
Abstract
The effects of exercise on stress fracture risk are paradoxical. Exercise can promote both bone formation and resorption, which in turn, can reduce and increase risk of stress fractures, respectively. We review classic and current literature that suggests that the processes that underlie these responses to exercise are distinct. Bone remodeling involves osteoclastic resorption of fatigue-damaged bone, coupled with subsequent bone deposition to replace the damaged tissue. Bone modeling involves the independent action of osteoblasts and osteoclasts forming or resorbing bone, respectively, on a surface. In the formation mode, modeling results in increased bone stiffness, strength, and resistance to fatigue. Both the remodeling and modeling responses to exercise require significant time for newly deposited bone to fully mineralize. We propose that recognizing these two distinct physiologic pathways and their related time courses reveals the theoretical basis to guide exercise prescription to promote bone health during periods of heightened stress fracture risk. Such guidance may include minimizing rapid increases in the duration of repetitive exercises that may cause fatigue damage accrual, such as long-distance running and marching. Rather, limiting initial exercise characteristics to those known to stimulate bone formation, such as short-duration, moderate-to-high impact, dynamic, and multidirectional activities with rest insertion, may increase the fatigue resistance of bone and consequently minimize stress fracture risk.
Impact Statement
The role of exercise in the pathophysiology of stress fracture is seemingly paradoxical because exercise can simultaneously result in a bone resorption response, which occurs in the short term to repair fatigue damage, and a formation response that makes bones stronger in the long term. These physiological processes, in turn, simultaneously increase and decrease the risk of stress fracture, respectively. Much of the confusion in the field arises from attributing bone metabolic responses to exercise solely to the process of bone remodeling. In this minireview, we review classic and current literature that proposes that bone remodeling serves to repair fatigue damage that occurs with exercise, while a distinct mechanism called bone formation modeling serves to form bone in response to exercise, independent of prior resorption. Recognition of these distinct physiologic pathways helps move the field forward by revealing straightforward practical strategies for exercise prescription to prevent stress fractures.
Introduction
The responses of bone to exercise are paradoxical in that they include both bone resorption and formation. Resorption and formation after exercise are often erroneously attributed solely to bone remodeling – a process that begins with focal osteoclastic resorption, followed by osteoblastic bone deposition within a basic multicellular unit (BMU). As we propose in this article, classic and current literature suggest that a fundamental flaw in this focus is that bone functional adaptation in response to increased mechanical loading through remodeling would require resorption prior to deposition within each BMU. Bone resorption as a prerequisite to formation is inefficient, would require extensive time for adaptation, and initial resorption would leave bone transiently weaker and less resilient to successive exercise bouts.
In this minireview, we emphasize two separate physiologic processes that are responsible for the response of bone to exercise, instead of focusing solely on bone remodeling. Specifically, we propose that bone formation in response to exercise is largely an adaptive bone formation modeling response.1 –3 In bone formation modeling, formation is altogether independent of resorption, which means novel formation of bone does not require prior resorption.1,4 Bone remodeling in response to increased mechanical loading can be at least partially attributed to the repair of fatigue damage, which would require resorption of bone prior to deposition. Appreciating the independent physiologic phenomena underlying the distinct processes of bone remodeling and modeling provides the theoretical concepts for exercise prescription to prevent stress fractures – a problem that still plagues military recruits and endurance athletes nearly a century and a half after these injuries were first recognized.5 –7
Bone remodeling and modeling in the pathophysiology of stress fractures
Stress fractures are bone tissue injuries that occur with repetitive mechanical loading. They are debilitating injuries that require time away from sport or military duty and, for military members, can result in separation from service. 8 They are common during periods of rapid increases in exercise duration and intensity such as seen during the initial months of military training 9 and at the beginning of a competitive athletic season. 10 The paradox that exercise can both contribute to and protect from stress fractures, and the practical significance of such observations, is explained with recognition of two distinct physiological responses of bone to exercise that can occur simultaneously – bone remodeling and modeling.
The role of remodeling in the pathophysiology of stress fractures
Bone deforms in response to mechanical loading from exercise. The measure of bone deformation, defined as a change in length divided by its original length, is termed, “strain” (Figure 1). Bone strain can lead to the generation of microscopic fatigue damage, or microdamage, in the form of linear microcracks or diffuse, sublamellar tissue damage (Figure 1, Remodeling Loop). 11 Accrual of this tissue damage can decrease bone stiffness, strength, and toughness and can eventually lead to failure of the bone, as was shown in racehorses.11,12 Fortunately, tissue damage in bone is targeted for removal through bone remodeling. 11 Specifically, osteocytes, which are the mechanosensitive resident cells in bone, 13 and their dendritic processes detect damage that disrupts the osteocyte syncytium and replaces it with healthy tissue through a process called targeted remodeling.14,15 Osteocyte apoptosis at damaged loci occurs within 24h of fatigue loading and microdamage induction.16 –18 Consequently, adjacent viable osteocytes within 100 and 300 µm of microcrack loci promote osteoclastogenesis by releasing vascular endothelial growth factor and receptor activator of NF-κB ligand (RANKL), as well as by downregulating RANKL’s decoy receptor, osteoprotegerin.19,20 These cytokines are necessary for initiating intracortical remodeling by promoting the osteoclast recruitment, proliferation, and differentiation necessary to resorb the damaged bone around the dead osteocytes. During targeted remodeling, osteoclasts resorb damaged bone within 10–14 days,17,21 with the removal of 40% of microdamage number density within 10 days. 17 This resorption of bone in targeted remodeling transiently increases intracortical porosity (Figure 1, Remodeling Loop).
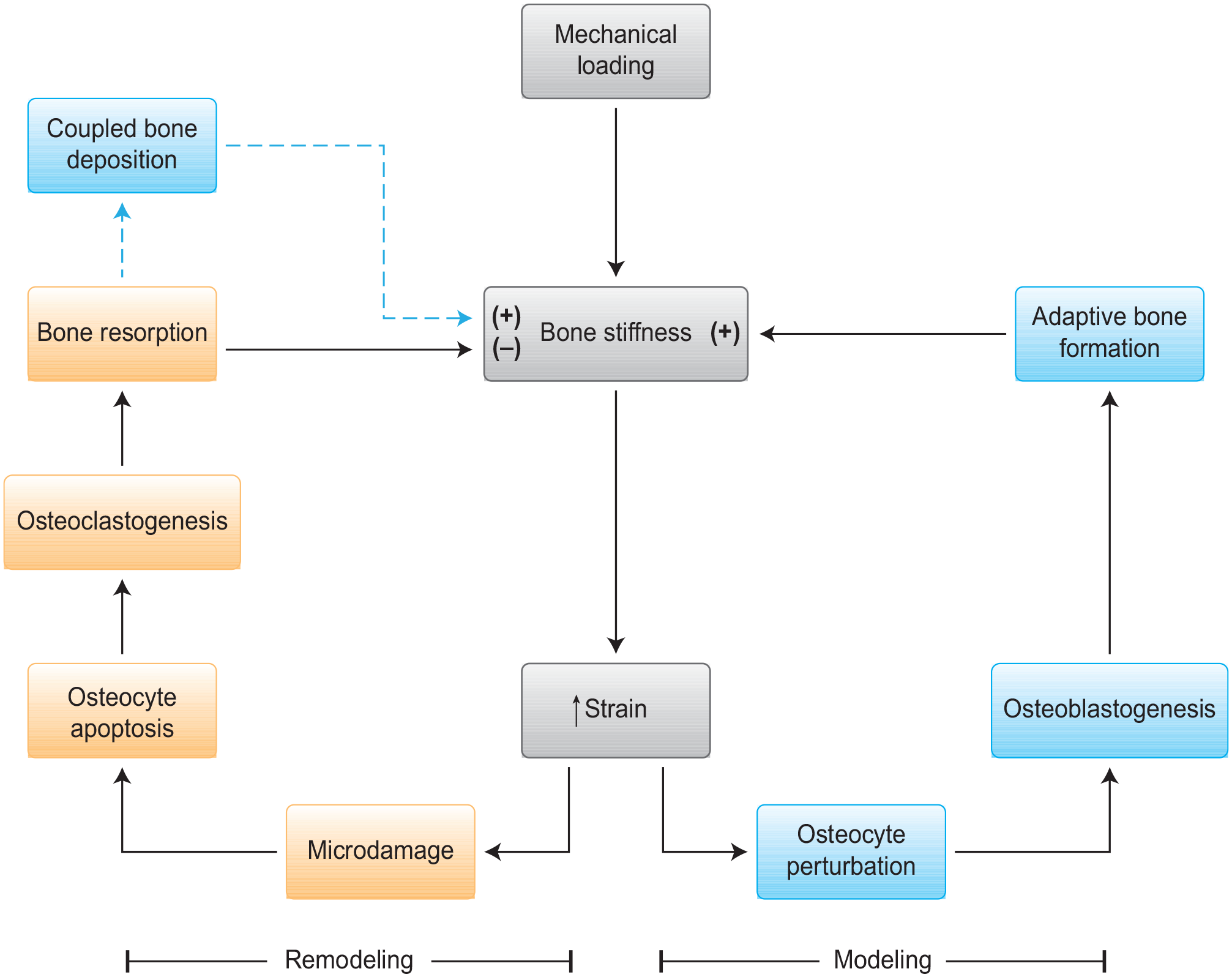
Mechanical loading paradox: Strains within bone tissue, generated by mechanical loading during exercise, can result in microdamage accrual and targeted remodeling that can temporarily decrease the stiffness and further resistance to microdamage in a positive feedback manner that could ultimately lead to stress fracture (Remodeling Loop). Paradoxically, the same strains from mechanical loading stimulate an adaptive bone formation modeling response that can increase bone stiffness in a manner that improves the fatigue resistance of bone and therefore may reduce risk of stress fractures (Modeling Loop).
Over time, osteoblast activity at the remodeling site promotes deposition of new bone to replace fatigue-damaged tissue (Figure 1, Remodeling Loop).21,22 However, mineralization of the newly deposited matrix occurs gradually, spanning weeks to months. 23 Thus, the initial increase in porosity can result in stress concentrations and decreased bone stiffness and strength24,25 requiring months to a year until mechanical competence is restored (Figure 1, Remodeling Loop). 26
Hence, the bone remodeling response to exercise is perplexing in that it is necessary to prevent stress fractures through microdamage repair, but also promotes stress fracture by leaving bones more porous and at a mechanical disadvantage, at least transiently. 27 Because of the important role remodeling plays in replacing fatigue damage with healthy bone, solutions for stress fracture prevention could focus on not only preventing generation and accrual of fatigue damage, but also on promoting the other mechanoadaptive response to exercise – bone modeling.
The role of modeling in the pathophysiology of stress fractures
Fortunately, the same strains that induce microdamage can simultaneously promote adaptive bone formation modeling (Figure 1, Modeling Loop). Mechanical loading sensed by osteocytes initiates this protective modeling response. Osteocytes translate mechanical stimuli into biochemical signals that alter gene and protein expression in response to loading.13,28 –30 Perturbation of the osteocyte by direct strain or fluid flow shear stress during mechanical loading initiates intracellular calcium signaling and the secretion of pro-osteoblastic paracrine factors including prostaglandins, nitric oxide, insulin-like growth factor 1, and adenosine triphosphate.31,32 Mechanical loading of osteocytes also suppresses secretion of negative regulators of bone formation, including sclerostin and dickkopf-1.33,34 Osteocyte secretion of pro-osteoblastic factors and suppression of inhibitors of bone formation promote the osteoblast recruitment, proliferation, and differentiation necessary to stimulate bone formation (Figure 1, Modeling Loop). 35 This adaptive bone formation in response to heightened mechanical loading occurs as a result of osteoblast activity uncoupled from osteoclast activity1,36 and is therefore a bone modeling response. 1
De novo bone formation can occur on all surfaces of the bone, including trabecular, endocortical, and periosteal surfaces. In trabecular bone, mechanical loading has been shown to increase the thickness of existing trabecular elements.2,36 However, Increases in cortical thickness through formation at the diaphysis of long bones on the periosteal surfaces provide the greatest mechanical advantage.37 –40 This periosteal formation results in increased second moment of inertia (i.e., wider bones) and reduces subsequent strain, to promote bone that is likely more resistant to fatigue 41 and therefore less likely to incur a stress fracture.6,42 –45 In bone formation modeling, because formation occurs without prior resorption, a positive adaptive bone response can occur in a relatively short period. 46 For instance, in military recruits, appreciable bone formation following novel physical training can be observed in as little as 8 weeks. 47
In summary, remodeling can be stimulated as a repair response that, although it can take months to a full year to complete, is necessary for replacing fatigue damage accrued with repetitive mechanical loading. While remodeling results in resorption in the short term, the final result of remodeling stimulated by fatigue damage repair is often no change in bone mass overall in healthy young people. By preventing accumulation of fatigue damage, this process is likely critical for maintaining the long-term health of the bone. Formation modeling, on the other hand, is the primary mechanoadaptive response of bone to exercise that confers substantial mechanical benefits that will then ideally prevent the generation of fatigue damage in the first place during exercise in the future, once the adaptation of the bone is fully completed. Stress fracture prevention strategies should leverage both of these physiologic pathways.
Practical implications for stress fracture prevention
Given the substantial time necessary to complete both remodeling and formation modeling, a practical implication of the model is that exercise conditioning regimens should be initiated as early as possible before high-risk periods for stress fractures to allow for both adaptive processes to conclude. For example, once a civilian has enlisted in the military, physical conditioning may only be protective from stress fracture if begun early enough to result in anabolic bone formation and conclusion of targeted remodeling. Other strategies for exercise prescription to offset risk of stress fracture include minimizing remodeling by limiting exercises with characteristics that promote accrual of fatigue damage and emphasizing exercises with characteristics that promote adaptive bone formation modeling.
Limiting exercise characteristics that promote accrual of fatigue damage
Avoiding fatigue damage is a straightforward way to prevent the positive feedback loop of targeted remodeling (Figure 2). As reviewed, physiological strains generated during mechanical loading cause fatigue damage.27,49 Besides the magnitude of strain, the rate at which peak strains are achieved, or strain rate, can also influence the generation of microdamage. 50 Strain magnitudes and rates are inherently linked during physical activity. For example, higher peak tibial bone strain magnitudes and rates are associated with running (~900 µε compressive strain magnitude, ~27,000 µε/sec compressive strain rate) compared with walking (~550 µε compressive strain magnitude, ~7,000 µε/s compressive strain rate). 51 In turn, higher strain characteristics, especially strain rates, result in greater accumulation of microdamage and loss of bone stiffness. 50 From a practical standpoint, these observations suggest that higher intensity, dynamic exercises, such as zigzag, up and down hill running, 51 may lead to a greater amount of microdamage accrual than lower intensity and less dynamic exercises.
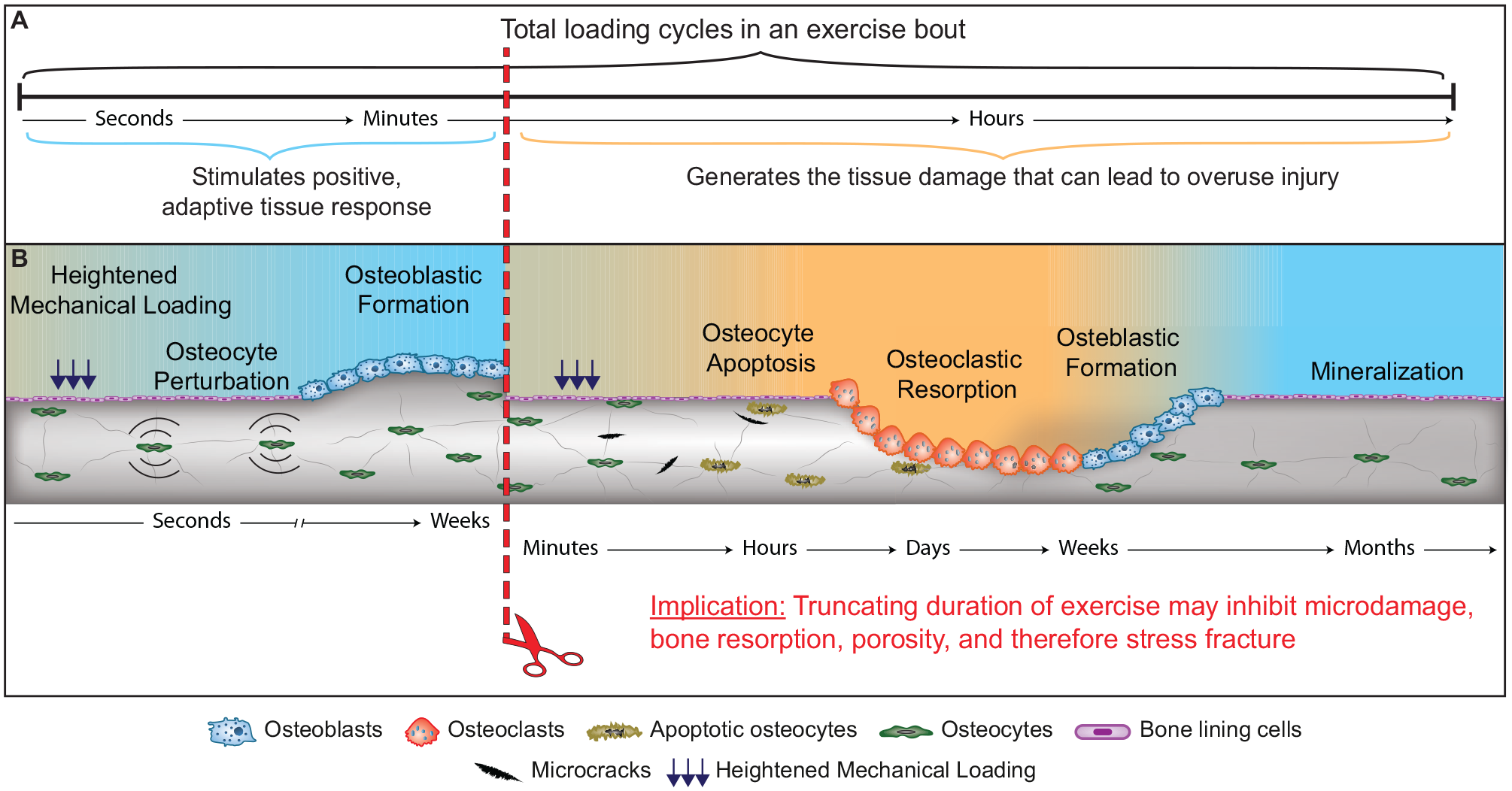
Implications of the mechanical loading paradox: Only the first few cycles of exercise result in an adaptive bone formation response. Continued exercise and increasing exposure to repetitive loading may not add benefits and can induce microdamage and increase risk of stress fracture. Accordingly, the practical implication is that truncating the duration of exercise may inhibit this positive feedback loop that can lead to stress fracture while still preserving the positive adaptive bone formation response.
An important exercise characteristic that could be a key target for stress fracture prevention is the cumulative cycles of loading and overall duration of the exercise bout (Figure 2). Low strain magnitudes such as those that occur during habitual physical activity can also result in appreciable accumulation of fatigue damage and loss of bone stiffness.50,52 This suggests that longer durations of low intensity exercise may have mechanical consequences in terms of fatigue damage accrual. Limiting the duration of exercise may be advantageous for attenuating fatigue damage in part because muscular fatigue with long-duration exercise increases the strain magnitudes and rates experienced during exercise.49,53 In one study, strain magnitudes increased by 26% following a 2 km run and by 29% during a 40 km march, while strain rates increased by 13% after the run and 17% after the march. 53 These higher strain magnitudes coupled with long duration exercise may lead to further accrual of fatigue damage.
The concept of limiting exposure to long-duration exercise to reduce microdamage accrual holds relevance for military recruits, who have traditionally been exposed to substantial amounts of repetitive loading. In recruits from the Israeli Defense Forces (IDF), who suffered rates of stress fracture as high as 30%, it was estimated that by the fourth week of initial military training when stress fracture incidence was highest, the recruits had already walked, marched, or ran a total of 250 miles, or approximately 210,000 loading cycles. 54 When the IDF implemented new training requirements that promoted adequate sleep and lowered the cumulative marching distance allowed during training, stress fracture incidence decreased by 60%. 55 While the relative contribution of limiting the amount of marching cannot be separated from that of the sleep intervention, these results provide evidence that reducing the cumulative amount of repetitive loading exercises may reduce the incidence of stress fracture during times of heightened risk.
The potential benefits of lowering risk of stress fracture from limiting long duration repetitive loading must be balanced with consideration of the benefits of endurance training on cardiorespiratory fitness and self-efficacy56,57 – both of which may be important benefits in relatively new Soldiers. One potential solution to this problem may be to increase endurance in new recruits more slowly over the course of the first year rather than doing so more rapidly during initial military training. Alternatively, if aerobic conditioning exercises are introduced far enough in advance to initial military training to allow for completion of skeletal adaptation, then bones loaded during military training may be able to endure long duration exercises without being susceptible to stress fracture.
Maximizing exercise characteristics that promote adaptive bone formation modeling
In yet another paradox, some of the same exercise strain characteristics that promote microdamage are also important for promoting bone formation.46,58 Specifically, high strain magnitudes and rates are considered common characteristics of osteogenic, or bone forming, exercises. For instance, animal studies have shown that strain magnitude and bone formation exhibit a positive linear relationship.59,60 Other studies61,62 have demonstrated that bones respond with formation in response to dynamic loads only, with resorption observed as a result of static loading, 62 suggesting that strain rate is an important characteristic for inducing adaptive bone formation. Therefore, reducing strain magnitude and rate may not be an ideal strategy for stress fracture prevention because both characteristics are important for promoting increases in bone strength with exercise.
As reviewed, the conundrum that high strain magnitudes and rates can both introduce fatigue damage and result in adaptive bone formation might be solved by focusing instead on limiting exercise duration, particularly in the early stages of initial military training or at the beginning of a competitive athletic season. Such a strategy may not interfere with the osteogenic potential of exercise. This is because the osteogenic window is short, with the mechanosensitivity of bone decreasing appreciably after only a few loading cycles.63 –65 For example, an animal study demonstrated that 10 jumps per day over 8 weeks was nearly as osteogenic as 20 and 40 jumps per day, suggesting that the osteogenic potential decreases rapidly after exercise is initiated. 63 However, sensitivity of bone to exercise appears to be restored with limited recovery time. 66 Recovery periods as little as 14 s, and up to 8h, were shown to restore bone mechanosensitivity, and segmenting total exercise into discrete bouts improved the bone formation response to exercise in two rodent studies.66,67 These studies suggest that short-duration exercises and exercise with frequent rest periods may be important strategies for stress fracture prevention.
Besides limiting duration of repetitive exercise, participation in sports that involve multidirectional cutting movements and numerous accelerations and decelerations such as seen in ball sports like basketball, soccer, and volleyball, may confer benefits from adaptive bone formation modeling. Young adult women who participated in at least 2 years of recreational soccer were shown to have 19% greater estimates of breaking strength at the tibial diaphysis and 20–40% lower estimated strain magnitudes and strain rates during walking with load carriage compared with healthy controls.68,69 These studies suggest that exercises that include multidirectional loading hold promise for stress fracture prevention. This concept is supported by studies in the IDF, reporting reductions of over 50% in incidence of stress fractures in recruits who played ball sports in the 2 years leading up to initial military training relative to those who did not play ball sports. 70
Taken together, these studies in animals and humans collectively support the notion that to promote adaptive bone formation modeling and minimize fatigue damage, exercise should be as short in duration as practical, include recovery periods, and involve moderate-to-high intensity dynamic and multidirectional activities. While these concepts still require further prospective studies in humans to refine exercise guidelines, coaches and military leaders may want to apply these practical implications when designing conditioning regimens, particularly for individuals at high risk for stress fracture.
Summary
There are several paradoxes within the physiologic responses of bone to exercise, including that exercise promotes both a bone resorption response and a formation response. This phenomenon can be explained by the dual processes of bone targeted remodeling and formation modeling. Remodeling is necessary to repair fatigue damage generated during mechanical loading, and formation modeling is an efficient mechanism for improving bone stiffness and strength. Another perplexing observation is that bone remodeling may play a role in both stress fracture promotion and prevention through temporarily increasing porosity and repairing tissue damage, respectively. The practical significance of unraveling these paradoxes is that fatigue damage generation and accrual should be minimized to prevent the need for remodeling. This can be accomplished by avoiding rapid increases in training volume and limiting duration of training bouts, when possible, particularly during times of heightened risk for stress fracture. A final paradox is that moderate-to-high intensity and dynamic exercises generate fatigue damage but are also necessary to induce osteogenesis. The practical significance of these observations are that moderate-to-high intensity and dynamic exercises, particularly those that include multidirectional movements, should be included in conditioning programs to induce osteogenesis and extend the fatigue life of the bone. However, the duration of these exercises should be limited and rest periods included when practical. Appreciating the distinct physiologic pathways that underlie the responses of bone to exercise not only clarifies seemingly perplexing observations but also reveals straightforward, practical solutions for stress fracture prevention.
Footnotes
Acknowledgements
Research supports in part by appointments to the Postgraduate Research Participation Program funded by USARIEM and administered by Oak Ridge Institute for Science and Engineering (CMC and KLP). We would also like to acknowledge Dr Stefan Pasiakos for his thoughtful review.
Authors’ Contributions
All authors participated in the conceptual development and writing of the paper. CMC, JMH, and KIG contributed to the figure design.
Disclaimer
The opinions and assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the views of the US Army or of the US Department of Defense.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.