
Abstract
Intestinal mucosa barrier injury and immunity imbalance contribute to chronic kidney disease (CKD) progression. Type 3 innate lymphoid cells (ILC3s) are essential for normal intestinal homeostasis. Nevertheless, the relationship between ILC3s and CKD remains largely unknown. The aim of this study was to investigate the relationship linking ILC3s to clinical indicators among patients with renal dysfunction. The levels of circulating ILC3s and dendritic cells, as well as their subsets, in patients with renal dysfunction and healthy controls were determined through flow cytometry. The levels of human plasma granulocyte-macrophage colony-stimulating factor (GM-CSF) were measured using enzyme-linked immunosorbent assay. Renal function was evaluated by measuring the estimated glomerular filtration rate (eGFR), as well as the levels of serum creatinine, blood urea nitrogen (BUN), and uric acid. The results revealed that the proportion of peripheral ILC3s was significantly decreased in patients with renal dysfunction. This reduction was positively associated with the levels of eGFR, and inversely associated with the levels of BUN and uric acid. Similarly, the percentage of circulating C-C motif chemokine receptor 6-positive (CCR6 +) ILC3s was also obviously reduced, and demonstrated positive and negative associations with the levels of eGFR and BUN, respectively. Furthermore, the levels of CCR6 + ILC3s correlated positively with those of GM-CSF, as well as type 1 conventional dendritic cells (cDC1s), which also decreased in parallel with kidney function. Thus, the reduction of ILC3s, particularly CCR6 + ILC3s, was related to worsening kidney function in patients with renal dysfunction. This effect may delay renal function impairment by regulating cDC1s via the secretion of GM-CSF, indicating that CCR6 + ILC3s may serve as efficient biomarkers for evaluating kidney function.
Impact Statement
Intestinal barrier impairment and immunity imbalance drive the development of chronic kidney disease. Type 3 innate lymphoid cells (ILC3s) are essential for normal intestinal homeostasis. In this study, we demonstrated that reductions of ILC3s, particularly C-C motif chemokine receptor 6-positive (CCR6+) ILC3s, were related to worsening kidney function in patients with renal dysfunction. Therefore, these cells may serve as efficient biomarkers for the evaluation of kidney function.
Introduction
As a growing public health threat, chronic kidney disease (CKD) has an estimated global prevalence of 13.4% and is a major cause of death and morbidity worldwide. 1 An increasing body of data have indicated that intestinal mucosa immunity imbalance and barrier disruption are closely correlated with the development of CKD.2 –4 In CKD, the progressive loss of kidney function leads to functional and structural alterations in the gut mucosal barrier.5,6 Consequently, these changes result in the entry of toxins and immune-mediated pro-inflammatory products from the intestine to the bloodstream, contributing to CKD progression.7,8 Considering the harmful effect of intestinal barrier damage on kidney function, the identification of factors that maintain the intestinal barrier homeostasis may be beneficial for the prevention and treatment of CKD.
Recently, a novel class of innate immune cells termed innate lymphoid cells (ILCs), have been recognized as a critical regulator of sustaining barrier integrity, immune homeostasis, and host defense due to their presence and abundance in the barrier tissue surfaces, as well as their ability to rapidly respond to infection with diverse microbial pathogens.9,10 According to their expression of signature transcription factors and cytokines, ILCs can be categorized into three distinct subsets, encompassing types 1, 2, and 3 innate lymphoid cells (i.e. ILC1s, ILC2s, and ILC3s). These types of cells mimic the functions of T-helper 1 (Th1), Th2, and Th17 cells, respectively. 10 ILC3s, and particularly chemokine receptor 6-positive (CCR6+) ILC3s, are enriched at intestinal barrier surfaces where they play a curial role in intestinal barrier homeostasis by promoting epithelial wound healing, maintaining epithelial barrier function, and modulating the function of other resident immune cells.11 –14 These functions suggest that ILC3s may be beneficial for maintaining renal homeostasis by sustaining gut barrier integrity. The aim of this study was to investigate the relationship between ILC3s and clinical indicators in patients with renal dysfunction.
Materials and methods
Study participants
Patients with renal dysfunction and healthy controls (HCs) were recruited at the First Affiliated Hospital of Guangdong Pharmaceutical University (Guangzhou, China) from September 2020 to September 2021. Normal renal function was defined by an estimated glomerular filtration rate (eGFR) of ⩾ 90 mL/min/1.73 m2, while renal dysfunction was defined by an eGFR of < 90 mL/min/1.73 m2(CKD stages 2–5).15,16 The exclusion criteria were as follows: (1) non-renal dysfunction; (2) severe cardiac, pulmonary, liver, and infectious diseases; and (3) carcinoma. HCs without abnormalities (based on routine physical examinations) or a history of any kidney disease during the same period were enrolled. The ethics committee of the First Affiliated Hospital of Guangdong Pharmaceutical University approved the research protocol of this study (approval number: 2021146). Informed consent was provided by all participants.
Data collection
The following clinical information was obtained from the electronic medical record system: age, sex, medical history (including diabetes and hypertension), and levels of blood urea nitrogen (BUN), serum creatinine, and uric acid (UA). The Modification of Diet in Renal Disease formula-adjusted coefficient for Chinese individuals was used to estimate the eGFR. 17
Sample preparation and staining
Blood samples from peripheral veins were collected in heparin anticoagulation tubes. The samples were divided into two parts for isolation of peripheral blood mononuclear cells (PBMCs) and plasma. PBMCs were purified using Ficoll–Paque Plus (17-1440-03; GE Healthcare) density-gradient centrifugation. After 30 min of centrifugation at 400 g, mononuclear cells in the Ficoll-plasma interface were collected and washed twice with phosphate-buffered saline. Subsequently, PBMCs were subjected to cell surface staining with antibodies for 30 min at 4°C and in the dark. Plasma was obtained by centrifugation at 800 g for 20 min; the plasma samples were stored at −80°C until further analysis using enzyme-linked immunosorbent assay (ELISA).
Flow cytometry
Flow cytometry analysis was performed within 12 h after each blood sampling. The following surface marker antibodies (all purchased from Biolegend) were used to analyze ILCs and their subsets: 7-amino-actinomycin D (7-AAD) Viability Staining Solution (category number: 420404); fluorescein isothiocyanate (FITC) anti-human CD3 (category number: 300306); FITC anti-human CD5 (category number: 300606); FITC anti-human T cell receptor α/β (TCRα/β; category number: 306706); FITC anti-human CD16 (category number: 360716); FITC anti-human CD19 (category number: 302206); FITC anti-human CD11c (category number: 301604); allophycocyanin/Cyanine 7 (APC/Cyanine 7) anti-human CD45 (category number: 304014); APC/Cyanine 7 anti-human CD127 (category number: 351320); APC anti-human CD294 (category number: 350110); phycoerythrin (PE) anti-human CD117 (category number: 323408); and Alexa Fluor® 700 anti-human CCR6 (category number: 353434). Lineage markers included CD3, CD5, CD16, CD11c, CD19, and TCRα/β. ILCs were defined as 7-AAD− lineage−CD45 + CD127 + lymphocytes. ILC1s were defined as CD117−CD294− ILCs, ILC2s were defined as CD117−CD294 + ILCs, and ILC3s were defined as CD117 + CD294− ILCs. 18 CCR6 + ILC3s were defined as CCR6-positive cells among the total ILC3s.
Moreover, the following surface marker antibodies (all purchased from Biolegend) were used to analyze dendritic cells (DCs) and their subsets: FITC anti-human CD16 (category number: 302006); FITC anti-human CD14 (category number: 367116); FITC anti-human CD19 (category number: 363008); FITC anti-human CD20 (category number: 302304); FITC anti-human CD56 (category number: 362546); Brilliant Violet 65TManti-human human leukocyte antigen-DR (HLA-DR) (category number: 307650); PE/Cyanine7 anti-human CD11c (category number: 301608); APC/FireTM750 anti-human CD123 (category number: 306042); PE anti-human CD1c (category number: 331506); and Brilliant Violet 421TManti-human CD141 (category number: 344114). DCs were defined as CD14− CD16− CD19− CD20− CD56−HLA-DR + monocytes. Plasmacytoid dendritic cells (pDCs) were defined as CD123 + CD11− DCs. Conventional dendritic cells (cDCs) were defined as CD123− CD11c + DCs; type 1 conventional dendritic cells (cDC1s) were defined as CD141 + cDCs; type 2 conventional dendritic cells (cDC2s) were defined as CD1c + cDCs. 19 Flow cytometry was performed using a Beckman Cytoflex-2 flow cytometer, and the obtained data were analyzed using the software of the device.
ELISA
The levels of human granulocyte-macrophage colony-stimulating factor (GM-CSF) were measured in the plasma of 46 patients with renal disease using an ELISA kit (category number: 432007; BioLegend). Concentrations of GM-CSF were calculated by subtracting the absorbance measured at 570 nm from that measured at 450 nm.
Statistical analysis
Data analysis and graph plotting were conducted using the GraphPad Prism 9.0 software (GraphPad Software Inc., San Diego, CA, USA). Unpaired Student’s t-tests were used to analyze normally distributed data, expressed as the mean and standard deviation. Mann–Whitney U tests were used to analyze non-normally distributed data, expressed as the median (interquartile range). Pearson or Spearman coefficients were used for the calculation of correlations between variables. Two-sided p-values < 0.05 denoted statistically significant differences.
Results
Peripheral ILC3s were reduced in patients with renal dysfunction
A total of 57 patients with renal dysfunction and 27 HCs were enrolled in this study. Their characteristics are summarized in Table 1. Initially, we evaluated the levels of circulating ILCs and their subsets among patients with renal dysfunction. The gating strategy for ILCs and their subsets is shown in Figure 1(a). Compared with HCs, patients with renal dysfunction presented a lower frequency of ILCs (0.09 (0.06–0.12) vs 0.15 (0.09–0.20)%, respectively; p = 0.002) (Figure 1(b)). On subgroup analysis, patients with renal dysfunction exhibited significantly reduced percentages of ILC3s to ILCs (18.87 (12.15–31.55) vs 30.30 (21.12–34.23)%, respectively; p = 0.012) and ILC1s to ILCs (18.63 (12.17–28.73) vs 25.97 (20.25–34.95)%, respectively; p = 0.014) than HCs; however, differences were not observed between the two groups in terms of the percentage of ILC2s to ILCs (Figure 1(c)).
Participant characteristics.
eGFR: estimated glomerular filtration rate; BUN: blood urea nitrogen; UA: uric acid.
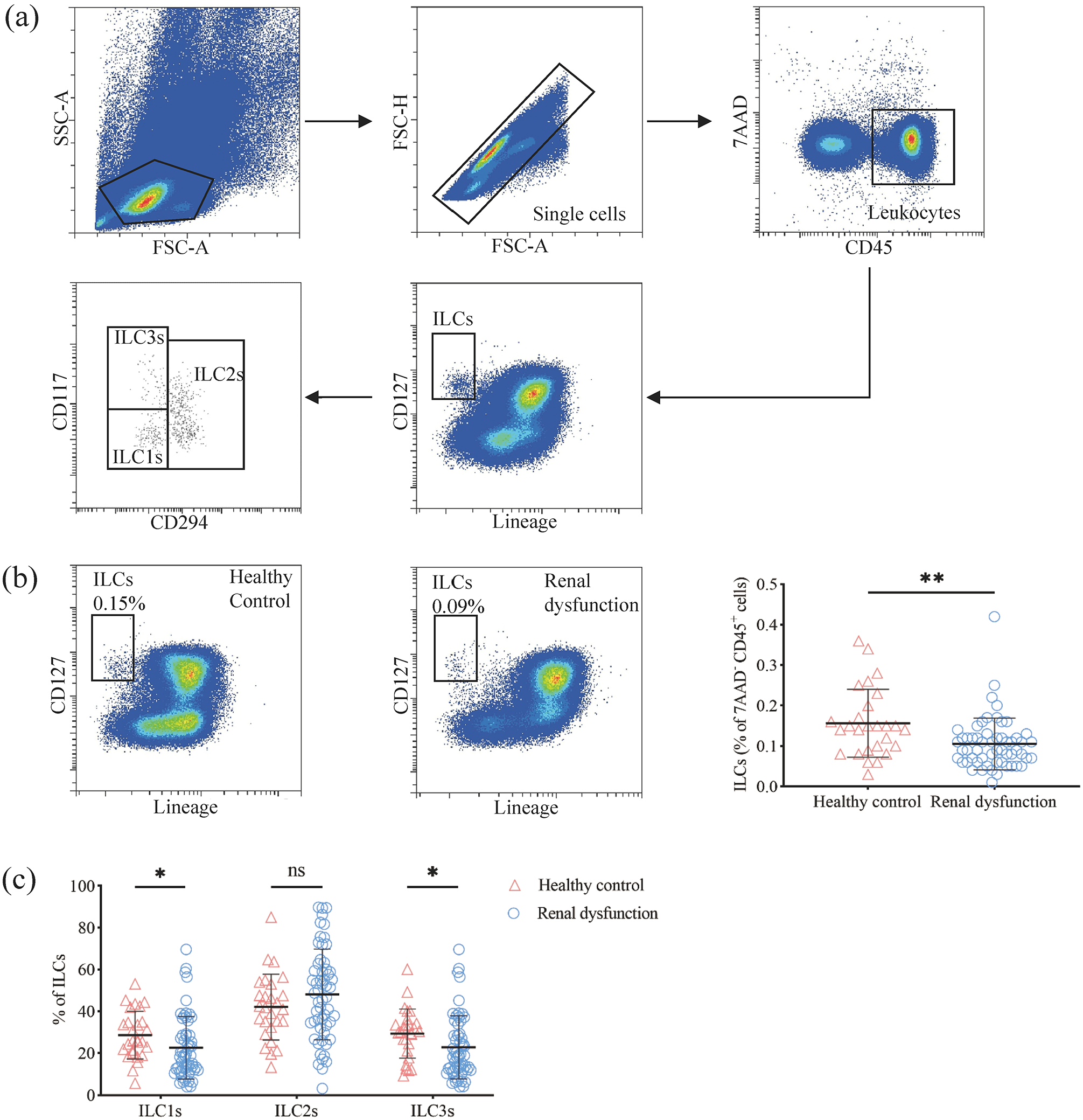
Reduction of peripheral ILC3s in patients with renal dysfunction. (a) Gating strategy for peripheral ILCs and their subsets. (b) Characteristic distribution of peripheral ILCs among patients with renal dysfunction. (c) Characteristic distribution of peripheral ILCs subsets among patients with renal dysfunction. 7AAD, 7-amino-actinomycin D; FSC, forward scatter; ILCs, innate lymphoid cells; ILC1s, type 1 innate lymphoid cells; ILC2s, type 2 innate lymphoid cells; ILC3s, type 3 innate lymphoid cells; ns, no significant; SSC, side scatter. *p < 0.05; **p < 0.01.
The levels of peripheral ILC3s correlated with renal function parameters
Correlations between the levels of ILC3s and renal function parameters were further analyzed in patients with renal dysfunction. The proportion of ILC3s showed a positive relationship with the eGFR (r = 0.338, p = 0.010) and a negative relationship with the levels of BUN (r = −0.334, p = 0.011) and UA (r = −0.300, p = 0.033). Notably, the proportion of ILC3s and the levels of serum creatinine were not significantly correlated (Figure 2).
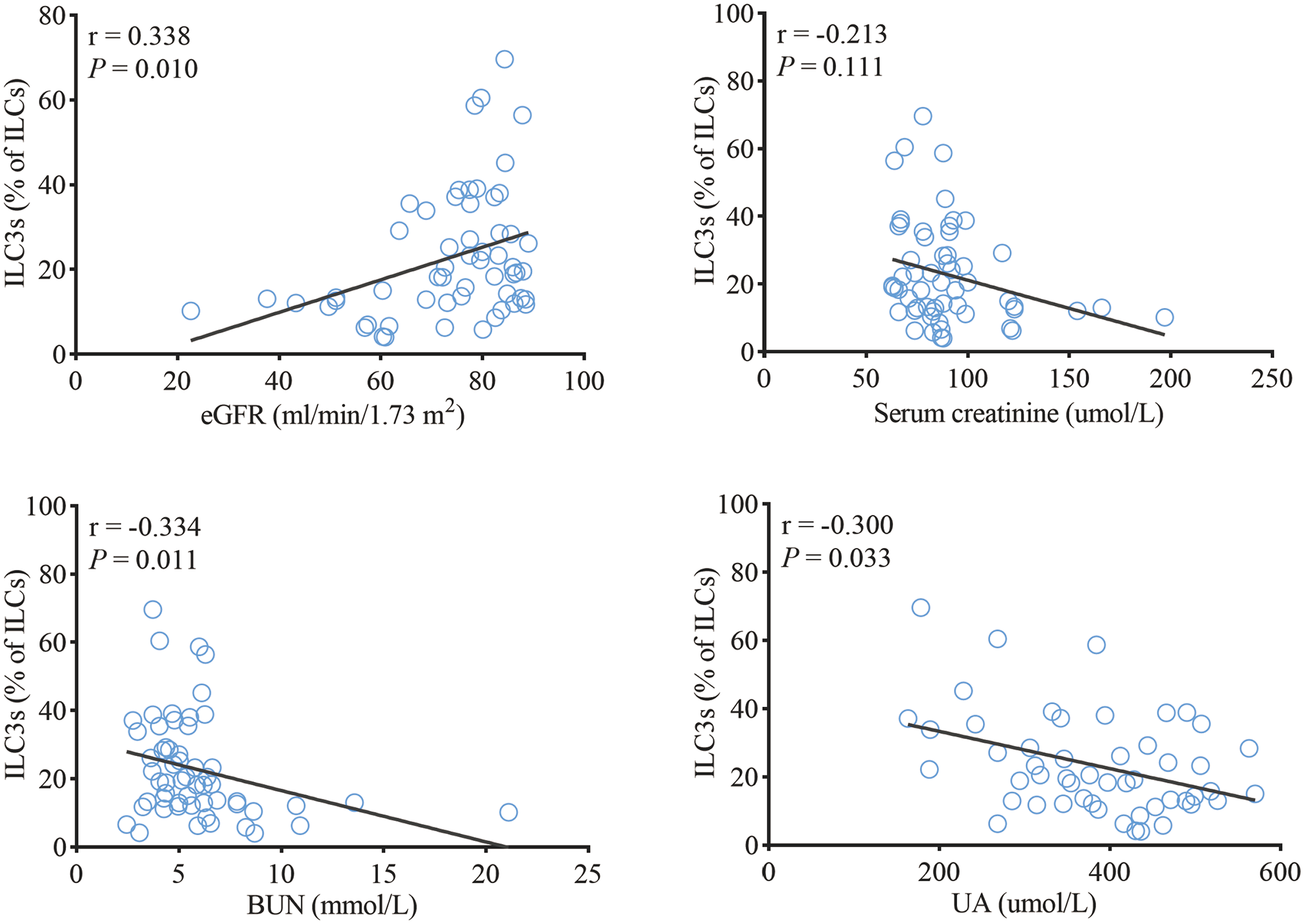
Levels of peripheral ILC3s showing correlation with renal function parameters. BUN, blood urea nitrogen; eGFR, estimated glomerular filtration rate; ILC3s, group 3 innate lymphoid cells; UA, uric acid.
The levels of peripheral CCR6 + ILC3s correlated with renal function parameters
The levels of CCR6 + ILC3 between patients with renal dysfunction and HCs were compared. Patients with renal dysfunction presented a lower frequency of CCR6 + ILC3s than HCs (5.38 (1.16–11.15) vs 7.76 (6.04–10.72) %, respectively; p = 0.038) (Figure 3(a)). Moreover, a positive association was found between the frequency of CCR6 + ILC3s and the eGFR (r = 0.317, p = 0.016), while an inverse association was found between the frequency of CCR6 + ILC3s and the levels of BUN (r = −0.265, p = 0.046). Nevertheless, the frequency of CCR6 + ILC3s in ILCs was not significantly associated with the levels of serum creatinine and UA (Figure 3(b)).
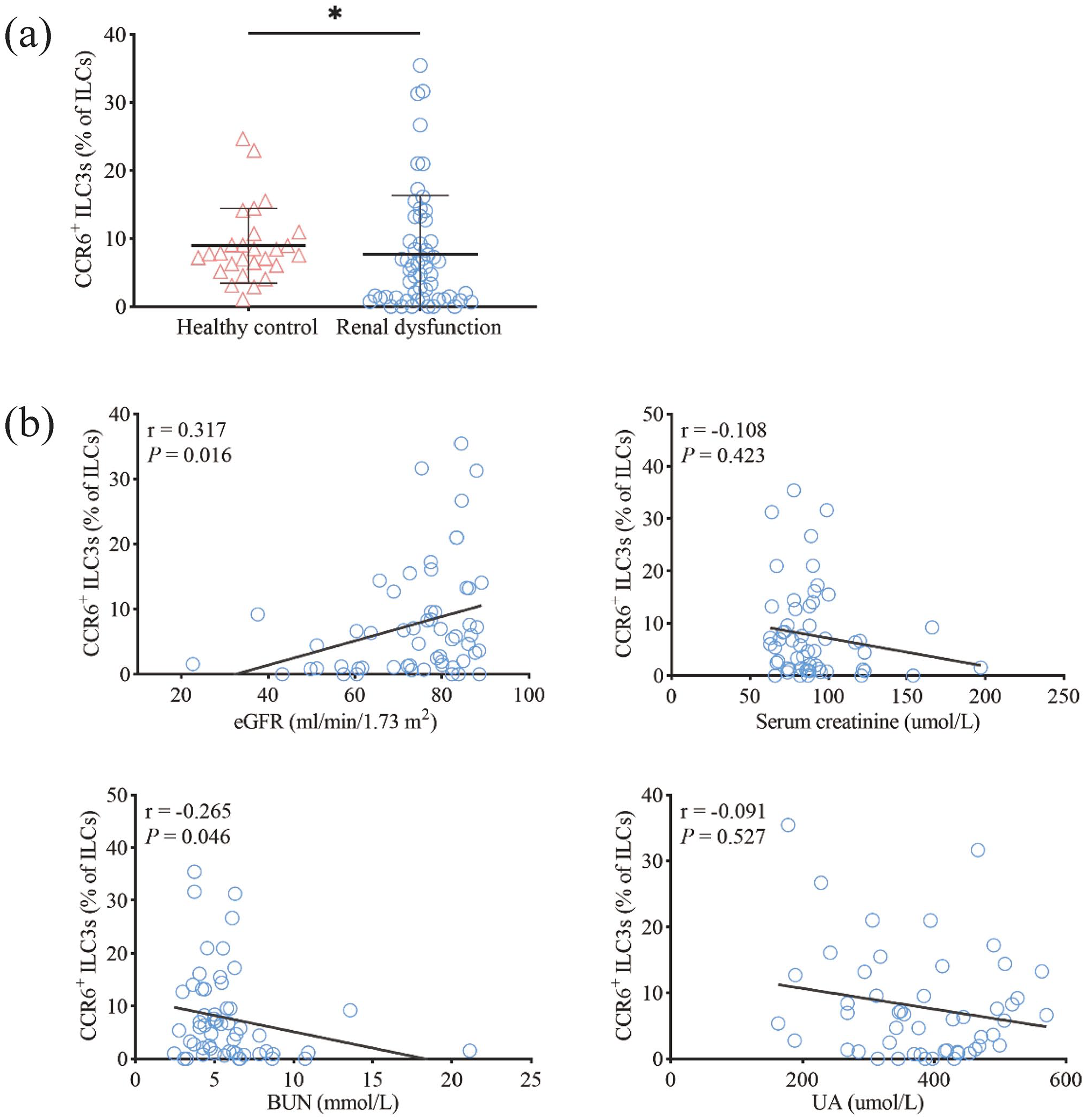
Levels of peripheral CCR6 + ILC3s showing correlation with renal function parameters. (a) Characteristic distribution of peripheral CCR6 + ILC3s among patients with renal dysfunction. (b) Correlations linking the levels of CCR6 + ILC3s to renal function parameters in patients with renal dysfunction. BUN, blood urea nitrogen; eGFR, estimated glomerular filtration rate; FSC, forward scatter; ILCs, innate lymphoid cells; ILC3s, type 3 innate lymphoid cells; SSC, side scatter; UA, uric acid. *p < 0.05.
The levels of peripheral CCR6 + ILC3s correlated with those of cDC1s and GM-CSF
Recently, it was shown that ILC3s promote the differentiation of DCs by releasing GM-CSF to maintain immune homeostasis in the intestine; 20 DCs have been recognized as critical effector cells related to hemostasis and inflammation in CKD. 21 Therefore, we sought to investigate whether the levels of DCs correlated with those of renal function parameters among patients with renal dysfunction. Blood samples were obtained from 24 patients with renal dysfunction and 10 HCs to determine the levels of DCs and their subsets. However, the levels of DCs did not differ significantly between the two groups (Figures 4(a) and (b)). Further subgroup analysis revealed that, patients with renal dysfunction had lower proportions of pDCs compared with HCs (29.75 ± 5.82 vs 15.49 ± 11.26%, respectively; p < 0.001) and cDC1s (2.88 ± 0.77 vs 1.88 ± 1.32%, respectively; p = 0.033) (Figure 4(c)). In addition, the frequency of cDC1s was positively associated with the eGFR (r = 0.446, p = 0.029), and inversely associated with the levels of serum creatinine (r = −0.414, p = 0.044) and UA (r = −0.714, p < 0.001) (Figure 5(a)). However, the frequency of pDCs was not associated with the levels of eGFR, serum creatinine, BUN, and UA (Figure 5(b)).
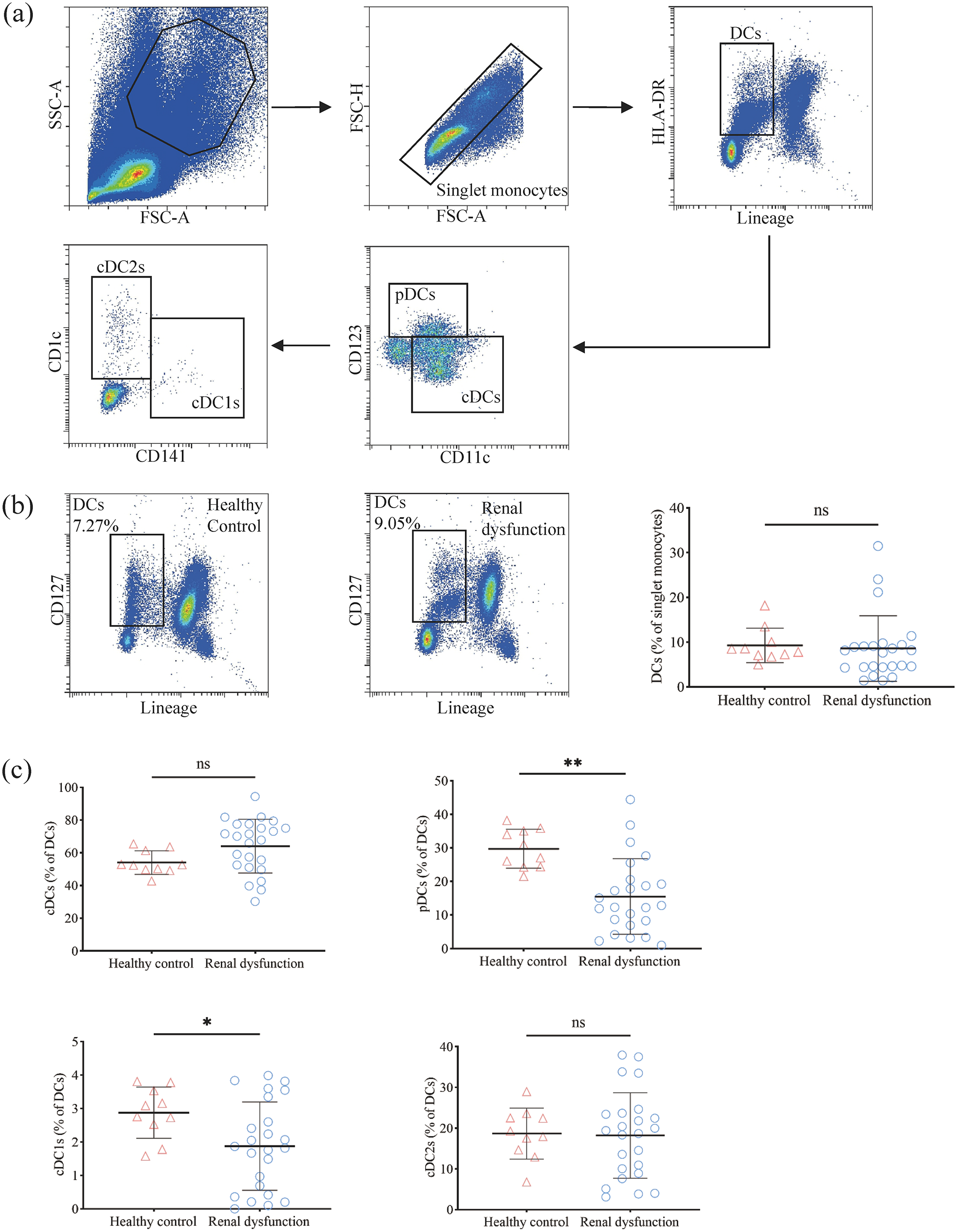
Reduction of peripheral pDCs and cDC1s in patients with renal dysfunction. (a) Gating strategy for the DCs and their subsets. (b) Characteristic distribution of peripheral DCs among patients with renal dysfunction. (c) Characteristic distribution of peripheral DCs subsets among patients with renal dysfunction. cDCs, conventional dendritic cells; cDC1s, type 1 conventional dendritic cells; cDC2s, type 2 conventional dendritic cells; DCs, dendritic cells; FSC, forward scatter; ns, no significant; HLA-DR, human leukocyte antigen-DR; pDCs, plasmacytoid dendritic cells; SSC, side scatter. *p < 0.05; **p < 0.01.
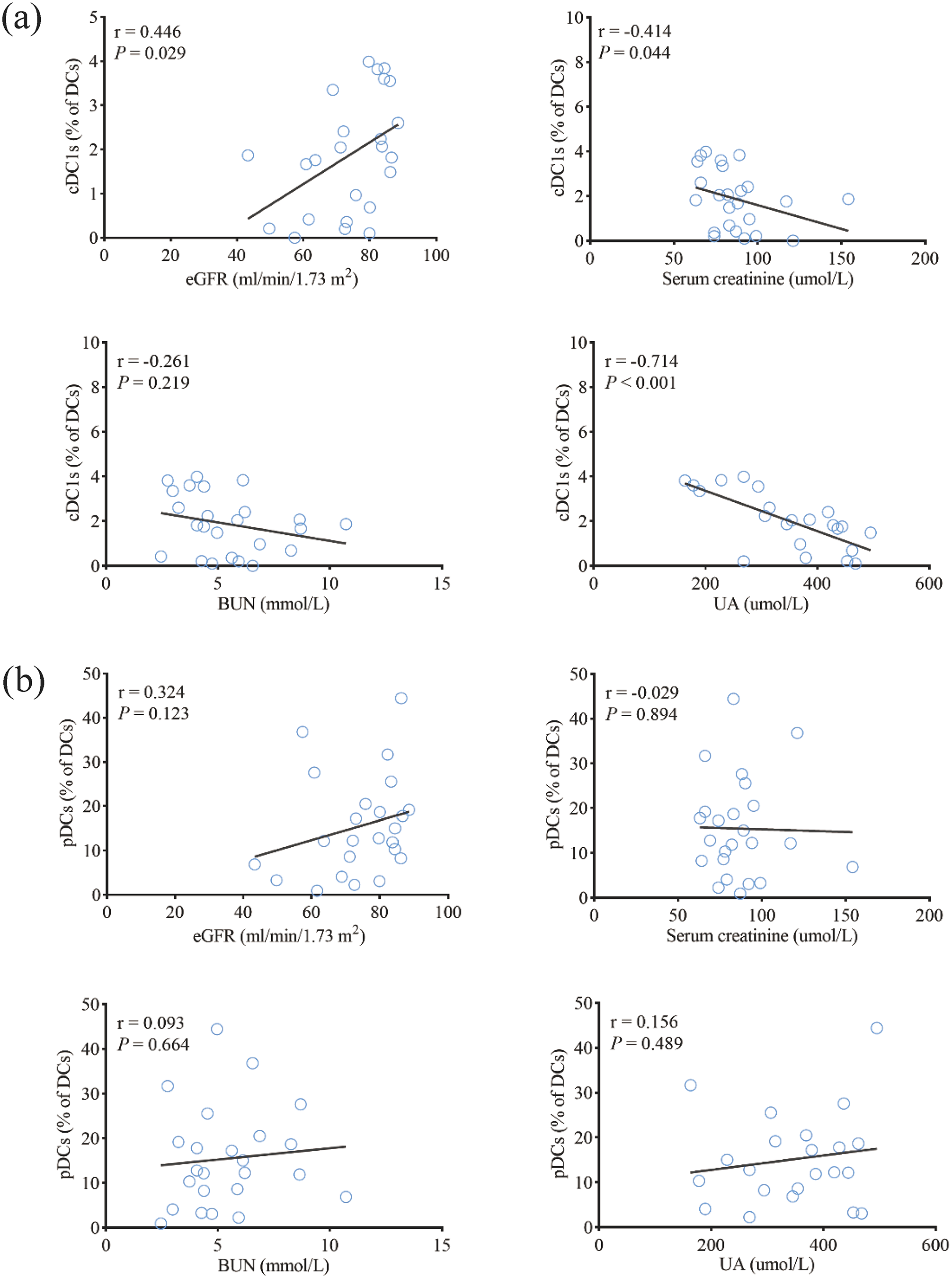
Levels of peripheral cDC1s showing correlation with renal function parameters. (a) Correlations linking the proportion of cDC1s to renal function parameters in patients with renal dysfunction. (b) Correlations linking the proportion of pDCs to renal function parameters in patients with renal dysfunction. BUN, blood urea nitrogen; cDC1s, type 1 conventional dendritic cells; DCs, dendritic cells; eGFR, estimated glomerular filtration rate; pDCs, plasmacytoid dendritic cells; UA, uric acid.
The correlations between the levels of ILC3s and CCR6 + ILC3s with those of cDC1s and GM-CSF were further analyzed. As shown in Figure 6, the frequency of ILC3s was positively correlated with that of cDC1s (r = 0.678, p < 0.001). Moreover, the levels of CCR6 + ILC3s were positively related to those of cDC1s (r = 0.528, p = 0.008) and GM-CSF (r = 0.415, p = 0.004).
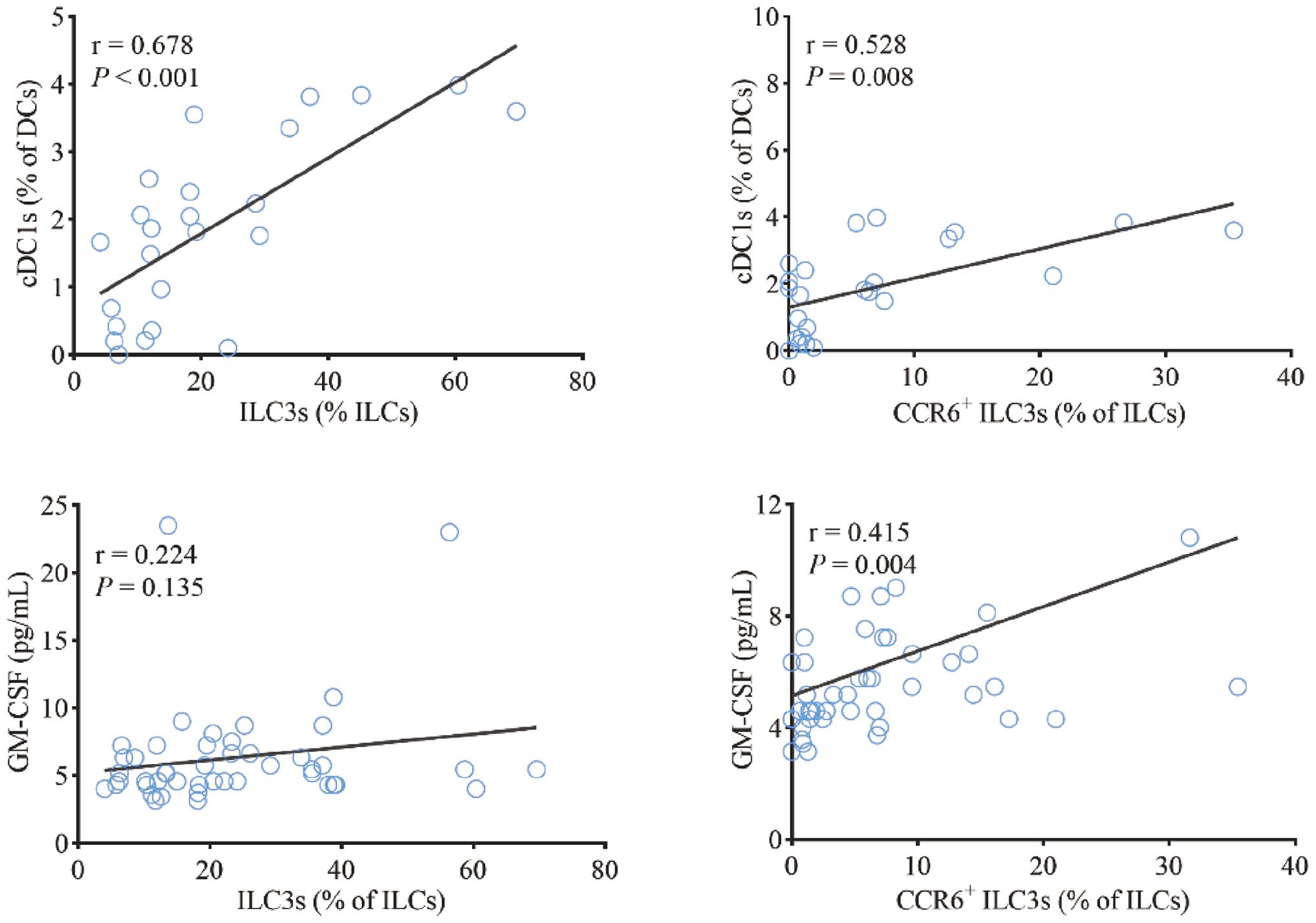
Levels of peripheral CCR6 + ILC3 showing correlation with those of peripheral cDC1s and GM-CSF. CCR6, C-C motif chemokine receptor 6; cDC1s, type 1 conventional dendritic cells; GM-CSF, granulocyte-macrophage colony-stimulating factor; ILCs, innate lymphoid cells; ILC3s, type 3 innate lymphoid cells.
Discussion
Accumulating evidence has demonstrated the importance of ILCs in the pathogenesis of CKD. 22 In mice with anti-glomerular basement membrane glomerulonephritis, ILC1s protect against renal injury by secreting Th1 cytokines. 23 Moreover, increased levels of ILC2s reduce renal injury and improved kidney function by producing Th2 cytokines and regulating anti-inflammatory macrophages in models of renal ischemic/reperfusion injury24,25 and adriamycin-induced glomerulosclerosis. 26 In the present study, the levels of circulating ILC3s were markedly decreased in patients with renal dysfunction and negatively correlated to disease severity. Similarly, a clinical study demonstrated that the percentage of peripheral ILC3s is notably decreased in lupus nephritis, particularly in patients with severe clinical symptoms. 27 This indicates that ILC3s may be an efficient biomarker for the evaluation of kidney function.
Previous studies have confirmed that CKD is linked to impaired gut barrier function.5,6,28 Yang et al. 29 observed that mice with CKD exhibited a reduction of claudin 1 (CLDN1) and increase of pro-inflammatory macrophages in the intestinal tissue, while probiotic treatment restored the normal levels to alleviate systemic inflammation and kidney fibrosis. ILC3s play a vital role in the generation of intestinal lymhoid tissue, thereby regulating the microbial population and maintaining the intestinal epithelial barrier integrity. 30 Loss of ILC3s induces a reduction in the numbers of intestinal stem cells and leads to the impairment of epithelial barrier function. 31 Interestingly, intestinal ILCs can spread to other tissues and organs via the circulation. 32 Furthermore, in patients with inflammatory bowel disease, the reduction in immature ILC3s in inflamed gut tissue has been found to parallel the reduction of immature ILC3s in the peripheral blood; 33 this finding was similar to those from another study, 34 and suggests that circulating ILC3s may reflect the ILC3 status in the intestine. As an ILC3s subset primarily enriched in the intestinal tract, CCR6 + ILC3s are of particular interest. 35 These cells can reduce intestinal impairment through expression of the major histocompatibility complex, which directly affects the function of CD4 + T cells.36,37 Furthermore, in nephritic mice, CCR6 deficiency aggravates renal tissue damage, albuminuria, and renal function loss. 38 In the present study, we also found that the levels of CCR6 + ILC3s were significantly reduced among patients with renal dysfunction and decreased in the parallel with kidney function. Therefore, through their beneficial impact on the gut barrier homeostasis, ILC3s may exert a protective effect against renal dysfunction.
The proportions of ILC3s and CCR6 + ILC3s were significantly correlated with the eGFR values, but not with the serum creatinine levels. Some conditions may have contributed to this finding. Compared to serum creatinine, eGFR is regarded as a more reliable and accurate index for monitoring of kidney dysfunction. 17 Serum creatinine levels may remain within normal limits in cases where the glomerular filtration rate is reduced to 50% of its normal value; 39 it is also easily influenced by age, gender, and daily diet.40,41 In this study, the level of UA was positively associated with the frequency of ILC3s, but not CCR6 + ILC3s. This indicated that CCR6 + ILC3s may not be the major subgroup of ILC3s that correlate with UA levels. As ILC3s represent a highly heterogeneous population that can be divided into different subgroups, 42 further research is needed to identify the subgroup of ILC3s relevant to UA levels.
CKD is characterized by significant alterations in the subsets of DCs, which have been linked to the development of this disease.43,44 In the present study, lower levels of peripheral pDCs were observed in patients with renal dysfunction versus HCs. However, there was no difference in the levels of peripheral cDCs between the two groups; this finding was similar to the data reported in a previous study. 45 Furthermore, our results revealed that the proportion of cDC1s was lower in patients with renal dysfunction and negatively correlated with the disease severity. Kurts et al. 46 reported that depletion of cDC1s led to diminished creatinine clearance, a tendency toward higher proteinuria, and more severe glomerular damage in mice with crescentic glomerulonephritis. Collectively, these observations indicate the role of cDC1s in the protection against renal dysfunction.
Moreover, several in vivo studies showed that the differentiation of DCs was regulated by ILC3s.47,48 In the current study, the levels of cDC1s were positively correlated with the frequency of ILC3s and CCR6 + ILC3s. Research has suggested that ILC3-derived GM-CSF interacts with intestinal DCs to facilitate the production of retinoic acid and interleukin-10 (IL-10), which in turn contributes to intestinal immune homeostasis. 20 We also found a positive correlation between the levels of CCR6 + ILC3s and plasma GM-CSF. These findings suggest that CCR6 + ILC3s appears to protect against impairment of kidney function by regulating cDC1s via the secretion of GM-CSF.
This study has some limitations. First, as this was a cross-sectional study, the causal relationship between ILC3s and disease severity in patients with renal dysfunction could not be determined. Second, the characteristics of ILC3s in the intestine and kidney tissue could not be assessed because we did not obtain such specimens. Thus, whether ILC3s delay the development of CKD by maintaining intestinal homeostasis and the underlying mechanism involved in this process warrant further investigation.
In summary, the reduction of ILC3s, particularly CCR6 + ILC3s, was related to worsening kidney function in patients with renal dysfunction. This effect may delay renal function impairment by regulating cDC1s via the secretion of GM-CSF. Therefore, ILC3s and CCR6 + ILC3s may serve as biomarkers for the evaluation of kidney function and be a future target in patients with CKD.
Footnotes
Authors’ Contributions
All authors have reviewed and approved the submitted version of this article. HJZ and XXH designed the study. ZYP, HQL, and YPZ performed experiments, statistical analysis, and wrote the initial draft of the manuscript. HBT, XYY, and HJZ contributed to revision. Z-YP, HQL, Y-PZ have contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the ethics committee of the First Affiliated Hospital of Guangdong Pharmaceutical University [approval number 2021146].
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Key-Area Research and Development Program of Guangdong Province (grant number 2022B1111070006), the Guangdong Innovation Research Team for Higher Education (grant number 2021KCXTD025), China Postdoctoral Science Foundation [grant number 2021M700034], Department of Education of Guangdong Province [grant number 2018GKTSCX033] and Bureau of Education of Guangzhou Municipality [grant number 202032875].