
Abstract
Cytophagocytic mononuclear (CPM) cells, previously known as Reiter’s cells, are macrophages containing apoptotic polymorphonuclear leucocytes. Although they can be found in synovial fluid (SF) from different arthropathies, their role remains unclear. This study was performed to determine the frequency and disease distribution of CPM cells in SF in a large cohort of patients with rheumatic diseases over a 12-year period. We also investigated the seasonal variation in their incidence. This record review study included the reports pertaining to SF analyses performed between January 2010 and December 2021. Data were retrieved from the charts of inpatients and outpatients at Rheumatology and Emergency Departments of Padova. The total number of SF samples containing CPM cells was 189: 69% was from patients with seronegative spondyloarthritis (SpA), thus indicating a strong association between CPM cells and SpA. SF samples containing CPM cells were predominantly inflammatory. Our analyses demonstrated a 6-month cyclical fluctuation in concentrations of CPM cells, with an increase in spring and autumn. The presence of CPM cells in SF might offer diagnostic insight into the definition of SpA. Further studies are warranted to ascertain the link between CPM cells and the apoptotic process, shedding light on the mechanisms leading to their formation.
Impact statement
Synovial fluid analysis is one of the most important laboratory tests in Rheumatology. It determines and correlates the degree of inflammation with disease severity. More important is its role in the immediate diagnosis of septic and crystal arthritis. The most studied cell populations in synovial fluid are monocytes, lymphocytes and polymorphonuclear cells. These cells are involved in the induction and in the resolution of the inflammatory process, but there’s no distinct phenotypes associated with specific rheumatological disease. By contrast, in this work we found that cytophagocytic mononuclear cells, best known as Reiter’s cells, are commonly associated with spondyloarthritis and present a seasonal variation with an increased frequency during spring and autumn. This finding can impact the initial evaluation of a patient with arthritis and offer new insights into the pathogenetic mechanisms of spondyloarthritis.
Introduction
Synovial fluid (SF) plays a vital role in maintaining joint integrity, lubrication and function. The varying degrees of inflammation in joint diseases result in alterations of the cellular and molecular composition of the SF. Consequently, SF analysis constitutes an important diagnostic tool in patients with musculoskeletal symptoms, especially in the early stages of the disease. Cell count analysis allows the classification of SF according to the total number of leucocytes and the percentage of mono- and polymorphonuclear cells (PMNs).
Neutrophils correlate positively with the degree of inflammation expressed by total white cell count, levels of inflammatory cytokines and other biomarkers. 1 In addition to monocytes, lymphocytes, and neutrophils, other cell populations of the mesenchymal or haematopoietic lineage can be found in SF, including chondrocytes, synoviocytes, mast cells, and cytophagocytic mononuclear (CPM) cells.2,3
CPM cells, previously known as Reiter cells, are macrophages containing apoptotic polymorphonuclear leucocytes at varying stages of degeneration (Figure 1). They were first described by Pekin et al. 4 in SF collected from two patients with reactive arthritis, formerly known as Reiter’s syndrome. Although of poor diagnostic value, 5 CPM cells have been associated with reactive arthritis, psoriatic arthritis, and ankylosing spondylitis. 3 In the absence of infective or crystal-induced arthritis (CIA), their presence is still considered as evidence of possible reactive arthritis.
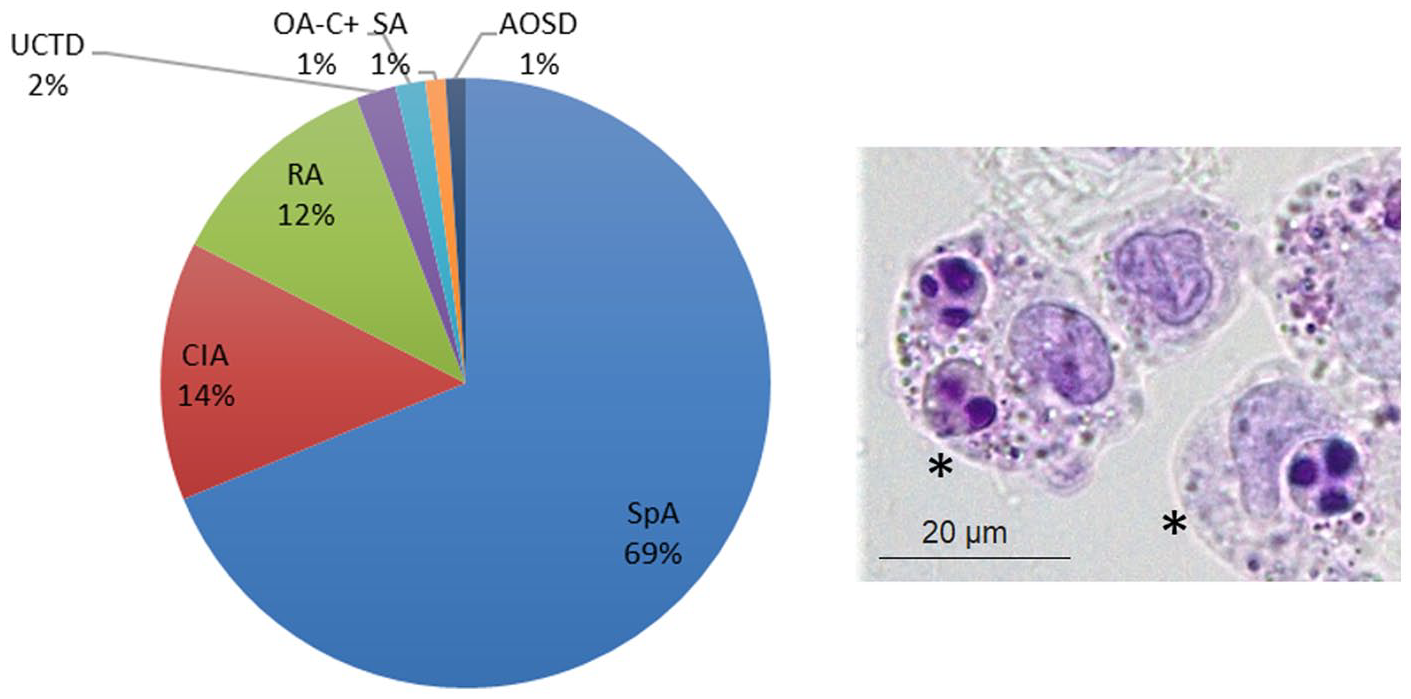
Disease distribution of cytophagocytic mononuclear cells during the studied period.
We aimed to investigate the distribution of CPM cells in SF samples in a large cohort of patients with different arthropathies over a 12-year period. Furthermore, using laboratory data and evidence-based observations, we also set out to ascertain possible seasonal variations in their incidence.
Materials and methods
The study was a record review study and have been conducted following the guiding checklist for the assessment of quality of RRS studies. 6 We analyzed SF analysis reports from the charts of all inpatients and outpatients in the Rheumatology and Emergency Departments of Padova University Hospital, between January 2010 and December 2021. We identified all SF samples containing CPM cells and gathered the following data: age, sex, SF, white blood cell (WBC) count, PMN and monocytes (M) percentage, as well as monosodium urate (MSU) and calcium pyrophosphate (CPP) crystals. A subsequent search on the hospital clinical database was performed to record the diagnosis of each enrolled patient. The investigators deidentified all patients’ protected health information from the data set.
SF examinations were performed according to standard methods. We used a Bürker counting chamber and prestained slides for cell morphology (Testsimplets®) to calculate total and differential WBC count, respectively; whereas the crystal search was performed using compensated polarized light microscopy.
CPM cells, when present, were evidenced under ordinary light in the Testsimplets® slide using one drop of fresh SF and a 1000x final magnification. They were recorded during differential cell determination by counting 100 consecutive leucocytes and expressing their number as percentage. To test whether CPM cell frequency presented a cyclical (seasonal) trend of variation, we calculated the percentage of CPM-positive SF samples for each month, adjusted to the total number of SF samples examined over the same period, reported the mean over 12 years, and combined data according to the four seasons: winter (December to February), spring (March to May), summer (June to August), and autumn (September to November).
Nonlinear regressions were used to derive a sine wave function, fitted to the per month percentage of CPM positive SF samples, using least squares method to identify the best parameter combination.
Non-parametric Kruskal-Wallis test with Dunn’s multiple comparison test was performed to compare SF characteristics among the diseases.
Results
We found CPM cells in 189 samples, with a percentage ranging from 1% to 3% per sample and distributed among the following diseases: spondyloarthritis (SpA), CIA, rheumatoid arthritis (RA), undifferentiated connective tissue disease (UCTD), osteoarthritis (OA) with crystals, septic arthritis (SA) and adult-onset Still’s disease (AOSD) (Table 1). We found that CPM cells were more frequent (69%) in SpA vs remaining arthropathies (Figure 1).
Features of the synovial fluid containing CPM cells according to disease distribution.
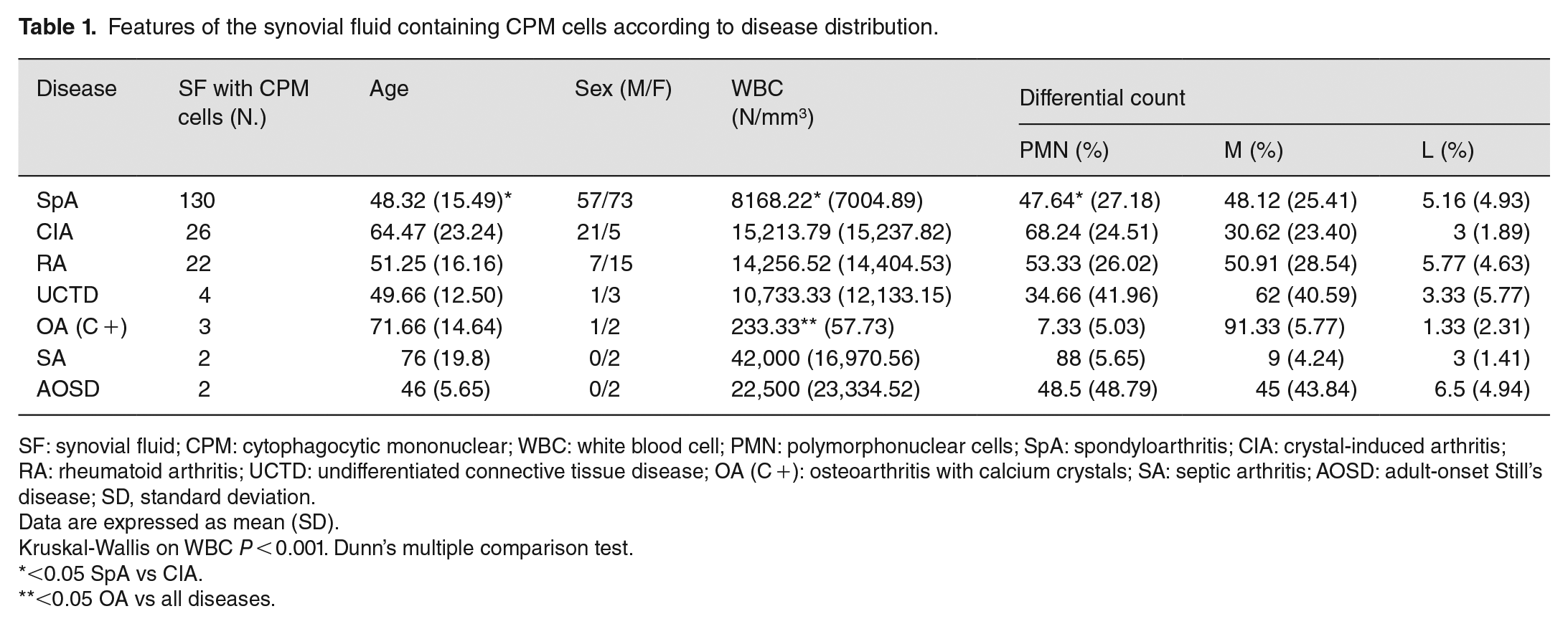
SF: synovial fluid; CPM: cytophagocytic mononuclear; WBC: white blood cell; PMN: polymorphonuclear cells; SpA: spondyloarthritis; CIA: crystal-induced arthritis; RA: rheumatoid arthritis; UCTD: undifferentiated connective tissue disease; OA (C +): osteoarthritis with calcium crystals; SA: septic arthritis; AOSD: adult-onset Still’s disease; SD, standard deviation.
Data are expressed as mean (SD).
Kruskal-Wallis on WBC P < 0.001. Dunn’s multiple comparison test.
<0.05 SpA vs CIA.
<0.05 OA vs all diseases.
The characteristics of SF containing CPM cells according to disease distribution are also reported in Table 1. Except for OA with calcium crystals (3 patients), all samples were inflammatory with a variable percentage of PMN cells. WBC in SF of patients with SpA were significantly lower vs patients with CIA, whereas no differences were found between SpA and RA. WBC in SF of patients with OA were significantly lower vs all the other arthropathies. SpA patients were the youngest among the population considered (Table 1).
Notably, we detected a seasonal pattern in the presence of CPM cells in SF with an increased frequency during spring and autumn (Figure 2). Using non-linear fit tools, we found monthly fluctuations in CPM cell frequency by a quantity that could be described by a sine wave function. In detail, the best-fit values demonstrated that a cyclical increase of CPM cell frequency could be observed about every 6 months, with an amplitude of variation estimated to be around 1.6 %.
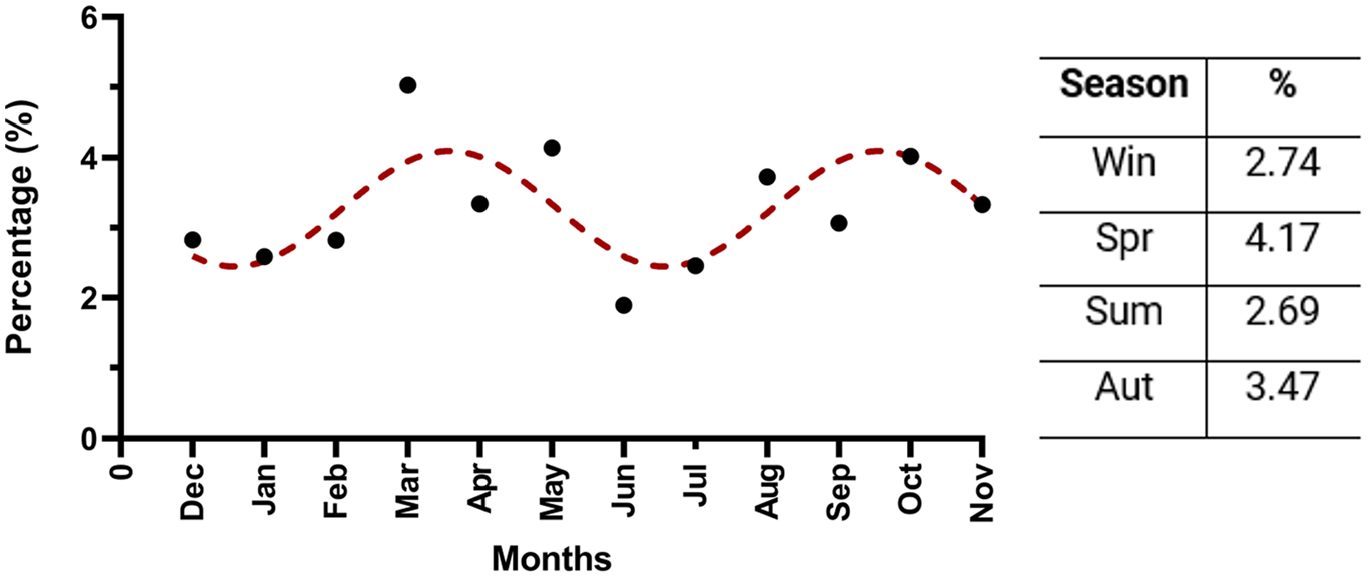
Seasonal variation of cytophagocytic mononuclear cells during the studied period.
Discussion
Our study explored the distribution of CPM cells in SF samples collected from a large cohort of patients with various arthropathies, using a chart review method. We found that CPM cells can be found in inflammatory SF and are mainly associated with seronegative SpA.
CPM cells have been described as macrophages involved in the clearance of apoptotic PMN cells as part of the resolution of joint inflammation. 7 Spent neutrophils are cleared via phagocytosis by macrophages and collected in the cytoplasm, thus forming a CPM cell.7,8 Therefore, the presence of CPM cells in SF might be related to apoptosis undergone by neutrophils. There are little data in the literature on the process of apoptosis in SF and the formation of CPM cells. Furthermore, it is not clear whether apoptosis is more pronounced in SF of patients with SpA vs other arthropathies.
In this regard, distinct levels of SF leucocyte apoptosis have been reported in different diseases. In the earliest clinically phase of RA, for instance, the inhibition of neutrophil and lymphocyte apoptosis allows to distinguish the disease from other early-stage arthritides. This process has been linked to the high levels of anti-apoptotic cytokines found in the joints of these patients, hence contributing to the accumulation of leucocytes. 9 Another possible explanation might be linked to the association between neutrophil survival and osteopontin, a glycosylated phosphoprotein that functions as a proinflammatory cytokine. Osteopontin and its cleaved forms have been shown to protect neutrophils from apoptosis and have been found significantly higher in SF of patients with RA vs PsA. 10 Lower levels of osteopontin in the SF of SpA patients may explain, at least in part, increased neutrophil apoptosis and resolution of inflammation via CPM cell formation. Moreover, leucocyte apoptosis is also inhibited by adenosine, which has been found elevated in SF of patients with RA and inversely correlated with the number of apoptotic neutrophils. 11 The second interesting observation of this study concerns the seasonal variation of CPM cell levels in SF. Our analyses revealed a 6-month cyclical variation in the presence of CPM cells with an increase in spring and, albeit to a lesser extent, in autumn. Seasonal cyclicity is a common feature of many diseases, especially those of infectious origin. Other features such as blood pressure, diabetes, psoriasis and vitamin D levels12,13 also present cyclical variations. Vitamin D deficiency, for instance, worsens during autumn and is associated with a higher risk of infection and chronic inflammation. 14 Moreover, dietary intake follows seasonal patterns and may result in alterations in the gut microbiome with repercussions on the pathogenesis and disease activity of many pathologies.14,15
Regarding the increased frequency of CPM cells in spring, we hypothesize an association between the presence of these cells and an increased number of flares in the patients. It has been reported that infectious triggers may play a role both in the pathogenesis and flares of SpA, 16 thus suggesting a possible link between infection, flares, and the presence of CPM cells in SF. However, a study conducted on a large cohort of patients with multiple follow-up visits over time, found that patients’ characteristics and disease activity did not appear to be affected by the change of seasons. 17 Although no association between improvement or flare and seasons has been found, we cannot rule out this hypothesis because of the different climate zones of the two works and the lack of further observations. We would remiss not to mention some of the limitations of our study. First, the design of the study may result in some information bias during data collection and analysis. Second, the strength of the association between CPM cells and SpA cannot be exactly established.
Although further epidemiological studies are warranted, CPM cells may offer an additional diagnostic datapoint for the definition of SpA. Furthermore, ascertaining the relationship between CPM cells and the apoptotic process may help clarify the mechanisms of their formation.
Footnotes
Acknowledgements
The Authors would like to thank Professor Leonardo Punzi for his precious mentorship in the field of synovial fluid analysis, and Eric Frank Nde for his assistance in editing the English version of this manuscript.
Authors’ Contributions
G.P., O.F., R.R., and S.A.: study conception; G.P., L.M., O.F., and S.A.: data collection; O.F. and P.A.: analysis and interpretation of results; O.F. and R.R.: draft preparation; G.P., L.M., O.F., P.A., R.R., and S.A.: draft critical revision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Padova (grant number DOR2278227/22) and the non-profit Organization “Studi in Reumatologia Antonio Spadaro” (RUNTS).