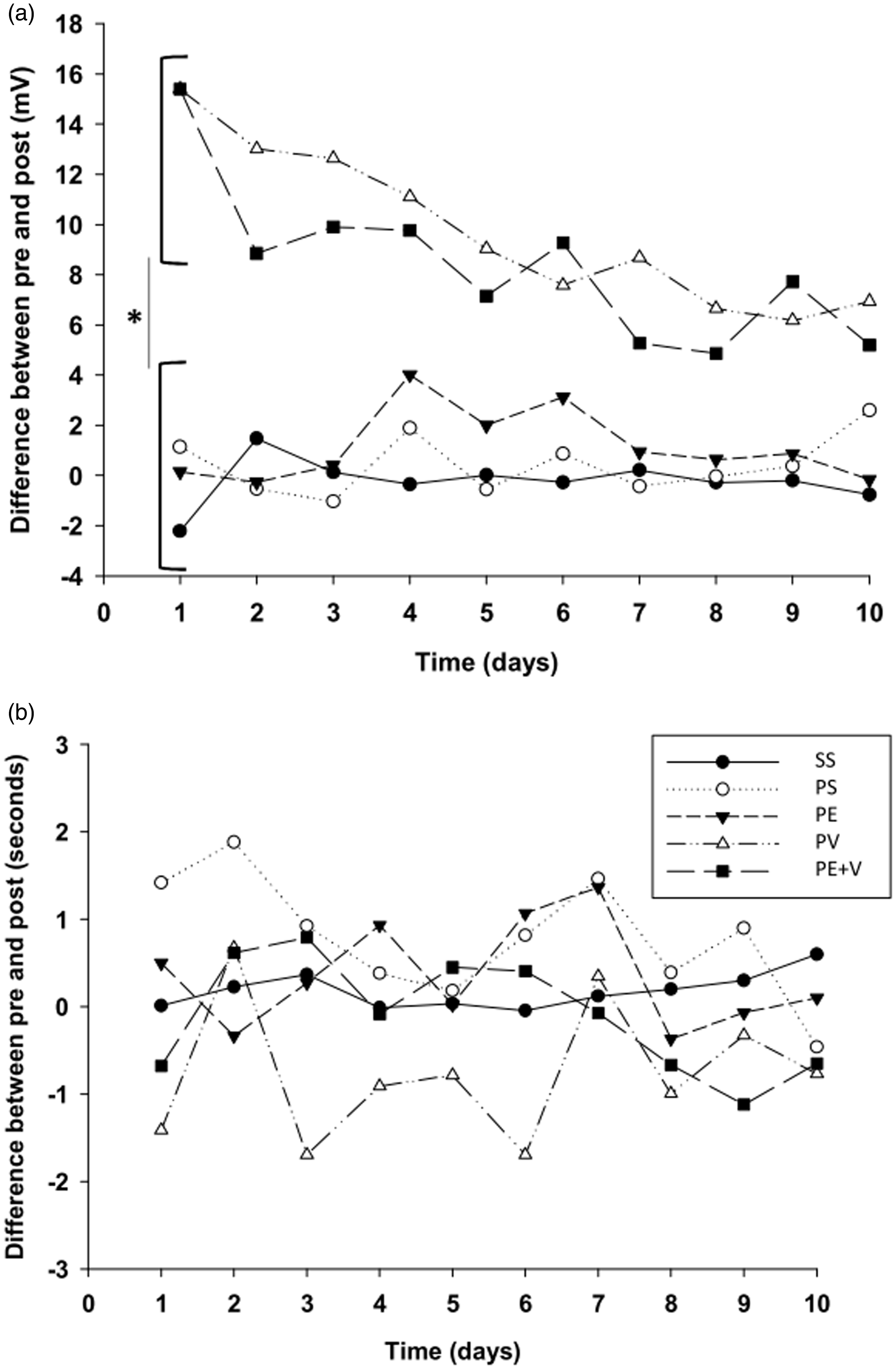
Mean values for the change in touch-pressure force (a) and in pain sensitivity time latency (b) for the five groups (*P < 0.05). Control saline sedentary group (SS); control chronic pain sedentary group (PS), n = 10; chronic pain group treated with low intensity exercise (PE); chronic pain group treated with whole body vibration (PV); chronic pain group treated with low intensity exercise plus vibration training (PE + V; n = 60, 12 per group).
Discussion
This study shows that for male rats exposed to a chronic pain model, 10 days of treatment with WBV led to decreased sensitivity to Aβ-fibers mediated by mechanical allodynia and C-fibers mediated by thermal stimulation (hot pain). After all the individual sessions, WBV decreased mechanical (touch-pressure) sensitivity and after the third session, the latency to pain perception was longer, mainly in the WBV groups. However, it is important to consider that during the first five sessions, the animals were exposed to only 5 min of WBV and 15 min of low-intensity exercise on the treadmill.
The exposure time used in this experiment is commonly used for performance enhancement or rehabilitation. Our results for mechanical sensitivity reduction are in agreement with studies conducted in humans 17,24,25 where, after a single WBV session, cutaneous sensitivity was significantly and temporarily impaired. A previous study 21 indicated that 10 min of local vibratory stimulus can affect the skin glabrous mechanoreceptive afferents, causing impaired perceptual and sensorimotor capacity for many minutes after vibration. Cutaneous receptors are highly sensitive to vibratory stimulus, which can influence the physiological messages. In most cases, the unit discharge in the mechanoreceptors is directly associated to the frequency of the vibration. 34 A decrease in mechanical sensitivity was found straight after both 5- and 10-min exposure to vibration. The force applied in order to the animals to perceive the von Frey was significantly greater after the WBV exposure.
A question arises as to whether loss of sensation might be useful. This investigation showed that touch-pressure mechanoreceptors and C-fibers are highly affected by vibration. In previous studies, the afferent discharge involving muscle spindles and fast adapting mechanoreceptors has been shown to be strongly affected by vibration.24–26 The touch pressure and vibration sensitivity that are transmitted by nerve fibers are related similarly to a muscle spindle single afferent Aα/Aβ-fibers. 35 Mechanical signals are carried for both and form a synaptic contact on inhibitory interneurons; this process produces a competition with the pain stimuli that reaches the projection neurons. It is possible to speculate that nerve fibers for mechanical and vibration sensitivity may also influence on the usual perception of stimulus quality as these fibers belong to the same category. Some findings indicate that Meissner corpuscles are multi-afferented receptor organs that would have nociceptive capabilities combined to being low threshold mechanoreceptors. 22
Mechanical vibration, in the large-diameter fiber systems, alters and attenuates the pain perception. 27 One hypothesis commonly used to explain the vibratory action is based on “Gate control theory of pain”, 23 according to which the dorsal horn of the spinal cord conducts the transmission of afferent neural signals to the higher centers where the pain is interpreted. The pain decrease caused by vibration might be explained by the large amount of Aα/Aβ-fibers, which are activated synchronously and thus stimulate the dorsal horn of the spinal cord. 28 The activation through vibration of low-threshold, large-diameter afferent Aβ-fibers (non-nociceptive), which synapse onto inhibitory (GABA-ergic or cholinergic) interneurons in the dorsal column of the spinal cord. Inhibitory neurotransmitters (e.g., GABA) are released by these interneurons, thus decreasing the excitability of second-order spinal neurons, so that consequent input from Aδ and C-fibers is attenuated. 27 Therefore, vibration could be used to decrease pain perception20,21 similarly to a transcutaneous electrical nerve stimulation (TENS). 36
Studies using passive vibration in humans20,36 showed the use of high frequency vibration directly to the location where the pain was perceived reduced the sensation of pain in about 70% of individuals with chronic and acute musculoskeletal pain. Furthermore, combined TENS with vibration could enhance the pain reduction effects. 36 Some authors have suggested that WBV training could reduce perceived pain in individuals with low back pain.21,37,38 In randomized controlled trials,37,39 pain relief was achieved following exercise on WBV platforms. It was speculated that eliciting muscles via stretch reflexes due to the generated instability, led to relaxation of the back muscles, thus decreasing pain perception. 37 We believe that the WBV was acting as local vibration, disturbing large-diameter fibers that reach projection neurons on the dorsal spinal column and, consequently, reducing the pain stimuli.
Patients with acute or chronic lower limb pain may benefit from a temporary reduction in their sensory capacity after WBV, prior to a rehabilitation session, without the use of drugs.28,40 This would allow them to perform exercises with less pain and greater range of motion. As a limitation of our study, biomarkers at the dorsal root ganglion that are involved in nociception were not analyzed. Future studies will focus on substance P, serotonin, and calcitonin gene-related peptide expression after WBV sessions in the dorsal root ganglion corresponding to lower lumbar spinal cord segments in a chronic pain model.
In conclusion, in rats subjected to a chronic pain model, the afferent discharges from touch-pressure mechanoreceptors were highly influenced by vibratory stimulation after each treatment session with WBV. Sensitivity to mechanical (touch-pressure) and thermal (hot pain) stimulation is impaired after WBV exercise; however, the thermal sensitivity decrease after WBV was not confirmed since differences between groups were not found.
In therapeutic interventions, when hypersensitivity in the lower legs negatively affects an exercise session, a reduction in sensitivity and the consequent reduction in pain might be helpful. Rehabilitation programmes can benefit from knowledge about the correct parameters of the exposure to WBV.
Footnotes
AUTHORS’ CONTRIBUTIONS
The conceptualization was conducted by AS, MZ, and MA. AS, LS, LRO, DCSC, and MBF contributed to the formal analysis of the article. The investigation was conducted by AS. MA contributed the resources. The original draft was written and prepared by AS. AS and LS performed the statistics. The article reviews and writing were conducted by AS, LS, and LRO. LS, LRO, DCSC, and MBF contributed to the visualization. MZ and MA supervised the study. The project administration was conducted by AS. All authors have read and agreed to the published version of the manuscript.
ACKNOWLEDGEMENTS
We acknowledge Total Image Fitness®, Canada, for donating the WBV equipment and the technical support of Silvia Barbosa, Otávio Américo Augustin and Marília Marques.
DECLARATION OF CONFLICTING INTERESTS
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES) [Finance Code 001] and National Council for Scientific and Technological Development (CNPq).