
Abstract
This study set out to investigate the clinical significance of serum tumor necrosis factor receptor-associated protein 1 (TRAP1) in diagnosing small cell lung cancer (SCLC) with different clinical stages, and to compare the diagnostic efficiency with neuron-specific enolase (NSE), carcinoembryonic antigen (CEA) and carbohydrate antigen 19-9 (CA19-9). Besides, to analyze the role of serum TRAP1 in tumor immunity. A total of 91 patients with SCLC, 99 patients with non–small cell lung cancer (NSCLC), 102 patients with pulmonary nodules (PN), and 75 healthy people were included. The concentrations of serum TRAP1 was detected by enzyme-linked immunosorbent assay (ELISA). NSE, CEA, and CA19-9 were detected by chemiluminescence. The results showed that level of TRAP1 in Group SCLC was lower than other three groups (P < 0.01), whereas NSE in SCLC was significantly higher than the others (P < 0.01), and the levels of CEA and CA19-9 were higher than healthy people and PN patients (P < 0.01). There was a significant difference in TRAP1 levels between patients with limited-stage disease SCLC (LD-SCLC) and extensive-stage disease SCLC (ED-SCLC) (P < 0.0001). The sensitivity and specificity of TRAP1 in diagnosing LD-SCLC were 0.964 and 0.560, respectively, and the area under the curve (AUC) was 0.819. The sensitivity and specificity in diagnosing ED-SCLC were 0.810 and 0.868, respectively, and the AUC was 0.933, which showed high diagnostic value. The AUC of these two groups can be increased to 0.946 and 0.947 in combination of four biomarkers, effectively improving the diagnosis rate of SCLC. Our findings have revealed that serum TRAP1 has high diagnostic value for SCLC and high diagnostic sensitivity for LD-SCLC. It is a potential biomarker for SCLC. Combined detection can effectively improve the diagnosis rate of SCLC. TRAP1 may be secreted into the circulation by mature immune cells and participates in tumor immunity as a carrier of tumor antigens.
Impact Statement
Tumor necrosis factor receptor-associated protein 1 (TRAP1) had been proved to have high diagnostic value for small cell lung cancer (SCLC), but it is unclear how the role of serum TRAP1 in tumor progression and tumor immunity is different from intracellular homologs. This research confirmed that serum TRAP1 level was negatively correlated with the clinical stages of SCLC patients and TRAP1 was more effective in diagnosing SCLC than neuron specific enolase (NSE), carcinoembryonic antigen (CEA), and CA19-9. These results imply that serum TRAP1 can be used for monitoring the tumor progression of early stages SCLC, evaluating the efficacy of anti-tumor drugs, predicting the recurrence of tumors, and detecting the spread of tumors. Moreover, we inferred TRAP1 may be secreted into the circulation by mature immune cells and participate in tumor immunity as a carrier of tumor antigens. Our findings will provide a theoretical basis for TRAP1 as a specific marker of SCLC.
Introduction
Lung cancer is a primary malignant tumor of the lung originating from the trachea, bronchial mucosa, or glands. Among male population, the incidence and mortality rates of lung cancer ranks first in all malignant tumors, and ranks second and first, respectively, in females. 1 Small cell lung cancer (SCLC) accounts for approximately 14% of lung cancer. It has the characteristics of short doubling time, early metastasis, and more than half of the patients are diagnosed as advanced. Hence, SCLC is considered the most malignant pathological subtype. 2 Serum tumor markers such as carcinoembryonic antigen (CEA), 3 neuron specific enolase (NSE) 4 and carbohydrate antigen 19-9 (CA19-9) 5 have been widely applied in the diagnosis of lung cancer, but there are few researches on SCLC specific markers. Therefore, novel biomarkers are urgently needed to enhance the diagnosis as well as improve prognosis of SCLC.
Tumor necrosis factor receptor-associated protein 1 (TRAP1), a member of the heat shock protein 90 (Hsp90) family, localizes to mitochondria and regulates metabolic transformation during tumorigenesis, leading to metabolic reprogramming and apoptosis evasion in cancer. 6 The research of Li et al. 7 showed that TRAP1 has high diagnostic value for SCLC, but it is unclear how the role of serum TRAP1 in tumor progression and tumor immunity is different from that of intracellular homologs. The purpose of this study was to evaluate the efficacy of serum TRAP1 in diagnosing SCLC patients with different clinical stages and the clinical significance of combining NSE, CEA, and CA19-9 detection. Besides, the possible role of serum TRAP1 in tumor immunity was discussed.
Materials and methods
General information
From July 2021 to July 2022, 190 patients with lung cancer were diagnosed in the Second Affiliated Hospital of Nanchang University, including 91 patients with small cell lung cancer (Group SCLC) and 99 patients with non–small cell lung cancer (Group NSCLC). Group NSCLC included 62 cases of lung adenocarcinoma, 26 cases of lung squamous cell carcinoma and 3 cases of large cell carcinoma. In addition, 102 patients with pulmonary nodules (Group PN) and 75 healthy people (Group NC) admitted at similar time were randomly selected. The inclusion criteria were as follows: (1) the newly treated patients had not undergone surgery, chemotherapy, or radiotherapy before; (2) clarify a diagnosis, and have complete clinical, imaging, and histopathological data; (3) patients denied other autoimmune diseases and other cancers; (4) the healthy volunteers in Group NC were excluded from pulmonary disease by CT examination. The exclusion criteria were as follows: (1) unknown tumor type or non-primary tumor; (2) combined with other lung diseases; (3) complicated with serious heart, kidney, liver as well as other system diseases, thyroid diseases blood and system diseases; (4) pregnant or breastfeeding. SCLC patients were grouped according to the American Veterans Administration (VA) staging standard: 8 limited-stage disease SCLC (Group LD-SCLC) was defined as stage I to III (Tany, Nany, M0), and 28 patients were included; extensive-stage disease SCLC (Group ED-SCLC) was defined as stage IV (Tany, Nany, M1a/b/c), and 63 patients were included. All participants were informed and signed informed consent.
Specimen collection
TRAP1 samples were collected by vacuum blood collection method and placed in a tube containing separation gel and coagulant. The specific process was fasting venous blood collection of 3.0 mL, centrifugation at 1026g/15 min, serum collection and stored at −80°C. NSE, CEA, and CA19-9 samples were also collected by vacuum blood collection method and placed in a tube without anticoagulant. The collection method was same as TRAP1.
Methods and instruments
TRAP1 (Shanghai Bohu Biotechnology Co., Ltd., China) was detected by enzyme-linked immunosorbent assay (ELISA). All operations were carried out according to the instructions, and blank control and standard control were established. Serum NSE, CEA and CA19-9 were detected by chemiluminescence method. The detection kits were provided by Siemens Medical Diagnostic Products Co., Ltd. in the United States. The detection instrument was ADVIA Centaur full-automatic chemiluminescence immunoanalyzer. The operation was strictly in accordance with the reagent instructions and the quality management standard documents of the Second Affiliated Hospital of Nanchang University.
Statistical analysis
SPSS 26.0 and GraphPad Prism 9.0 software were used for statistical analysis, and the test sample size was calculated by PASS 11.0. The One-sample Kolmogorov–Smirnov test was used for the data normality test. The measurement data were expressed as Median (P25–P75). Mann–Whitney U test was used for two independent samples, and Kruskal–Wallis H test was used for comparison of multiple independent samples. The counting data were expressed by the rate. The difference between groups was analyzed by χ2 test; Graphic production was performed by utilizing the GraphPad Prism. The receiver operator characteristic (ROC) curves were drawn and the area under the curve (AUC) was calculated. The cut-off corresponding to the maximum value of Youden’s Index was taken as the best clinical critical point for diagnosis. The diagnostic value of combined detection of tumor markers was evaluated by binary logistic regression analysis. P < 0.05 was considered significant in difference.
Results
Study population
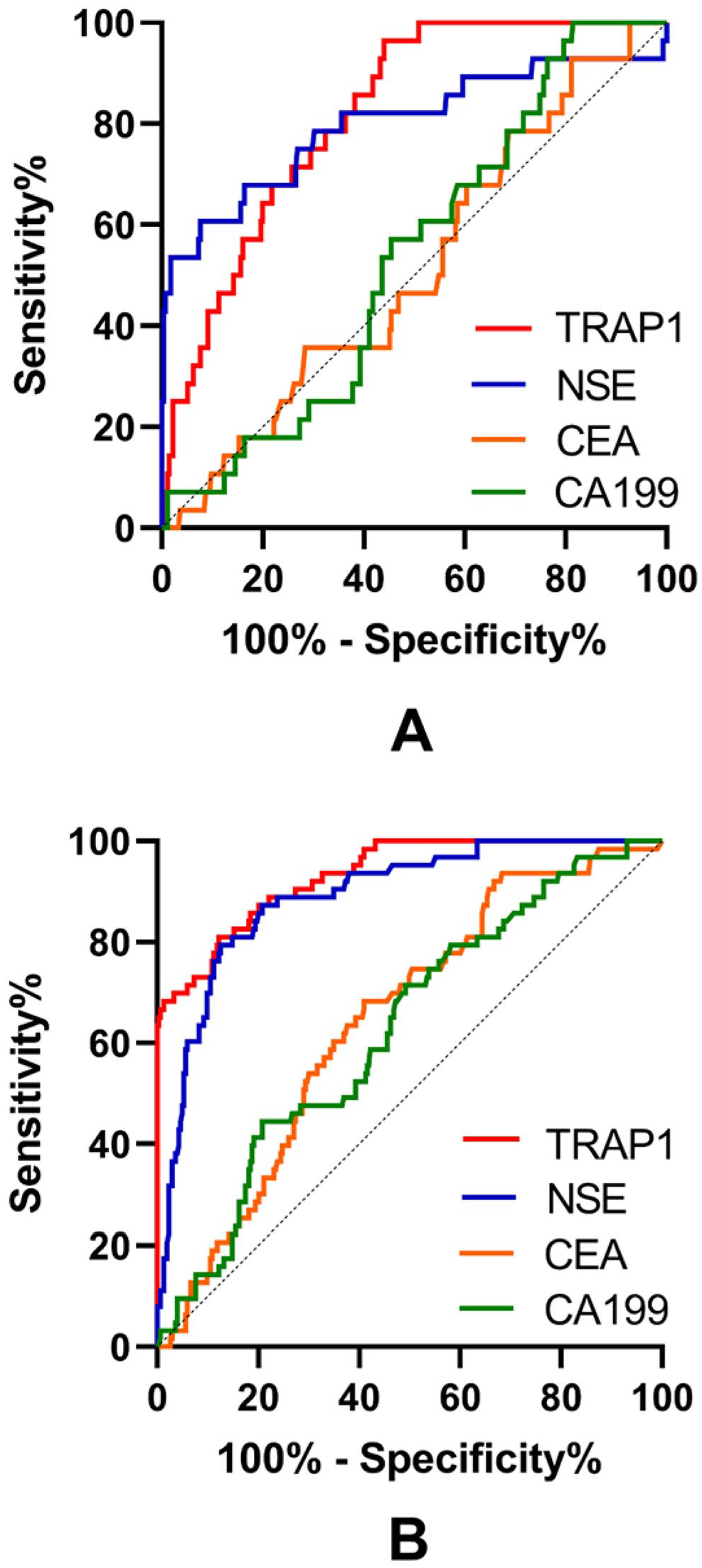
After χ2 test analysis, there was no significant difference in age and sex between the disease group and the control group (P > 0.05, Table 1).
Patient demographics.
NSCLC: non–small cell lung cancer; TNM: tumor node metastasis; VA: veterans administration; LD-SCLC: limited-stage disease—small cell lung cancer; ED-SCLC: extensive-stage disease—small cell lung cancer; PN: pulmonary nodules; NC: natural control.
P > 0.05.
Concentration of serum markers in each group
The single sample Kolmogorov–Smirnov test results showed that all the data of the four serum markers were biased. Therefore, non-parametric statistical methods were used for all data analysis.
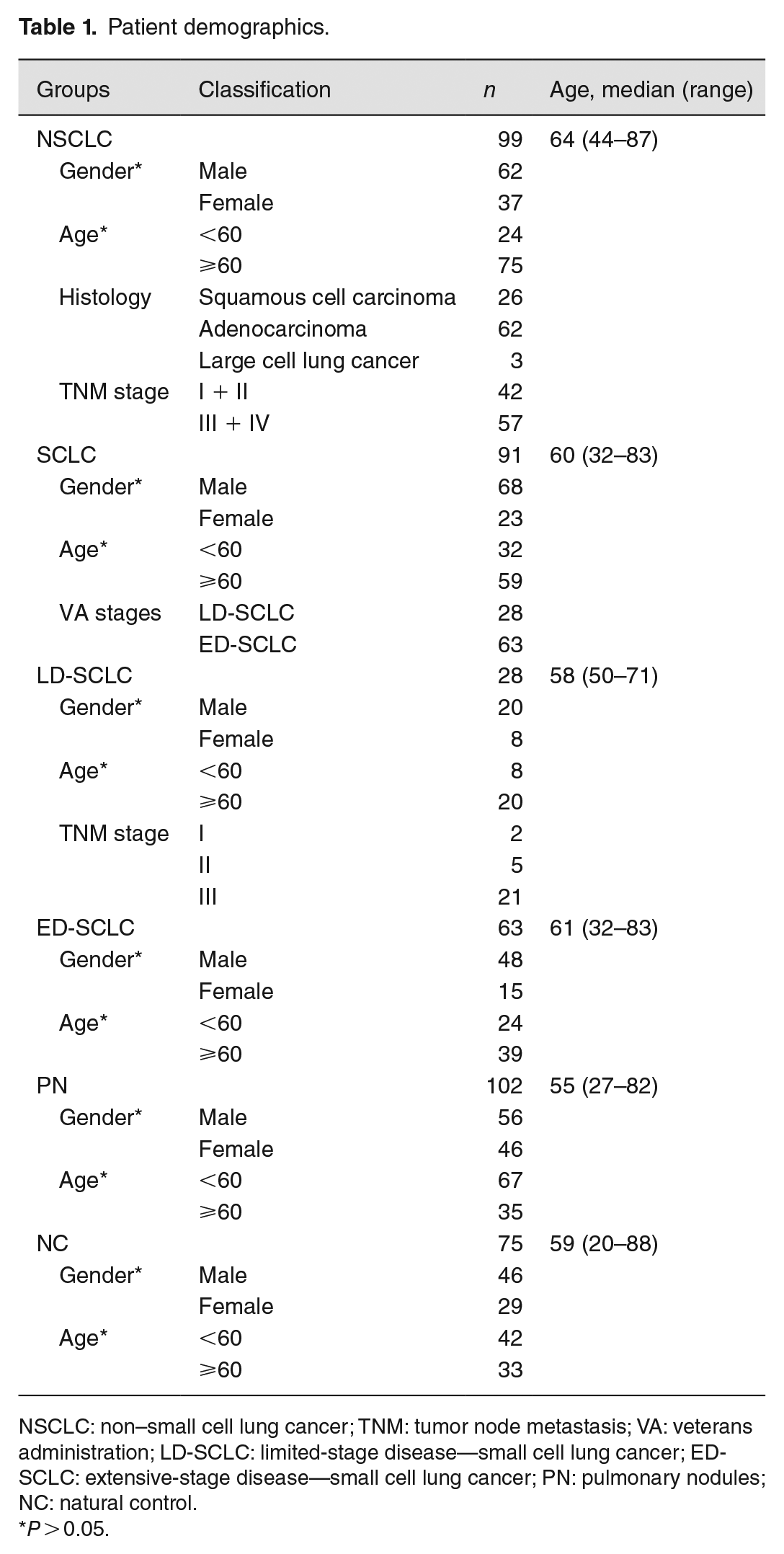
TRAP1 concentration in Group SCLC was 176.92 (78.78-259.78) pg/mL, which was significantly lower than that in other three groups (279.44 (252.04-300.92) pg/mL in Group NSCLC, 374.33 (330.97-508.10) pg/mL in Group PN, and 658.28 (459.17-1076.88) pg/mL in Group NC) (P < 0.01, Figure 1(A)). In Group SCLC, the concentration of NSE was significantly increased, reaching 14.11 (5.09-33.61) ng/mL, which was significantly higher than the other three groups (P < 0.01, Figure 1(B)). The level of CEA in Group SCLC was significantly lower than Group NSCLC, whereas slightly higher than Group NC and Group PN (P < 0.01, Figure 1(C)). The level distribution of CA19-9 was similar to CEA, since the level of CA19-9 in Group SCLC and Group NSCLC was significantly higher than that in Group PN and Group NC (P < 0.01, Figure 1(D)). The statistical difference between groups was examined by Kruskal–Wallis H test.
Expression levels of TRAP1 (A), NSE (B), CEA (C), and CA19-9 (D) in different disease groups and control groups. The level of TRAP1 in Group SCLC was lower than other three groups (P < 0.01), whereas NSE in SCLC was significantly higher than the others (P < 0.01), and the levels of CEA and CA19-9 were higher than healthy people and PN patients (P < 0.01).
Levels of serum biomarkers in different clinical stages of SCLC
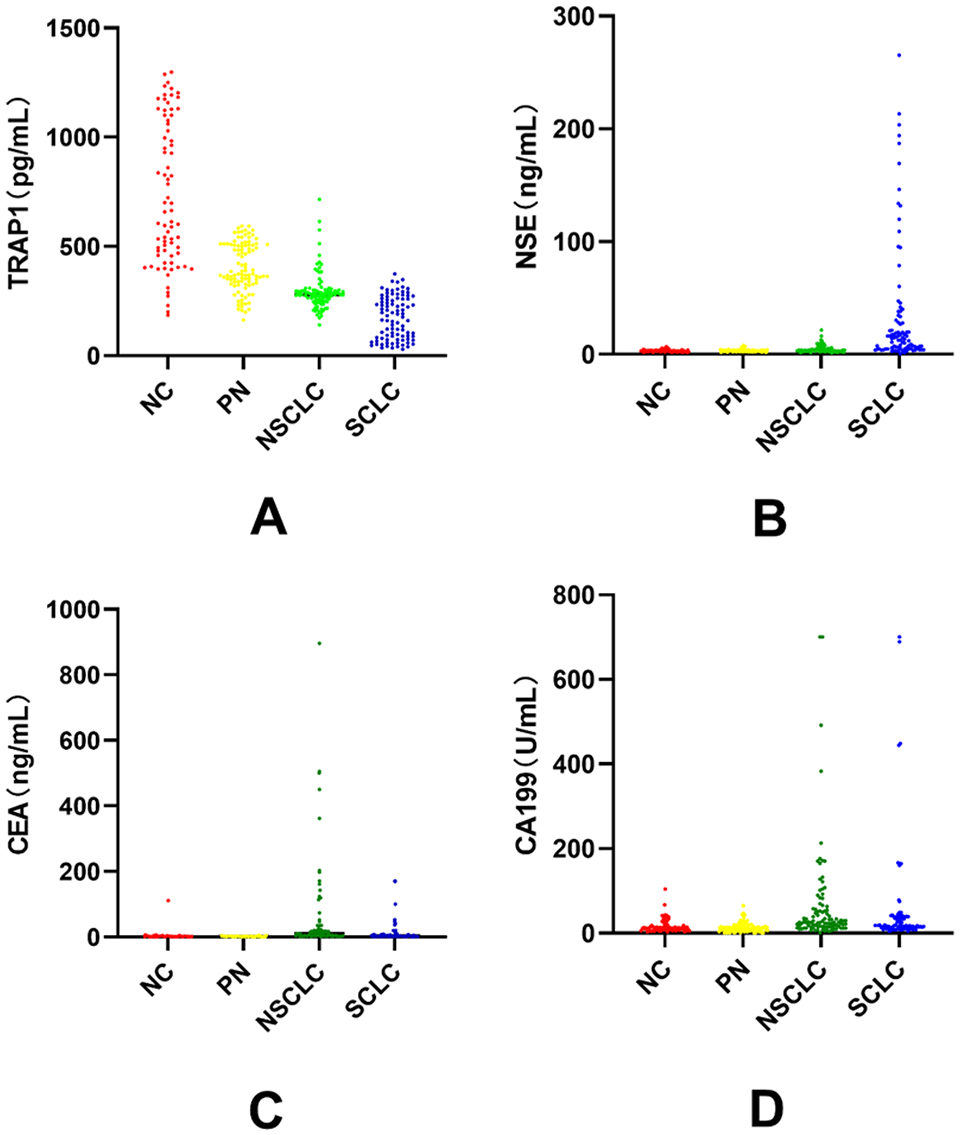
There were differences in the levels of four serum biomarkers between different SCLC clinical stages. The concentration of TRAP1 in Group LD-SCLC was 256.04 (200.09–291.91) pg/mL, which was significantly higher than that in Group ED-SCLC (104.10 (61.85–226.05) pg/ml), and the difference was statistically significant (P < 0.0001, Figure 2(A)); The CEA concentration of Group LD-SCLC was lower than Group ED-SCLC: LD-SCLC was 2.25 (1.36–3.90) ng/mL, and ED-SCLC was 4.35 (2.03–12.41) ng/mL (P < 0.01, Figure 2(C)). There was no statistical difference in NSE (P = 0.229, Figure 2(B)) and CA19-9 levels (P = 0.130, Figure 2(D)) between the two groups. The statistical difference between Group LD-SCLC and Group ED-SCLC was examined by Mann–Whitney U test.
Comparison of serum levels of TRAP1 (A), NSE (B), CEA (C), and CA19-9 (D) in peripheral blood of patients with LD-SCLC and ED-SCLC (plots were derived from data presented in Figure 1). There was a significant difference in TRAP1 levels between patients with limited-stage disease SCLC (LD-SCLC) and extensive-stage disease SCLC (ED-SCLC) (P < 0.0001).
Diagnostic value of TRAP1, NSE, CEA, and CA19-9 in different clinical stages SCLC
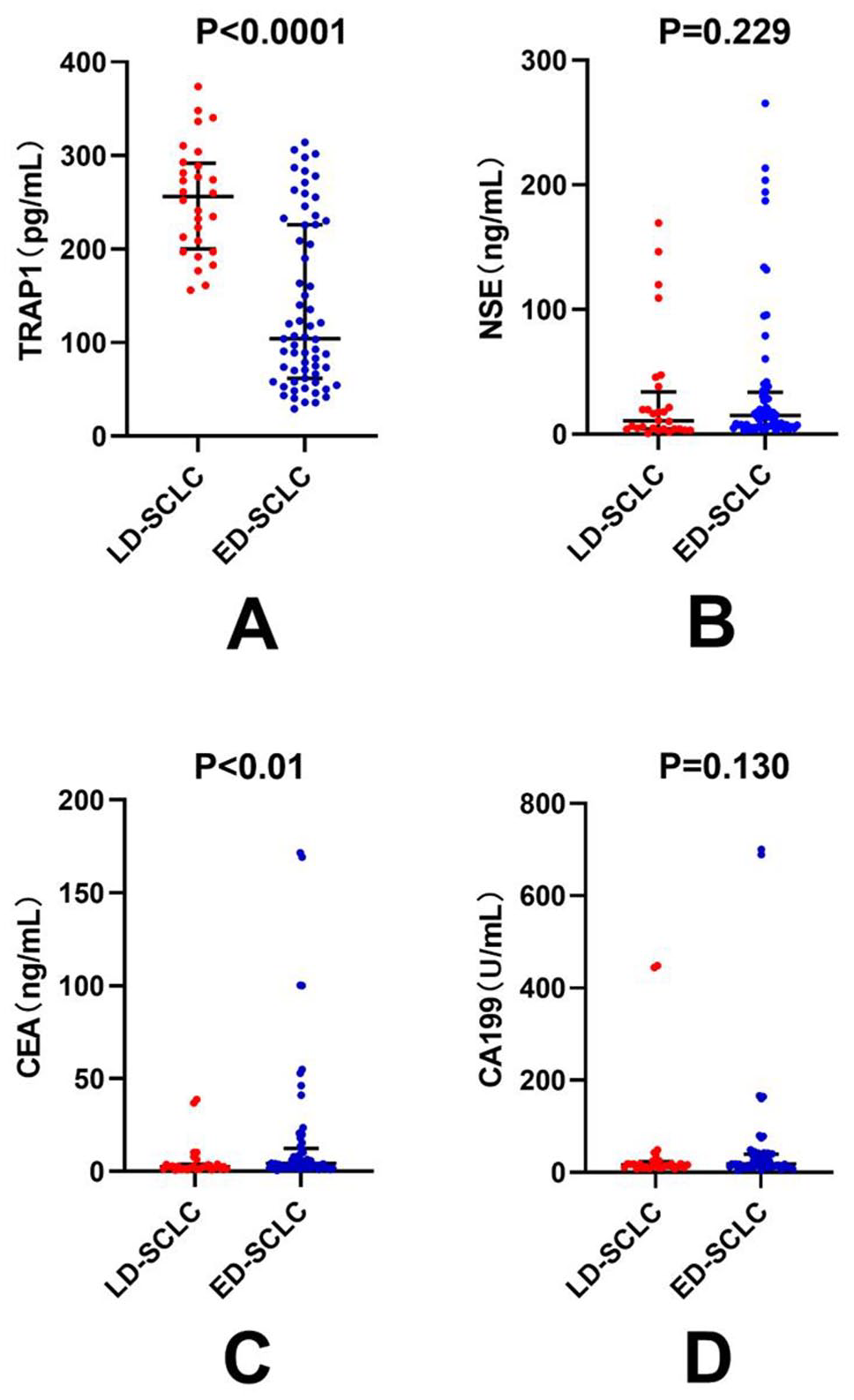
The ROC curves of LD-SCLC and ED-SCLC diagnosed by TRAP1, NSE, CEA and CA19-9 were drawn separately (Figure 3). As shown in Table 2, the AUC of four serum markers for LD-SCLC were 0.819, 0.800, 0.513, and 0.535, respectively; The AUC for ED-SCLC was 0.933, 0.891, 0.646, and 0.627, respectively. Among the single marker tests, TRAP1 had the highest diagnostic efficiency in both Group LD-SCLC and Group ED-SCLC. According to the maximum value of Youden’s index, the optimal cut-off values of TRAP1 for diagnosing LD-SCLC and ED-SCLC were 349.03 pg/mL (sensitivity = 0.964, specificity = 0.560) and 236.76 pg/mL (sensitivity = 0.810, specificity = 0.868), respectively. The AUC of TRAP1 combined with NSE in diagnosing LD-SCLC was 0.908 and that of ED-SCLC was 0.943. The combined detection of four tumor markers had the largest AUC, which was 0.946 and 0.947, respectively.
ROC curve of TRAP1, NSE, CEA, and CA19-9 in the diagnosis of LD-SCLC (A) and ED-SCLC (B). The AUC of TRAP1, NSE, CEA, and CA19-9 for LD-SCLC were 0.819, 0.800, 0.513, and 0.535, respectively. The AUC for ED-SCLC was 0.933, 0.891, 0.646, and 0.627, respectively. Among the single marker tests, TRAP1 had the highest diagnostic efficiency in both Group LD-SCLC and Group ED-SCLC.
Diagnostic efficiency of four serum tumor markers for SCLC at different clinical stages.
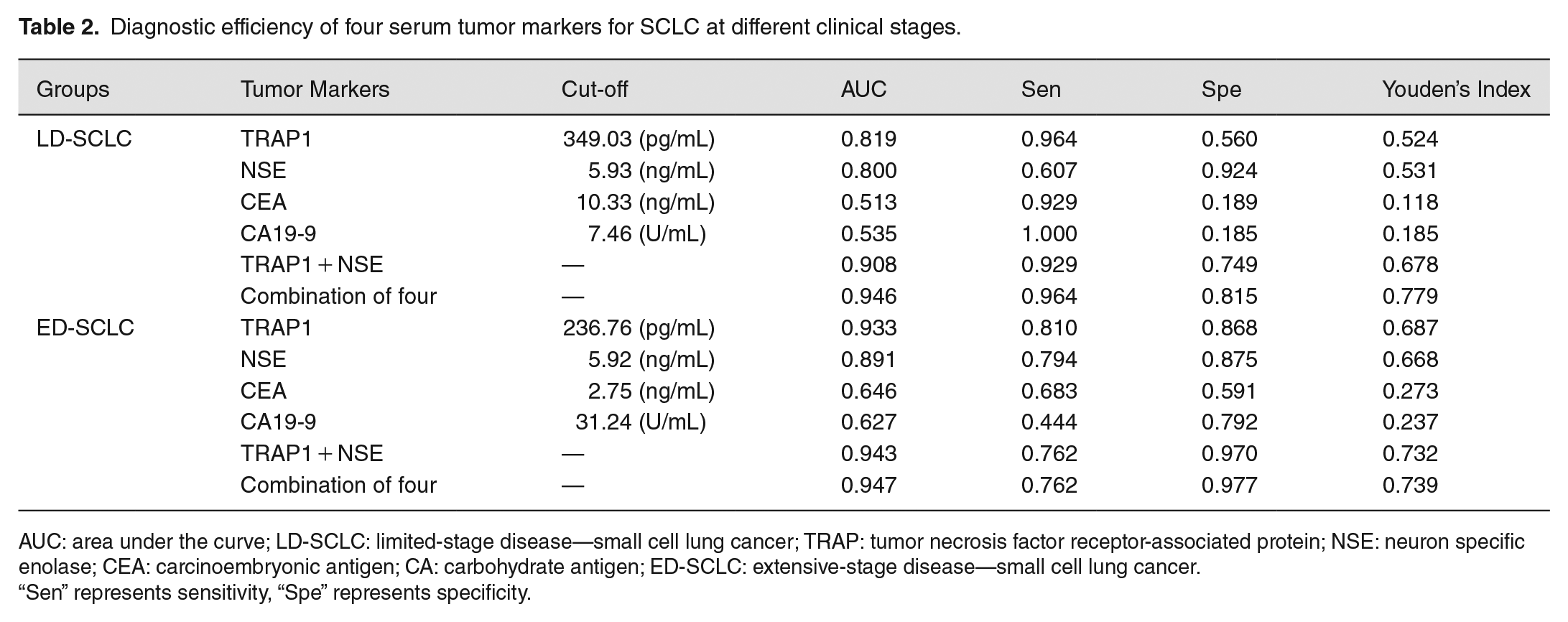
AUC: area under the curve; LD-SCLC: limited-stage disease—small cell lung cancer; TRAP: tumor necrosis factor receptor-associated protein; NSE: neuron specific enolase; CEA: carcinoembryonic antigen; CA: carbohydrate antigen; ED-SCLC: extensive-stage disease—small cell lung cancer.
“Sen” represents sensitivity, “Spe” represents specificity.
Discussion
SCLC is the most malignant subtype of lung cancer. 70% of the patients have metastasis at the time of diagnosis. The median survival period is less than 2 years, the 5-year survival rate is less than 7%, and the prognosis is extremely poor. 9 A study conducted in 2021 indicated that the 2-year survival rate of LD-SCLC patients has increased from 36% to 46% in the past 30 years. In contrast, the 2-year survival rate of ED-SCLC patients has hardly changed, from 7% to 8%. 10 Therefore, early diagnosis is of great significance for improving the prognosis of SCLC patients. Tumor marker detection is an effective detection method to improve the detection rate of lung cancer. Abnormal serum tumor markers levels can ferret out suspected lung cancer cases and serve as the basis for further pathological examination. At present, the majority of researches are focused on the relevant markers of NSCLC, while less on SCLC. TRAP1 is a mitochondrial specific Hsp90 family member and is ubiquitously expressed in all cells. Compared with normal cells, it is highly expressed in mitochondria isolated from tumor cells. 11 At the normal expression level, the role of TRAP1 is to regulate the content of reactive oxygen species (ROS) and calcium in mitochondria, control the function of electron transport chain, maintain the integrity of mitochondrial cristae and supervise the opening of permeability transition pore (PTP). As TRAP1 expression increase, mitochondria lose calcium sensitivity, ROS levels decrease, and prevent PTP opening, leading to metabolic reprogramming and apoptosis escape in cancer. Theoretically, given the high abundance of heat shock proteins (HSPs) in cancer and their molecular chaperone functions, they have the potential to become an ideal source of tumor antigens. 12 At present, many studies13 –15 have discussed the effect of TRAP1 expression in lung cancer tissues on the metabolism and proliferation of cancer cells. In terms of clinical diagnosis, TRAP1 has been proved to have high diagnostic value for SCLC. This current study focuses on the level changes of serum TRAP1 in SCLC patients with different clinical stages, and improves its clinical value by the combination of NSE, CEA, and CA19-9 as well as discusses the possible role of serum TRAP1 in tumor immunity for the first time.
TRAP1 level in Group SCLC was the lowest among the four groups and the highest in Group NC. Besides, the median concentration of TRAP1 in Group ED-SCLC was about half of that in Group LD-SCLC, which was negatively correlated with the clinical stage, consistent with the results of Li et al. 7 These results imply that serum TRAP1 can be used for differential diagnosis of SCLC, monitoring the tumor progression of LD-SCLC patients, evaluating the efficacy of anti-tumor drugs, predicting the recurrence of tumors, and detecting the spread of tumors. NSE mainly exists in neuroendocrine tissue, neural tissue and some tumor tissues of endocrine origin, and its content is extremely low in the serum of healthy people. It is considered as a high specific tumor marker of SCLC. 16 In our study, the serum NSE concentration of Group SCLC was significantly higher than that of the other three groups, which was consistent with the results of the same type of trials.17,18 There was no significant difference between ED-SCLC and LD-SCLC (P > 0.05), which was consistent with the findings of Wang et al., 19 but contrary to the findings of Wang et al. 20 and Li et al. 17 We consider it may be related to the TNM stage of the SCLC patients. Although SCLC patients of stages I–III were all defined as LD-SCLC, their serum NSE levels were not similar but positively correlated with the tumor progression. In our research, patients of stages III accounted for about 75% of LD-SCLC patients, whose NSE level was not much different from stages IV. Therefore, Mann–Whitney U test may not be able to verify the significant difference between Group LD-SCLC and Group ED-SCLC. CEA is an acidic glycoprotein with the characteristics of human embryonic antigen extracted from colon cancer and embryonic tissue. It is mainly used to characterize lung adenocarcinoma and SCLC in the auxiliary diagnosis of lung cancer. 21 Our results show that the CEA level of SCLC is significantly lower than NSCLC, but slightly higher than that of NC and PN. It is directly related to the ultra-high level of serum CEA of lung adenocarcinoma patients in Group NSCLC, which is consistent with the results of the same type of studies. 22 We observed that the CEA level in ED-SCLC was higher than LD-SCLC, which was consistent with the findings of Li et al., 17 indicating that CEA is expected to be a serological indicator for monitoring the progression of SCLC tumors as well. CA19-9 is a mucosal glycoprotein and a representative biomarker of pancreatic cancer. 23 Studies have reported that serum CA19-9 level of lung cancer patients will also increase. 5 In this study, the level of CA19-9 was significantly increased in NSCLC and SCLC, but there was no statistical difference between LD-SCLC and ED-SCLC. In addition, the level of CA19-9 also increases in many benign diseases such as chronic pancreatitis, interstitial pneumonia, and bronchiectasis, causing false positive diagnosis of lung cancer. 24 It is generally believed that the clinical value of CA19-9 in diagnosing SCLC is limited.
Liquid biopsy is considered as a non-invasive alternative to tissue biopsy, which requires only a small amount of body fluid (such as blood) to provide advanced diagnostic information. The efficiency of serum markers in diagnosing LD-SCLC represents the ability to detect tumors in early stages, while AUC is considered as a quantitative measure of differential diagnostic ability. When the cut-off value is 349.03 pg/mL, TRAP1 has the highest AUC (AUC = 0.819) and the highest sensitivity (Sen = 0.964) among the four markers. It has medium diagnostic value for LD-SCLC as well as a good indicator for early screening. NSE has higher specificity and has medium diagnostic value for LD-SCLC. The AUC can be increased to 0.908 by combining the two biomarkers. The accuracy of CEA and CA19-9 in diagnosing LD-SCLC is low, and they don’t have clinical diagnostic value when tested alone. However, through combined detection with TRAP1 and NSE, the AUC can be increased to 0.946, which can effectively make up for the diagnostic specificity of TRAP1 and greatly improve the detection rate. Due to the characteristics of early metastasis in SCLC, the efficiency in the diagnosis of ED-SCLC has more practical clinical significance. Compared with LD-SCLC, the Youden’s index of ED-SCLC diagnosed by the four markers was improved. When the cut-off is 236.76 pg/mL, the AUC of TRAP1 in diagnosing ED-SCLC is 0.933, the sensitivity is 0.810, and the specificity is as high as 0.868. TRAP1 can distinguish SCLC from NSCLC and benign space occupying lesions in the lung, and its performance is superior to the other three markers. NSE still has the highest specificity (Spe = 0.875) among the four items and AUC (AUC = 0.891), showing high diagnostic value. The AUC of CEA and CA19-9 were less than 0.65, as a result, their diagnostic values were low. Although the combined detection can improve the specificity of TRAP1 within limits, the AUC is only increased by 0.01, whereas the sensitivity of diagnosis will be reduced and the missed diagnosis rate will be increased. Therefore, it is necessary to adjust the strategy of combined diagnosis according to the needs of diagnosis. Further studies in the future are needed, to evaluate the diagnostic value of TRAP1 in a wider population, for example, SCLC patients in different regions, race and a larger sample size were included.
The role of serum TRAP1 in tumor immunity hasn’t been discussed. Our results show that the serum TRAP1 content of Group NC is about four times to Group SCLC, which has a great difference between the two groups. However, Lee et al. 25 found that TRAP1 was strongly expressed in SCLC tumor pathological specimens by immunohistochemical staining, and the positive rate up to 100%, which was much higher than surrounding tissues. This seemingly contradictory result may be related to the different functions of TRAP1 in tissues and extracellular. Mitochondrial TRAP1 is upregulated in the cellular stress response caused by heat, hypoxia and nutrient deficiency, which is essential for the survival of tumor tissues in the harsh microenvironment, because it allows the persistence of unstable amino acid sequences and accelerates the energy metabolism of tumor cells by promoting the Warburg effect, thus driving tumor malignant proliferation. 26 Some studies have reported that heat shock can increase the expression of TRAP1 by 200 folds. 27
Although there is little direct evidence on the origin and biological function of TRAP1 in serum, the immunological function of circulating HSPs have been reported widely. HSPs are usually released from tissues into body fluids in the form of free form or membrane-bound particles 28 in the case of cell/tissue stress, injury, cell death, hypoxia in cancer progression, and various other pathological conditions. Therefore, they are called alarmins, damage-associated molecular patterns (DAMP) or tumor associated antigens (TAAs). 29 The existing forms of extracellular HSPs in body fluids include free proteins, protein complexes, ribonucleoprotein (RNP) complexes, vesicle surface bound HSPs, membrane-bound HSPs, or HSPs rich extracellular vesicles (EVs), such as exosomes and oncosomes. 30 Intriguingly, a lot of studies have identified mitochondrial proteins are secreted as EVs cargo, which act as communication devices between cells.31 –33 It has been proved that TRAP1 can be secreted from tumor cells in the form of exosomes. 34 In addition, Calderwood et al. 28 reported that many types of HSPs, including Hsp90, are secreted from a variety of cells, and speculated that they may perform specific immune functions. The research of Lv et al. 35 showed that anticancer drugs can stimulate human hepatoma cells to release exosomes with HSPs and trigger effective natural killer (NK) cell anti-tumor response in vitro. In conclusion, we infer that TRAP1 secreted to the outside of the cell may be regarded as a danger signal by the immune surveillance system and have the effect of immune stimulation.
The research of molecular chaperone vaccine in the treatment of cancer has promoted the establishment of the hypothesis of the immunophilic function of extracellular HSPs.36,37 Studies have indicated that Hsp90 forms a complex by binding with antigenic peptides and presenting it to antigen presenting cells (APCs) to mediate the cross presentation of acquired antigens by APCs. 38 In this process, Hsp90 can accompany the whole antigenic peptide to cross the plasma membrane of APC and guide it to the proteasome. APC processes and presents the antigen through MHC class I or MHC class II pathways, and finally displays it to T lymphocytes to activate cellular immunity. Therefore, we speculate that serum TRAP1 plays a role as a carrier of tumor specific antigen in tumor immunity. By carrying tumor antigen in the circulation into APCs, it triggers antigen cross presentation and cross priming of APCs, and then activates cytolytic immune cells such as NK cells and cytotoxic T lymphocytes (CTLs) to play an anti-tumor role. Currently, the source and secretion mechanism of TRAP1 in serum have not been clarified. The results of De Maio et al. 39 and Vega et al. 40 proved that Hsp70 in HSPs family can be released from many kinds of cells, containing tumor cells, reticulocytes, peripheral blood mononuclear cells, B lymphocytes, and dendritic cells. In view of the result that serum TRAP1 level in LD-SCLC is higher than that in ED-SCLC, one possible explanation is that the main source of circulating TRAP1 is the mature immune cells in human body rather than tumor cells. Tumor development dramatically drives extensive disruption of hematopoiesis and restructures the global immune landscape across immune cell lineages. 41 This disruption manifests most prominently in an expansion of immature neutrophils and monocytes in the periphery of tumor-burdened hosts, which then also traffic to the tumor microenvironment and contribute to local immunosuppression.42,43 Peripheral reorganization of the immune macroenvironment in cancer leads to decreased frequency of functional mature immune cells. Therefore, in patients with advanced cancer, the decreased frequency of mature immune cells gives rise to the decreased secretion of TRAP1 in mitochondria, and the decrease of serum TRAP1 concentration ultimately. At the same time, this may explain why the concentration range of serum TRAP1 varied greatly in Group NC. As the average age of the healthy volunteers included was close to 60 years old. Almost all immune cell types, both mature cells and their progenitors, go through age-related changes concerning numbers and functions, 44 which leads to lower numbers of functional mature immune cells, lymphoid cells, 45 for instance. In addition, a few of the elderly may suffer from chronic geriatric diseases beyond the exclusion criteria, leading to a further decline in immunity. The combination of the above two factors led to a low level of serum TRAP1 in the healthy control group. Nowadays, the research results in this field are scarce, and more clinical and basic research evidences are needed to clarify the relevant mechanisms.
Conclusions
In short, serum TRAP1 has high diagnostic value for SCLC and high sensitivity for LD-SCLC. It can detect the presence of tumor before SCLC occurs and spreads. It is a serological marker with great potential for SCLC. The detection rate of SCLC can be effectively improved by combined detection with NSE, CEA, and CA19-9. In addition, serum TRAP1 may be secreted into the circulation by mature immune cells and participate in tumor immunity as a carrier of tumor antigens.
Footnotes
Authors’ Contributions
LMT: conceptualization, funding/resources, data acquisition, validation and supervision. SPK: conceptualization, writing-original draft, and writing-review & editing. XL: methodology, funding/resources, and writing draft. TLO: conceptualization, formal analysis, writing-review & editing, project administration. LQY: data analysis, writing-review & editing. JLY: investigation, visualization. YKW: investigation and visualization. QJY: data curation. XHL: data curation and project administration. XY: statistical analysis. HL: writing-reviewing and editing. XYH: project administration and supervision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the ethics committee of the Second Affiliated Hospital of Nanchang University.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the following funds: Key Research and Development Program of Jiangxi Province [Grant Number: 20203BBGL73149, 20192BBG70033]; Science and Technology Plan of Health Commission of Jiangxi Province [Grant Number: 202210628, 20193468]; Special Fund for Postgraduate Innovation of Jiangxi Province [Grant Number: YC2021-S176]; Scientific Research Training Program for College Students of Nanchang University [Grant Number: No.43, No.130]; Research Project of Degree and Postgraduate Education and Teaching Reform of Nanchang University [Grant Number: NCUYJSJG-2022-064].