
Abstract
Increased vulnerability to physiologic stressors, termed frailty, is a common occurrence in patients with chronic heart failure (CHF). However, the definite biomarkers to assess frailty in CHF patients are not known. Here, we assessed the frailty phenotype and its potential association with heart failure (HF) markers in CHF patients. We categorized controls (n = 59) and CHF patients (n = 80), the participants, into robust, pre-frail, and frail based on the cardiovascular health study (CHS) frailty index. The plasma levels of HF markers, including tumorigenicity 2 (s-ST2), galectin-3, and heart-type fatty acid binding protein (H-FABP), were measured and correlated with frailty phenotype and cardiac function. The levels of plasma s-ST2, galectin-3, and H-FABP were profoundly elevated in CHF patients. Conversely, the frailty index scores were significantly lower in ischemic and non-ischemic CHF patients versus controls. Of the assessed HF markers, only H-FABP was positively correlated (r2 = 0.07, P = 0.02) with the frailty score in CHF patients. Collectively, these observations suggest that circulating H-FABP may serve as a biomarker of frailty in CHF patients.
Impact Statement
Frailty is often seen in patients with chronic heart failure (CHF). Here, we show, for the first time, significant associations of the established circulating heart failure marker with lower frailty index in CHF patients. More specifically, plasma heart-type fatty acid binding protein (H-FABP) level was found to be positively correlated with frailty in these patients. The level of galectin-3 was elevated in frail but not in pre-frail CHF patients. Consistently, frailty was found to be negatively correlated with cardiac contractile function and positively with cardiac morphometric parameters, including left ventricular (LV) posterior wall thickness and LV dimension.
Introduction
Frailty is characterized by fatigue, weakness, and increased vulnerability to exhaustion, which are common findings in patients with chronic heart failure (CHF). 1 Frailty also predicts mortality in cardiovascular diseases. 2 The cardiac stressors, including ischemic and non-ischemic conditions, promote adverse cardiac remodeling and progressive contractile dysfunction with compromised systemic blood supply.3–6 Therefore, CHF has systemic consequences, leading to gradual muscle weakness and atrophy, reduced aerobic capacity, and physical dependency.7–9 CHF patients also exhibit poor prognosis, reduced long-term survival, and a compromised aerobic capacity. Moreover, muscle wasting due to the systemic effect of CHF is also associated with a lower life expectancy. 10 Therefore, better characterization of the frailty indexes in patients with CHF is essential for overall better management and lifestyle.
The definition of frailty given by Freid et al. 11 for the clinical diagnosis is based on five indices. These include muscle weakness, slowness, reduced physical activity, self-reported exhaustion, and loss of body weight. 12 Muscle weakness is defined as low handgrip strength (HGS) for a given gender and body mass index (BMI). Slowness is defined as low gait speed over a specified distance for a given gender and BMI. Reduced physical activity is defined as a daily physical activity within the lowest quintile for the given gender. Self-reported exhaustion is defined as a feeling that “everything I did was an effort” and “I could not get going” within the past week. The loss of body weight is defined as losing >4.5 kg of body weight within the past 12 months. 12 The individuals with one or two indices are referred to as pre-frail and, with three or more indices, as frail. 13 This definition of frailty remains widely accepted in clinical practice.14,15 The cardiovascular health study (CHS) exhibits comparable diagnostic accuracy of frailty with other relevant assessment tools. 16 CHS is also valuable in predicting the risk of hospitalization and mortality.17,18 However, CHS is only applicable to ambulant participants due to the measurements of gait speed and physical activity. Therefore, it cannot be applied to the bedridden, wheelchair-bound, and/or uncooperative patients. Thus, bedside diagnostic and/or predictive markers of frailty are required. Several diagnostic criteria for frailty are proposed, including the widely accepted criteria for the elderly population by Rockwood et al. 19
Accumulating evidence suggests that the plasma proteomic changes in patients may be associated with accelerated frailty. For example, a recent study has reported increased levels of plasma haptoglobin, transferrin, and fibrinogen in pre-frail versus non-frail older adults. 20 Another study showed that the circulating angiotensinogen, kininogen-1, and antithrombin III levels may assist in monitoring the progression of frailty in older adults. 21 In addition, heart failure biomarkers may reflect physical capacity due to the systemic detrimental effects of heart failure. Considering the frequent occurrence of frailty in CHF patients, it is possible that the established heart failure markers may have associations with frailty, particularly in patients with CHF.
Several inflammatory, growth factors and muscle injury plasma biomarkers are correlated with the progression of cardiovascular diseases, including CHF.22–26 The expressions of inflammatory biomarkers, such as plasma galectin-3 and tumorigenicity 2 (s-ST2), are associated with the advancement of heart failure (HF).27,28 Furthermore, tissue injury markers, such as heart-type fatty acid binding protein (H-FABP), are also reported as a strong predictive marker of HF post-myocardial infarction. 29 Recently, we have reported that the plasma levels of H-FABP and galectin-3 negatively correlate with the physical performance of patients with CHF. 30 However, it is unknown whether these HF markers have any associations with frailty in patients with CHF.
The broader aim of this study was to evaluate the potential associations of HF markers H-FABP, s-ST2, and galectin-3 with the amount of frailty in patients with CHF. We report, for the first time, a robust inverse correlation of left ventricular ejection fraction (LVEF) and a positive correlation of LV posterior wall (LVPW) thickness with frailty in CHF patients. Of the assessed HF markers, the levels of plasma H-FABP exhibited positive correlations with frailty phenotype in patients with CHF.
Materials and methods
Study design and samples
We recruited 80 male patients with CHF (median age = 68 years) and 59 male controls (median age = 63 years) at the Hayatabad Medical Complex, Peshawar, Pakistan. Written informed consent was obtained from all participants. The clinical research ethics committee of the hospital provided the ethics approval for this study. LVEF < 50% was the inclusion criteria for patients with CHF. Patients with unstable angina, major organ failure, cardiac transplant, musculoskeletal disorders, recent surgeries, and/or chronic bed rest within the past eight weeks were excluded. All participants were Caucasian males, and the study was conducted according to the Declaration of Helsinki. 31
Echocardiography
We used the standard guidelines of the American Society of Echocardiography to perform two-dimensional (2D) echocardiography 32 and as described previously. 33 Briefly, the echocardiographic study was performed on all participants, and data were acquired using an ultrasonic system (Apollo i700, Canon Medical Systems, Beijing, China) and a 3 MHz probe. An M-mode tracing was recorded using the parasternal long-axis view, followed by the analysis of left ventricular interior dimensions, interventricular septal thickness (IVS), and posterior wall (LVPW) thickness. The system automatically calculated the LV contractile function, including left ventricular fractional shortening and LVEF.
Assessment of frailty
The CHS criteria were used to assess frailty based on five criteria, including muscle weakness, low walking speed, unintended weight loss, self-reported exhaustion, and reduced physical activity. 33 Patients who met 3–5 criteria were classified as frail, those with 1–2 criteria were classified as pre-frail, while the remaining patients were classified as robust, as described previously. 33
Plasma biomarkers
We collected blood sample from patients and control population in a vacutainer coated with an anticoagulant. Platelet-poor plasma was prepared as described previously. 34 The levels of HF markers were assessed in plasma using ELISA kits for Galectin-3 (Abcam #ab269555), H-FABP (Abcam #ab243682), s-ST2 (Abcam # 254505), and C-reactive proteins (CRP) (R&D Systems, Minneapolis, MN, USA) levels following the manual instructions.
Statistical analysis
The values were presented using mean and standard error of mean after confirming the normal distribution of the data. A one-way analysis of variance (ANOVA) followed by Tukey’s post hoc test was employed to compare the healthy controls with the two categories of CHF patients. We used simple regression analysis to evaluate the relationship among variables. Data were analyzed using GraphPad Prism 8.4, and the P-value < 0.05 was considered statistically significant.
Results
Characteristics of the study population
The recruited 80 patients included 56 ischemic and 24 non-ischemic patients, and 26 of them presented with diabetes mellitus, hypertension, and/or hypercholesterolemia. We recently reported the basic laboratory parameters and other phenotypic characteristics of these patients. 30 The echocardiographic investigations revealed significant LV chamber dilatation and LV contractile dysfunction in CHF patients with ischemic and non-ischemic heart failure (Table 1). The BMI was higher in both ischemic and non-ischemic CHF patients than in healthy controls. The level of plasma high-density lipoprotein (HDL) and erythrocyte sedimentation rate (ESR) were lower in the CHF patients compared to controls (Table 1).
Age, body composition, parameters of sarcopenia and physical performance, plasma biomarkers, and cardiac parameters in ischemic and non-ischemic heart failure patients in comparison to healthy controls.
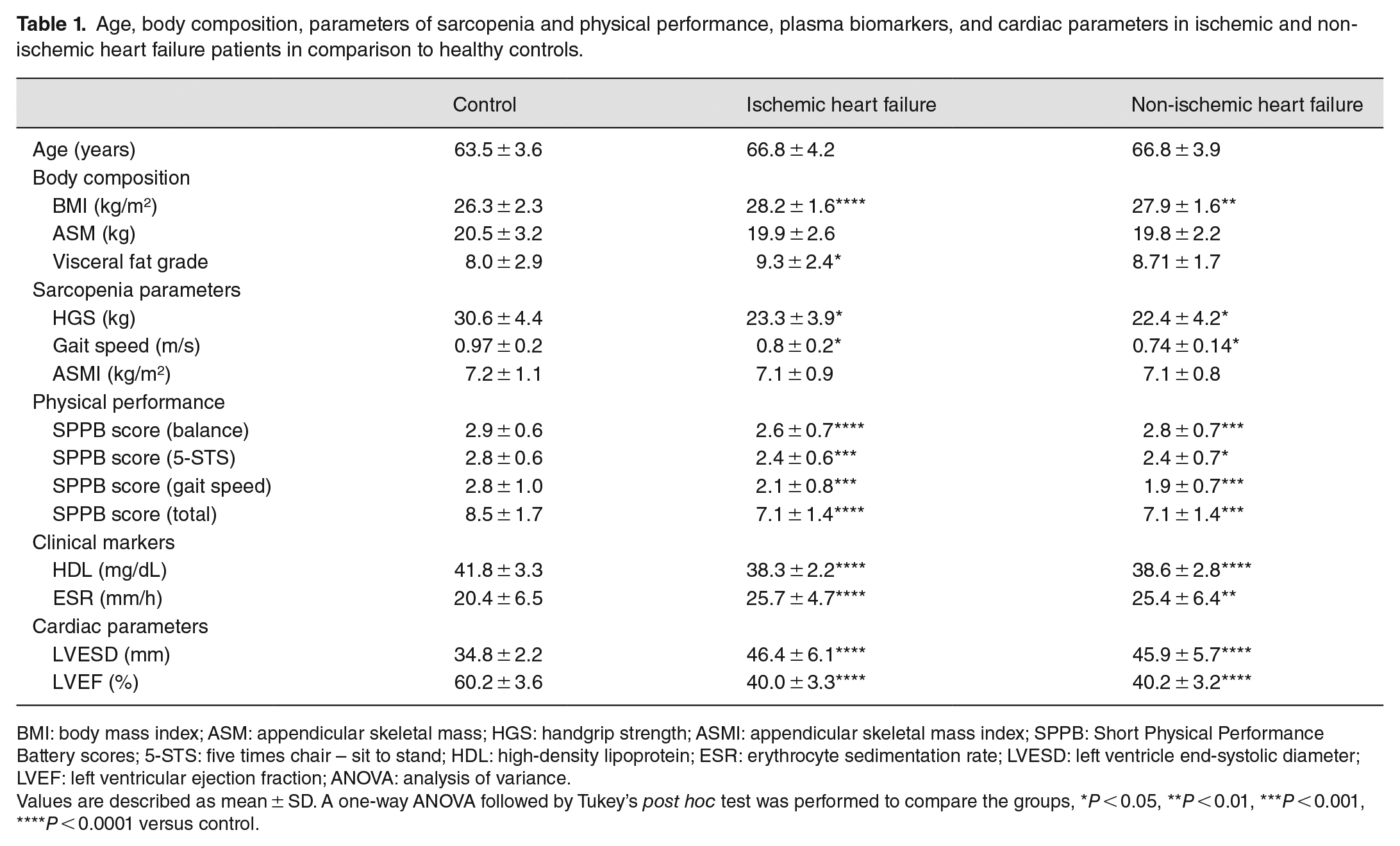
BMI: body mass index; ASM: appendicular skeletal mass; HGS: handgrip strength; ASMI: appendicular skeletal mass index; SPPB: Short Physical Performance Battery scores; 5-STS: five times chair – sit to stand; HDL: high-density lipoprotein; ESR: erythrocyte sedimentation rate; LVESD: left ventricle end-systolic diameter; LVEF: left ventricular ejection fraction; ANOVA: analysis of variance.
Values are described as mean ± SD. A one-way ANOVA followed by Tukey’s post hoc test was performed to compare the groups, *P < 0.05, **P < 0.01, ***P < 0.001, ****P < 0.0001 versus control.
Cardiac contractile dysfunction correlates with the frailty index in CHF patients
We assessed the frailty index and HF markers in the controls and CHF patients. As expected, the frailty index was significantly higher in CHF patients than in controls (Figure 1(A)). Next, we assessed the plasma levels of the HF markers in the study population. The galectin-3 levels were significantly elevated in the ischemic CHF patients versus controls (Figure 1(B)). However, the levels of plasma H-FABP and s-ST2 were significantly higher in both groups of CHF patients (Figure 1(C) and (D)). Finally, these patients also demonstrated higher CRP levels than controls (Figure 1(E)).
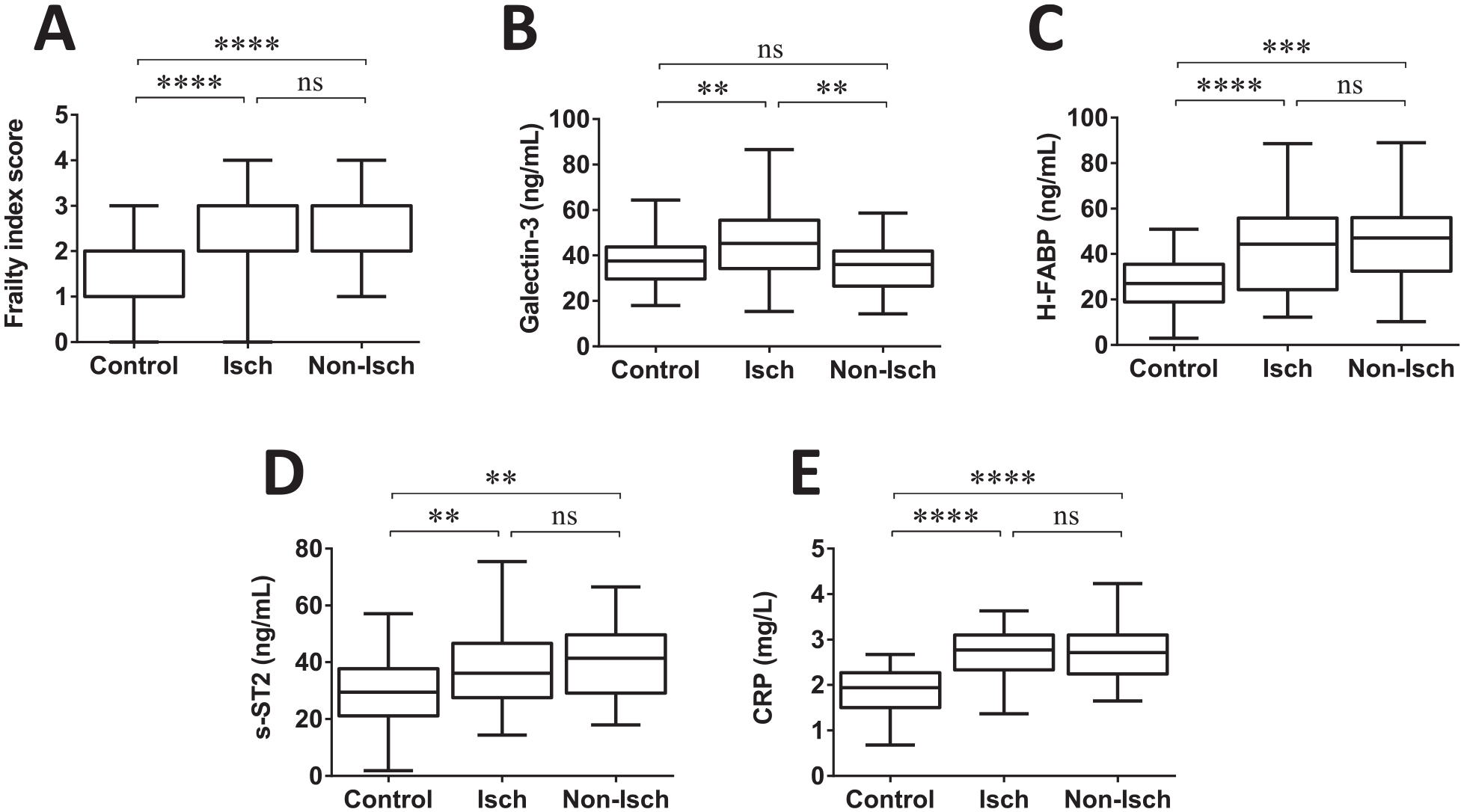
The plots show (A) frailty index, and levels of (B) galectin-3, (C) H-FABP, (D) s-ST2, and (E) CRP in healthy controls and patients with ischemic and non-ischemic heart failure. A one-way ANOVA followed by Tukey’s post hoc test was performed to compare the groups, **P < 0.01, ***P < 0.001, ****P < 0.0001, control, n = 53; CHF, n = 72–74.
Next, we analyzed potential associations between echocardiographic indices and frailty parameters in CHF patients. The cardiac contractile function, as measured by the LVEF, showed a robust negative correlation with the frailty index (Figure 2(A)). However, there was no significant correlation between LV end-systolic dimension (LVESD) and the frailty index (Figure 2(B)). Consistent with LVEF, cardiac hypertrophy (LVPW thickness) displayed a significant positive correlation with the frailty index in the patients with CHF (Figure 2(C)).
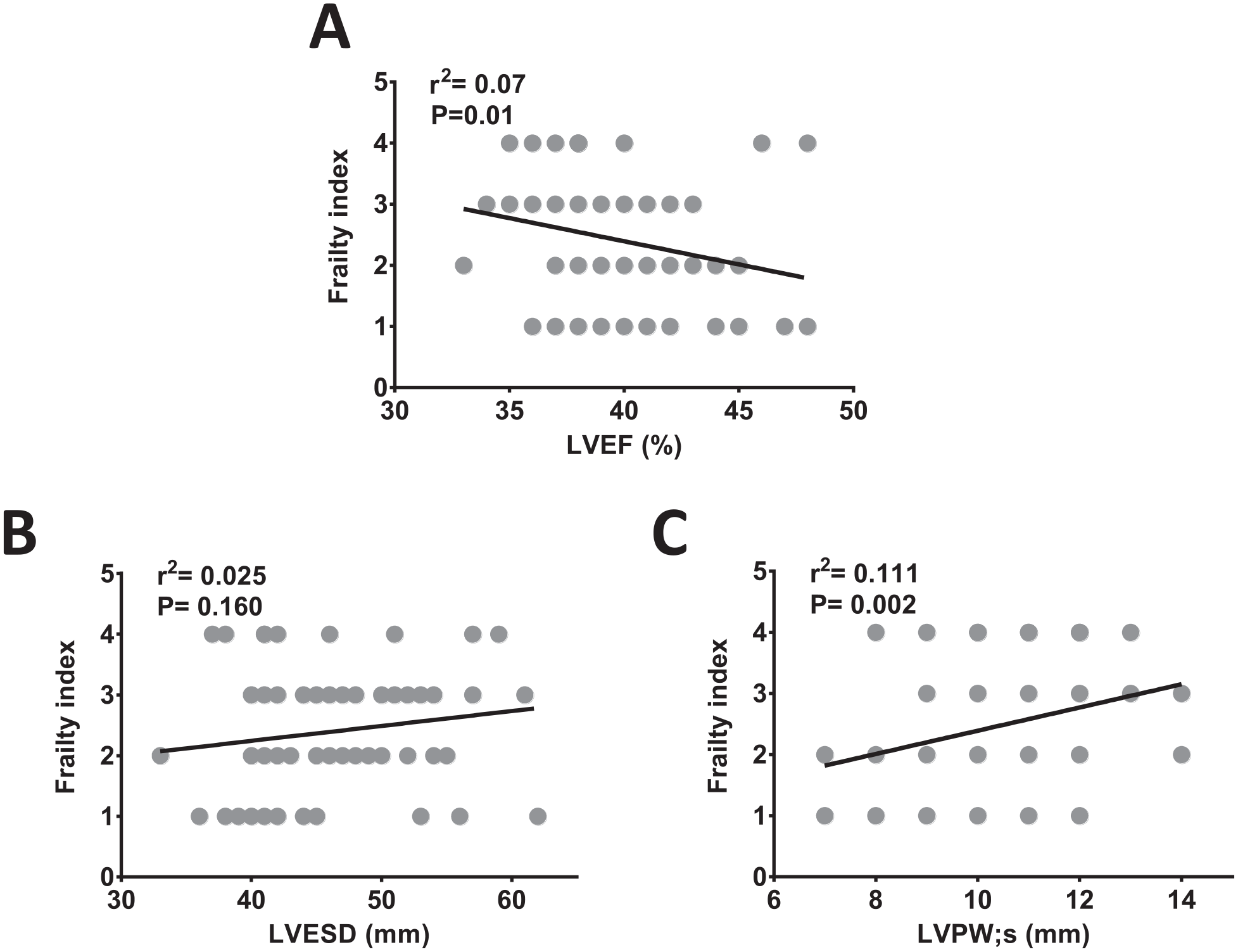
The correlation analysis of (A) LVEF, (B) LVESD, and (C) LVPW thickness with frailty index score in patients with CHF (n = 80).
Plasma H-FABP levels positively correlate with frailty in CHF patients
It is reported that the proteomic changes in the plasma of the geriatric population may have associations with the frailty index.20,21 However, it is unclear whether plasma biomarkers of HF predict the levels of frailty in CHF patients. In this series, we assessed the levels of plasma biomarkers of HF and correlated them with the frailty index of CHF patients. The plasma level of H-FABP displayed significant positive correlations with the frailty index in patients with CHF (Figure 3(A)). However, the levels of plasma s-ST2 and galectin-3 did not show any associations with frailty (Figure 3(B) and (C)). Consistently, the level of plasma CRP was also not associated with the frailty index (Figure 3(D)). These findings strongly suggest that plasma H-FABP may serve as a predictive frailty biomarker in CHF patients.
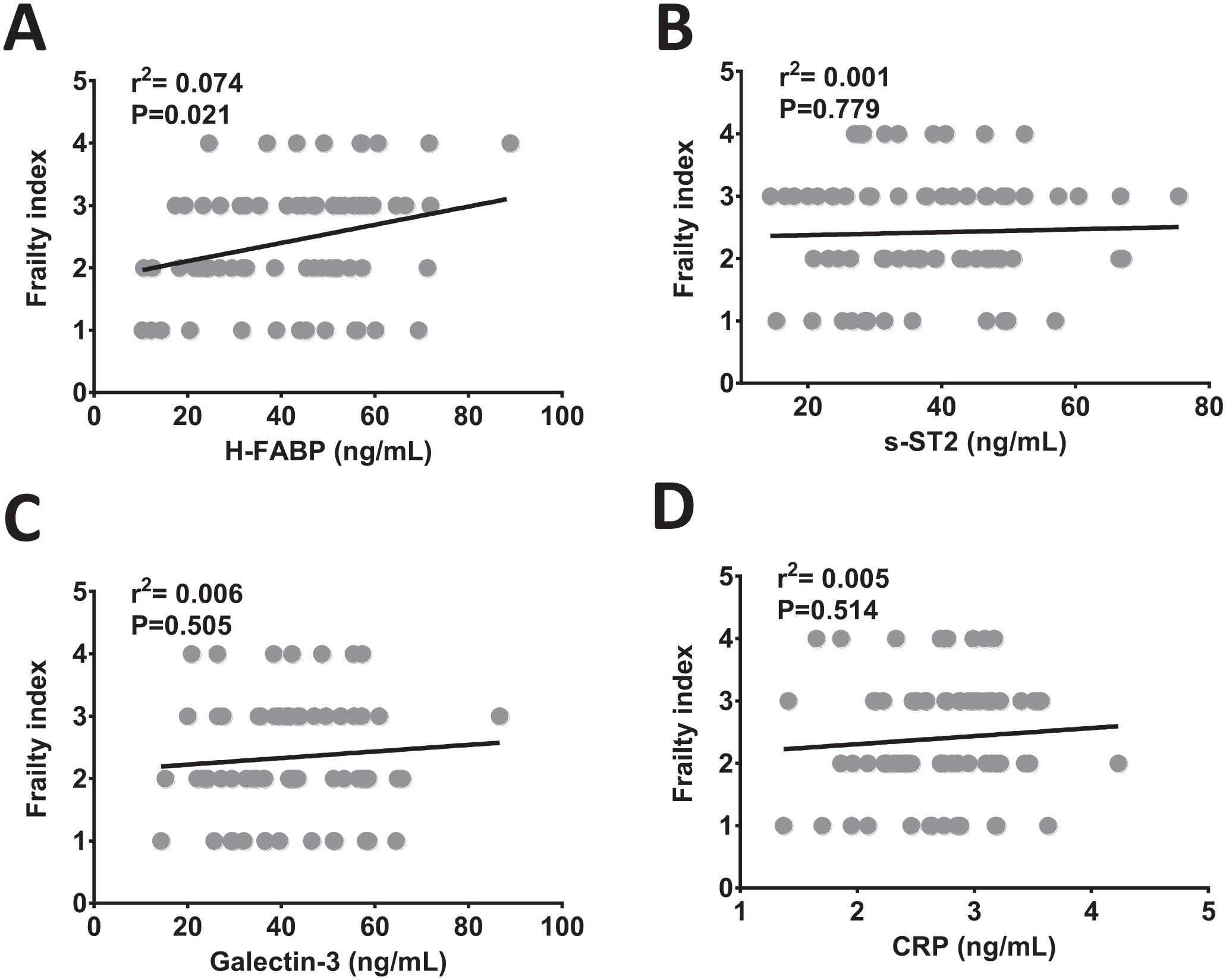
The correlation analysis of plasma (A) H-FABP (n = 74), (B) s-ST2 (n = 74), (C) galectin-3 (n = 72), and (D) CRP (n = 80) with frailty index score in CHF patients.
Plasma H-FABP negatively correlates with cardiac dysfunction in frail but not in pre-frail CHF patients
The potential associations of biomarkers H-FABP, s-ST2, galectin-3, and CRP with cardiac contractile function (LVEF) and cardiac hypertrophy (LVPW thickness) were assessed in pre-rail and frail CHF patients to understand the potential role of these biomarkers in frailty. The s-ST2 levels exhibited a robust inverse correlation with LVEF (r2 = 0.19, P = 0.004) in pre-frail but not in frail patients with CHF (Figure 4(A)). In contrast, plasma H-FABP levels were negatively correlated with LVEF in frail (r2 = 0.17, P = 0.01) but not in pre-frail patients (Figure 4(B)). Plasma galectin-3 was inversely correlated with LVEF in both groups but more profoundly in frail (r2 = 0.33, P = 0.0007) than pre-frail group (Figure 4(C)). Similar to galectin-3, plasma CRP was also negatively correlated with LVEF in both pre-frail (r2 = 0.23, P = 0.001) and frail (r2 = 0.20, P = 0.006) groups of CHF patients (Figure 4(D)).
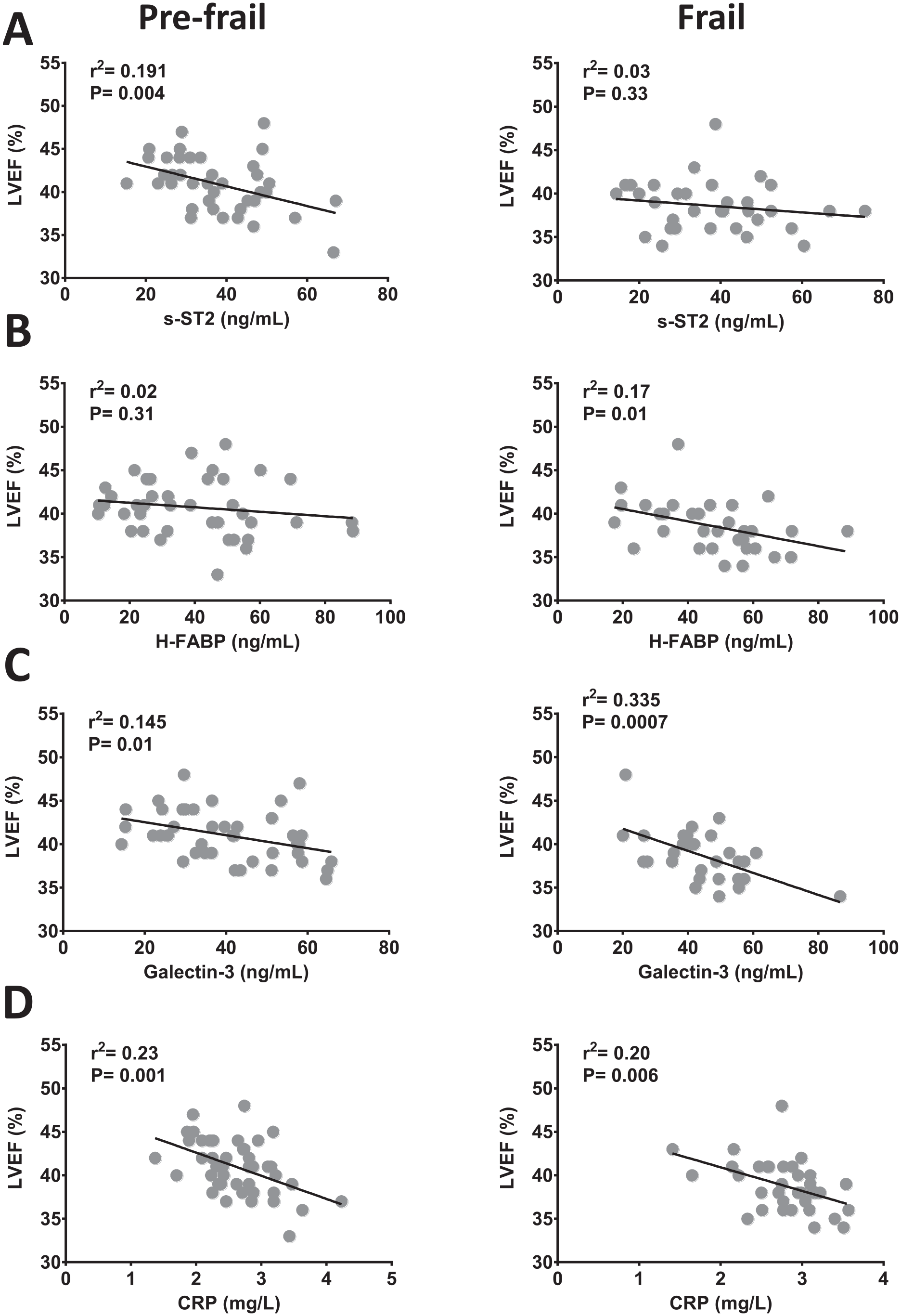
The correlation analysis of plasma (A) s-ST2 (n = 74), (B) H-FABP (n = 74), (C) galectin-3 (n = 72), and (D) CRP (n = 80) with left ventricular contractile function LVEF in pre-frail and frail patients with CHF.
Further investigations revealed a differential association pattern of circulating HF biomarkers with cardiac hypertrophy indicator LVPW thickness in pre-frail and frail patients with CHF. Thus, the plasma s-ST2 level was positively correlated with LVPW thickness in the pre-frail (r2 = 0.10, P = 0.04) but not in the frail group (Figure 5(A)). Similarly, plasma H-FABP exhibited a strong positive correlation with LVPW thickness in pre-frail (r2 = 0.20, P = 0.003) and but not in frail patients despite a trend toward significant association (Figure 5(B)). Conversely, plasma galectin-3 was not correlated with LVPW thickness in pre-frail and frail groups (Figure 5(C)). However, plasma CRP levels displayed a significant positive correlation (r2 = 0.14, P = 0.01) with LVPW thickness in pre-frail but not in frail patients with CHF (Figure 5(D)). Taken together, these findings suggest that s-ST2 is elevated in early pre-frail, H-FABP in frail, and galectin-3 and CRP both in pre-frail and frail stages of the CHF patients.
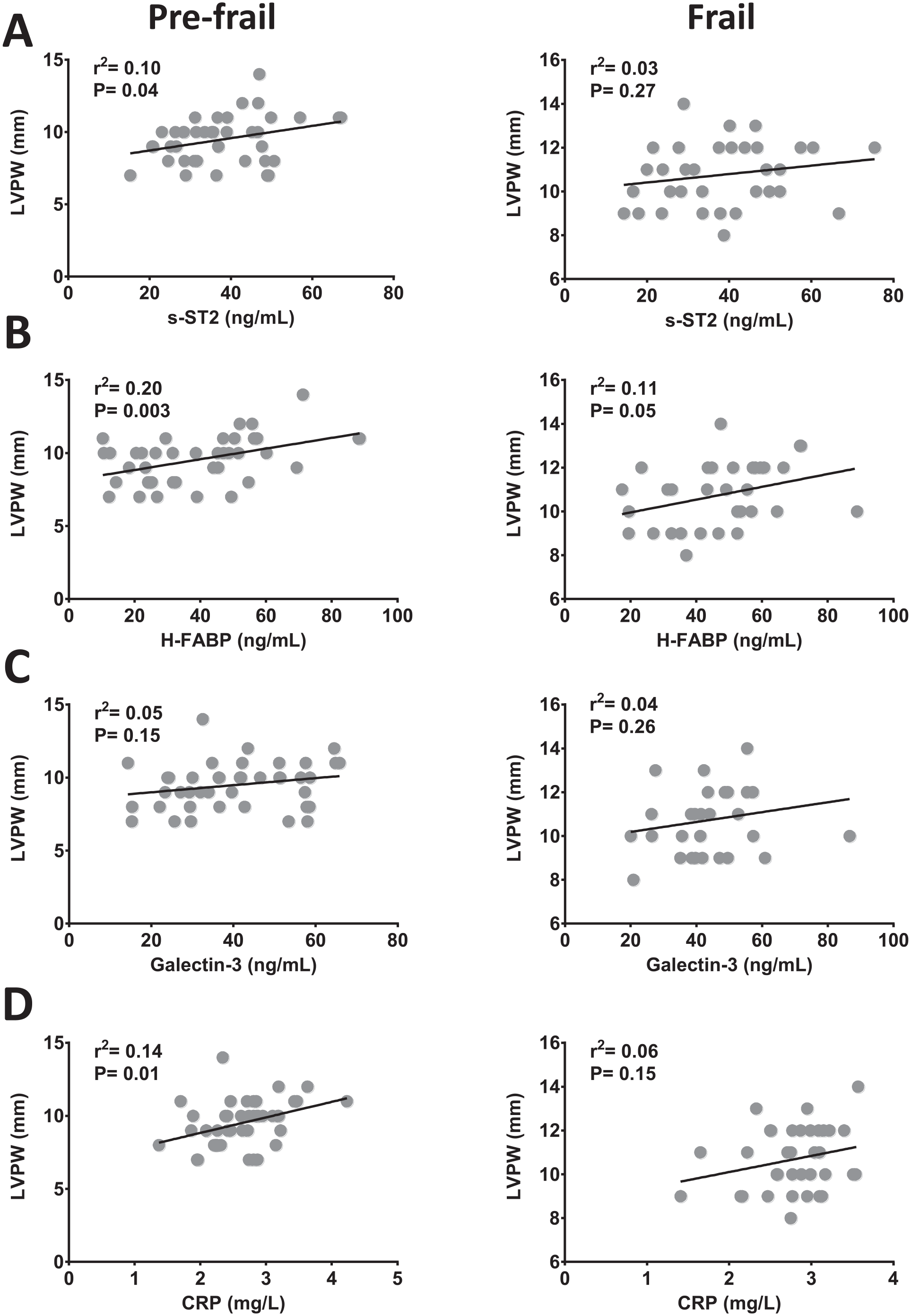
The graphs show correlations of (A) s-ST2 (n = 74), (B) H-FABP (n = 74), (C) galectin-3 (n = 72), and (D) CRP (n = 80) with LV posteriors wall (LVPW) thickness in pre-frail and frail patients with CHF.
Discussion
Frailty is commonly observed in the geriatric population, and accelerated frailty is often associated with CHF and other comorbidities.1,35 Here, we present, for the first time, that the frailty index directly correlates with the LV contractile function (LVEF) and cardiac hypertrophy (LVPW thickness) in patients with ischemic and non-ischemic CHF. The HF biomarkers plasma H-FABP, but not galectin-3, s-ST2, and CRP, exhibited robust positive correlations with the frailty index in CHF patients (Figure 6). Overall, these circulating proteins appeared to be better predictive markers of LV contractile function than hypertrophy in frail patients with CHF.
The schematic representation shows accelerated frailty in patients with chronic heart failure (CHF). The frailty was positively correlated with the heart failure marker H-FABP.
The changes in the levels of protein biomarkers in aging and pathological conditions are associated with accelerated frailty phenotype.20,21 Studies suggest that the crosstalk between proteomic biomarkers and various physiological pathways may govern frailty. 36 Irrespective of etiology, we observed a profound upregulation of plasma H-FABP in the recruited HF patients. The circulating H-FABP level was positively correlated with the frailty index. The positive correlation of H-FABP with LVPW thickness and no correlation with LVEF in pre-frail CHF indicate that H-FABP may be somehow associated with cardiac hypertrophy in pre-frail patients, leading to cardiac contractile dysfunction as evident by an inverse correlation of LVEF with H-FABP in frail patients. Moreover, H-FABP exhibited a positive correlation with the inflammatory marker CRP in CHF patients. Although no previous report links the circulating H-FABP with frailty in CHF patients, our finding indicates that H-FABP may be associated with the induction of systemic inflammation in CHF patients, which potentially facilitates accelerated frailty. Consistent with our observations, inflammatory markers interleukin-6 (IL-6), CRP, and IL-1RA have previously shown strong associations with weak muscle strength and compromised physical capability in the elderly population. 37 Another recent report has linked elevated levels of plasma CRP with poor physical ability. 38 Improved physical performance in athletes with the anti-inflammatory dietary intervention 39 further indicates the role of the H-FABP/inflammation nexus in the frailty of CHF patients.
The elevated plasma galectin-3 has been linked to poor outcomes in HF patients by many studies.40,41 Consistently, we observed higher galectin-3 levels, particularly in patients with ischemic HF. A study reported an independent association of plasma galectin-3 with frailty in geriatric patients with HF. 42 In contrast, we did not observe any association between plasma galectin-3 and frailty in patients with CHF. In this study, Komici et al. specifically focused on patients with systolic HF. However, our study cohort included ischemic and non-ischemic patients with systolic and diastolic dysfunction. This could be the potential reason for the differential observations on the association of galectin-3 with frailty in HF patients.
Previous studies reported robust associations of plasma sST2 with the severity and prognosis of HF.43,44 Consistently, we observed profound elevation of plasma sST2 in both ischemic and non-ischemic CHF patients. In our study, the levels of sST2 have shown consistent correlations with cardiac contractile dysfunction, LV remodeling (LVESD), and hypertrophy. Importantly, studies suggest that the levels of sST2 may also serve as a potential predictive biomarker for frailty in patients with HF and other critical illnesses.45,46 However, we did not observe any association of sST2 with either physical performance parameters or overall frailty in patients with CHF. Hence, sST2 may contribute to disease severity due to its crucial role in inducing systemic inflammation but may not be a predictive biomarker of frailty in critically ill patients.
The major strength of our study is the monocentric nature, which was particularly focused on male patients. It limits several confounding factors related to gender, lifestyle, race, and evaluation techniques. However, the inclusion of only male patients may also be a limiting factor due to potential gender-specific alterations in the levels of assessed biomarkers. We did not take the history of inflammatory conditions in the recruited patients, which may also affect the levels of assessed markers.
Collectively, here we report strong associations of LVEF and LVPW thickness with frailty in CHF patients. The H-FABP level was significantly induced in both pre-frail and frail patients compared to controls. The levels of circulating H-FABP exhibited a negative correlation with LVEF in frail patients and positive correlations with LVPW thickness in pre-frail patients with CHF. The frailty index was positively correlated with H-FABP levels but not with sST2 levels, galectin-3, and CRP in patients with CHF. These findings suggest that circulating H-FABP potentially serves as a biomarker of frailty in the advanced stage of HF.
Footnotes
Authors’ Contribution
Conceptualization: RQ and FA; Data curation: RQ, AK, JK, and FA; Formal analysis: RQ and FA; Funding acquisition: RQ and FA; Investigation: RQ, AK, JK, and FA; Methodology: AK and JK; Project administration: RQ, AK, JK, and FA; Resources: RQ, AK, JK, and FA; Supervision: AK and JK; Validation: RQ, AK, JK, and FA; Writing – original draft: RQ and FA; Writing – review & editing: RQ and FA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by a Collaborative (22010901112) grant to Firdos Ahmad and a competitive (22010901121) grant to Rizwan Qaisar from the University of Sharjah.
Ethical Approval
The ethical approval for the study was obtained from the local ethics committee.