
Abstract
Preeclampsia increases the risk of pregnancy-related complications, nevertheless a successful spiral vessel remodeling, and trophoblast invasion reduces disorders of pregnancy. Matrix metalloproteinase-2 (MMP-2) clears the path for trophoblast invasion, and activation of MMP-2 largely depends on extracellular matrix metalloproteinases inducer (EMMPRIN) protein. This study aimed to investigate EMMPRIN gene polymorphism and MMP-2 activity in preeclampsia patients. Archival whole blood and serum samples of 74 preeclampsia and 66 normotensive pregnant women age-matched were used in this case–control study. Genomic DNA was extracted from the whole blood samples and EMMPRIN gene amplified with specific primers following fragments sequence mutation analysis. Serum MMP-2 activity was determined using enzyme-linked immunosorbent assay (ELISA) and socio-demographic data of participants retrieved from the database. Age of preeclampsia patients (32.78 ± 6.39) years and body mass index (BMI) (33.09 ± 7.27) kg/m2 compared with the normotensive counterparts (32.33 ± 5.56) years and (32.33 ± 5.56) kg/m2,respectively, were not statistically significant (P > 0.05). Serum matrix metalloprotease-2 (MMP-2) activity was significantly reduced in preeclampsia group (16.34 ± 7.07) compared with the normotensives (25.63 ± 4.56) (P < 0.001), and rs424243T/G variant (55.6%) was overrepresented among the cases compared with the normotensives (16.7%). The single-nucleotide polymorphism T/G was found to be associated with preeclampsia (odds ratio [OR] = 7.63; 95% confidence interval [CI] = 3.95–14.75; P < 0.0001). Decreased activity of MMP-2 and rs424243T/G SNP of EMMPRIN gene was reported in preeclampsia. These preliminary data warrant a further investigation into the relationship between EMMPRIN gene polymorphism and MMP-2 activity in preeclampsia.
Impact statement
Preeclampsia is pregnancy-related disorder which affects multiple organ systems. The etiology of the disorder is not clear; however, abnormal placental implantation and defective spiral artery remodeling have been implicated. The extracellular matrix metalloproteinases inducer (EMMPRIN) protein activates matrix metalloproteinase-2 (MMP-2) to clear the path for trophoblast invasion. EMMPRIN gene polymorphism may affect MMP-2 activation and trophoblast implantation. We study EMMPRIN gene polymorphism and MMP-2 activity in preeclampsia patients. Serum MMP-2 activity was significantly reduced, and rs424243T/G variant overrepresented among the patients compared with the normotensives. The single-nucleotide polymorphism T/G was found to be associated with preeclampsia. This preliminary data will drive further investigation to establish a relationship between EMMPRIN gene polymorphism and MMP-2 activity in preeclampsia. The relationship has the potential of identifying women who may be at risk of preeclampsia.
Introduction
Preeclampsia (PE) is a pregnancy-related, heterogeneous disorder that affects multiple organ systems; however, no definite etiology has been established up to date. 1 It is characterized by hypertension (systolic blood pressure ⩾140 mmHg and/or diastolic blood pressure ⩾90 mmHg) in a previously normotensive woman and an elevated concentration of protein in urine (⩾300 mg/24 h) after 20 weeks of gestation term. 2 Globally, prevalence of PE was estimated at 4.6% in 2013 with higher burden occurring in developing countries, accounting for approximately 2–8% of pregnancy complications worldwide.3–5
Even though the exact etiology of PE is unclear, factors including nulliparity, age, family and previous history, obesity, multifetal gestation, conditions leading to hyper-placentation and large placentas, and pre-existing chronic hypertension, gestational diabetes, renal disease, autoimmune disease, and ethnic variants of single-nucleotide polymorphism have been implicated in the condition.6,7 Abnormal placental implantation and defective spiral artery remodeling are the major pathophysiology underlying PE.8,9
Physiologically, spiral artery remodeling in early pregnancy reduces the resistance to utero-placenta blood flow, permitting sustained and adequate blood flow to the placenta and hence the fetus. 10 Defective placental implantation is characterized by reduced perfusion of the uterus and placenta, 11 and elevated levels of anti-angiogenic proteins (sFlt-1) in circulation of the mother. 12 Within 8–18 weeks of gestation, trophoblasts invade the uterus by attaching to the extracellular matrix (ECM), and degradation of the matrix and successful migration of trophoblasts ensure adequate contact with maternal blood supply. 13
A variety of factors expressed within the uterine cavity and on the trophoblasts, such as matrix metalloproteinases (MMPs), tightly control the invasive behavior of trophoblast into the endometrium and labor activation at full term.14,15 MMPs are a group of 28 structurally related family of zinc-dependent proteases which are regulated by five mechanisms: gene transcription, secretion, activation, inhibition, and glycosylation. 16 MMPs are secreted into the ECM as zymogens which require activation through cleavage. 17 A study reported low levels of MMP-2 and MMP-9, and high levels of tissue inhibitors of matrix metalloproteinases (TIMPs) in PE. 18 Balanced secretion of MMPs and TIMPs is implicated in normal spiral artery remodeling and altered levels have been associated with PE, intrauterine growth restriction (IUGR), and miscarriage.19,20
Extracellular matrix metalloproteinases inducer (EMMPRIN), also known as basigin (BSG) and CD147, is expressed on different cell types including epithelial, endothelial, hematopoietic, tumor, and T lymphocyte cells. EMMPRIN protein was reported to activate MMP-2 and MMP-9;21–23 thus, EMMPRIN serves as a key factor in trophoblast implantation through MMPs-mediated ECM degradation and endometrium invasion. EMMPRIN is a transmembrane glycoprotein and belongs to the superfamily of immunoglobulins. 23 The 1797 bp EMMPRIN gene is located on chromosome 19p13.3 and encodes 269 amino acids with a heavy extracellular N-terminal, transmembrane and intracellular sequences. The two extracellular immunoglobulin-like structures are required for the activation of metalloproteases.12,24
EMMPRIN gene is highly polymorphic and variants such as rs4919859, rs4682, rs8637 rs8259, rs2283574, rs6757, rs4919862, rs6758, and rs28915400 have been implicated in disease conditions.25,26 From our global literature search, no information exists on EMMPRIN gene polymorphism and MMP-2 activity in patients diagnosed with PE. Therefore, current preliminary study aimed to investigate EMMPRIN gene polymorphism and MMP-2 activity in patients diagnosed with PE.
Materials and methods
Archival whole blood and serum samples, and clinical characteristics and medical history records, that were collected from 74 PE and 66 normotensive pregnant women attending antenatal clinic at Korle Bu Teaching Hospital in the southern part of Ghana were used for the study. Pregnant women ⩾20 weeks gestation and diagnosed with hypertension (blood pressure ⩾140 mmHg systolic or ⩾90 mmHg diastolic and proteinuria were included. Normotensives are pregnant woman at ⩾20 weeks of gestation with no sustained hypertension (blood pressure < 140 mmHg systolic or <90 mmHg diastolic) and without proteinuria at time of recruitment confirmed by urine strip test. Women with multiple gestation and pre-existing chronic conditions, including diabetes, hypertension, cardiovascular disease, and HIV and hepatitis infections, were excluded.
Genomic DNA was extracted from whole blood samples using Quick-DNA™ Microprep Kit (Zymo Research, Irvine, CA 92614, USA) following manufacturer’s protocol. The concentration of DNA was determined using NanoDrop 2000/2000c (Thermo Fisher Scientific, Waltham, MA 02451, USA ) spectrophotometer and stored at −20°C until ready to use. The EMMPRIN gene was amplified from the genomic DNA samples by polymerase chain reaction (PCR) using the following primer set; forward: 5′-GAGTCCACTCCCAGTGCTTG-3′ and reverse: 5′-CTCGTGAAACACTTCAGAAGGAAAAGA-3′, and a ready-to-use OneTaq Quick-Load 2X Master Mix (BioLabs Inc., Lpswich, MA 01938, New England) following the manufacturer’s reaction conditions. A 25-μL PCR reaction mixture has the components and final concentration: 1× reaction buffer, 0.5 μM each of the forward and reverse primers, and 0.1 μg/μL genomic DNA. The reaction volume was obtained by adding nuclease-free water. The reaction mixture was subjected to an initial denaturation at 94°C for 30 s, 30 cycles of denaturation at 94°C for 30 s, annealing at 58°C for 1 min, and extension at 68°C for 1 min. Final extension was performed at 68°C for 5 min. The PCR amplifications were carried out using the Techne Prime Thermal Cycler (Bibby Scientific, Essex, CM2 6UN, UK) and the amplicons were separated on 1.5% agarose gels with ethidium bromide in Tris-acetate-EDTA (TAE) buffer. A 100-bp molecular weight ladder was used to determine the size of the bands.
Part of the amplicons of randomly selected samples of patients diagnosed with PE and normotensives were sent for commercial sequencing (Inqaba, Nigeria). The chromatograms were analyzed and the nucleotide sequences in FASTA format aligned with gene sequences in NCBI GenBank database using Align Sequences Nucleotide BLAST platform to determine the sequence similarities with human EMMPRIN gene.
Serum MMP-2 activity in patients and normotensives was measured by a sandwich enzyme immunoassay technique using Amersham Matrix Metalloproteinase-2, Biotrak™ Activity Assay System kit (GE Healthcare Bio-Sciences Corp, Piscataway, NJ, USA) following manufacturer’s protocol. A Varioskan LUX multimode microplate reader (Thermo Scientific™, Waltham, MA 02451, USA) operating on the SkanIt™ software was used to read absorbance at 405 nm. All samples were measured in duplicates and the mean value calculated was used for data analysis. A calibration curve and blank were run for the test plate.
All analyses were performed with SPSS software (version 24.0; SPSS Inc., Chicago, IL, USA). Continuous variables were presented as mean ± SD and categorical data were presented as percentages. Student’s t test was used for comparison of continuous variables, and odds ratio (OR) was used to determine association between the categorical variables. P < 0.05 was considered statistically significant.
Results
The clinical parameters of the study participants are presented in Table 1. There was no significant difference between the mean (±SD) ages of the PE and normotensive pregnant women (32.33 ± 5.56 versus 32.78 ± 6.39) years. The blood pressures, both systolic and diastolic, of the PE women were significantly higher than their normotensive counterparts (P < 0.001), whereas body mass index (BMI) and gestational age showed no significant difference between the study groups (P > 0.05). There were varying degrees of proteinuria among the PE women, and greater proportion of the patients showed about 300 mg/24 h or 1+ urine protein.
Clinical variables of study participants.
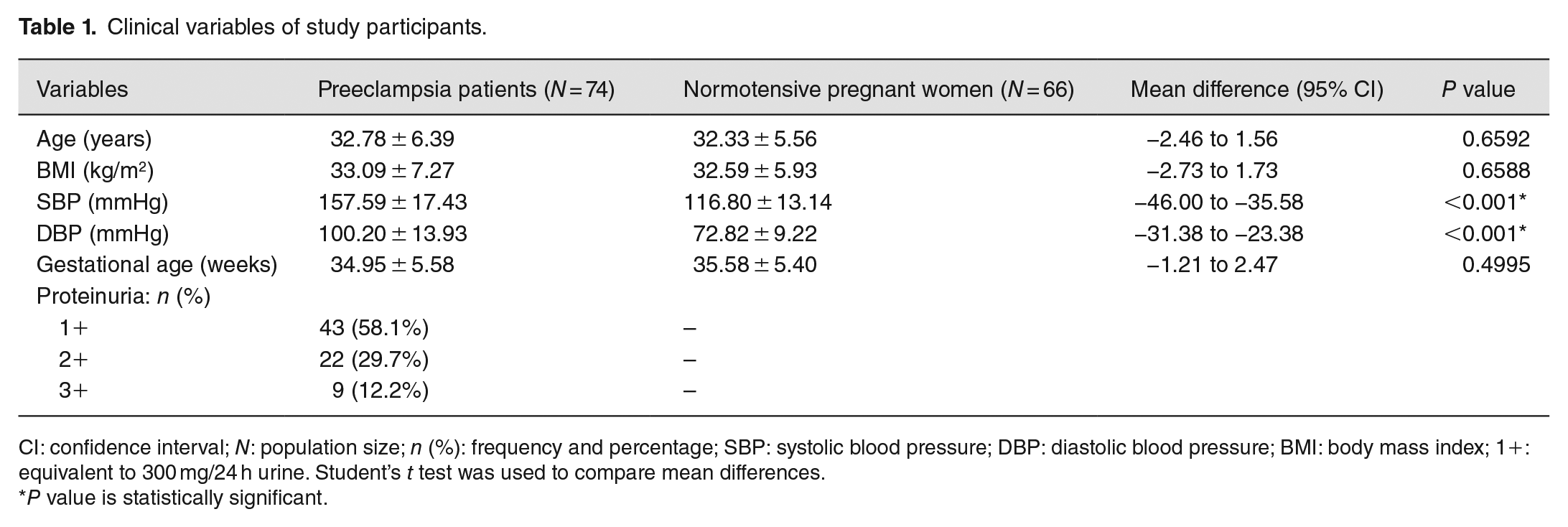
CI: confidence interval; N: population size; n (%): frequency and percentage; SBP: systolic blood pressure; DBP: diastolic blood pressure; BMI: body mass index; 1+: equivalent to 300 mg/24 h urine. Student’s t test was used to compare mean differences.
P value is statistically significant.
Serum activity of MMP-2 was significantly reduced in the PE pregnant women compared with their normotensive counterparts (P < 0.001) (Figure 1). EMMPRIN gene 3′-untranslated region chromatograms showed either T/T wild-type or T/G genotypes (Figure 2), and alignment of the gene sequence with reference (AP023479.1) presented a rs424243T/G (Figure 3). The genotype T/G was overrepresented among the PE patients (61.1%), while the T/T genotype was significantly higher in the 83.3% normotensives than the patients, and the genotype rs424243T/G was statistically associated with PE (OR = 7.85, P < 0.05) (Table 2).
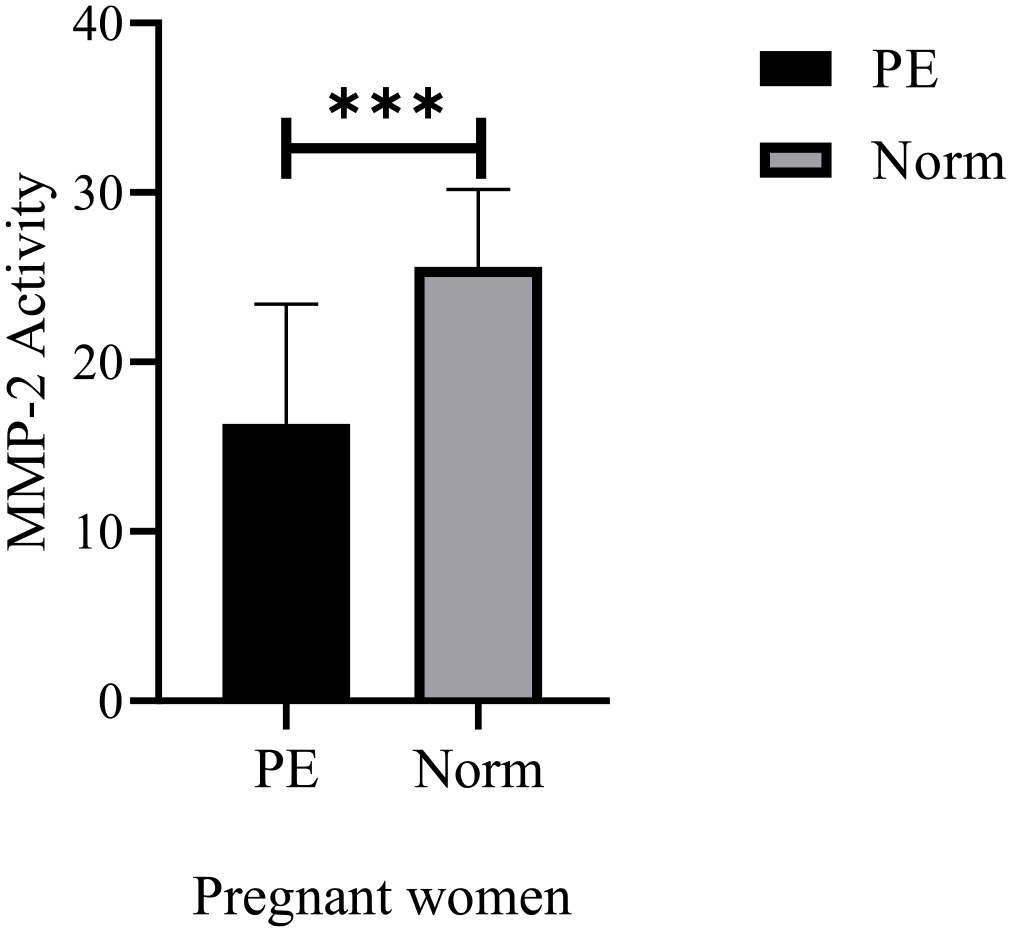
Preeclampsia (PE), normotensive pregnant women (Norm).
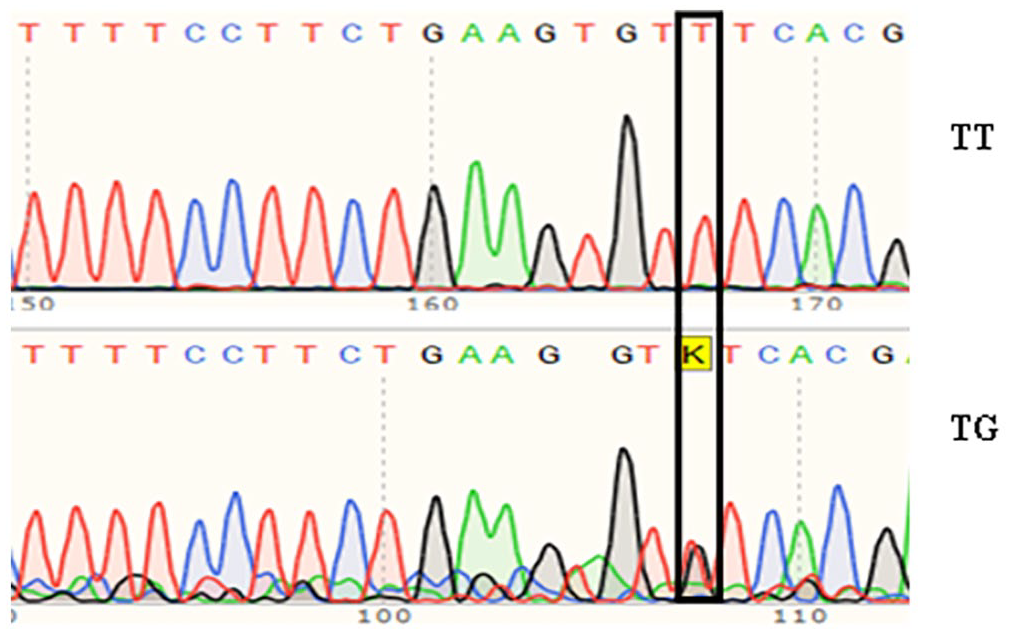
The K (T/G) SNP was predominant in PE-affected patients than normotensives.
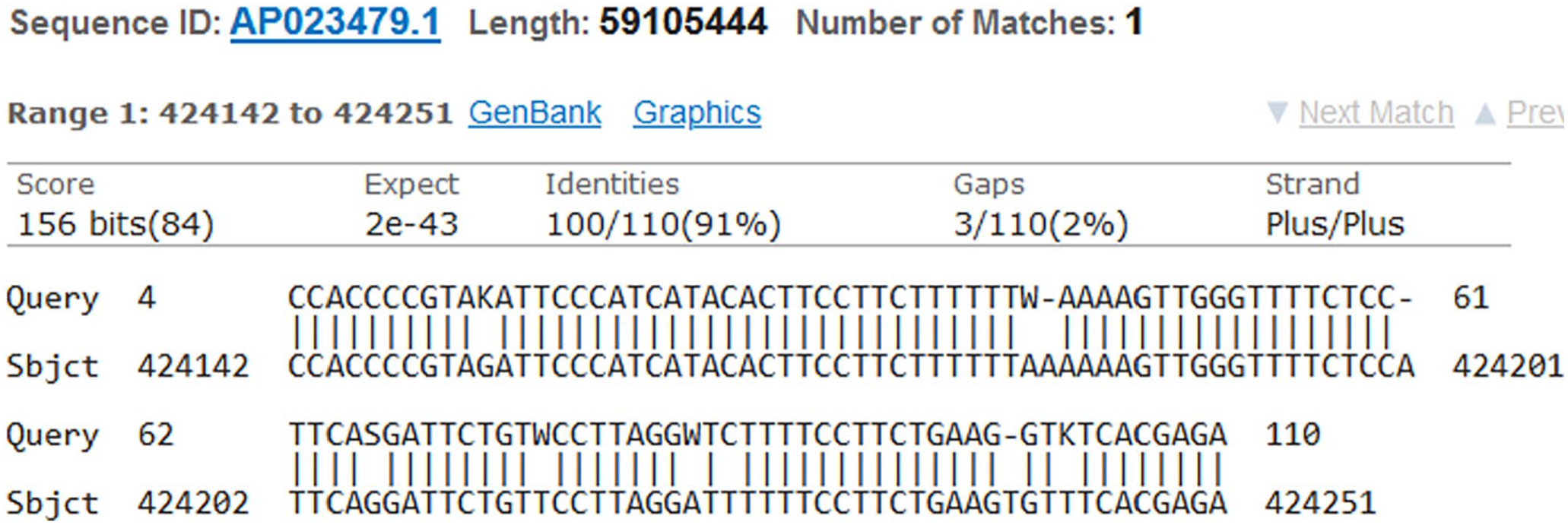
The trimmed sequences obtained from the patients aligned within the region of 424142 to 424251 of the human chromosome 19 (AP023479.1) reference sequence obtained from the NCBI database.
Association of EMMPRIN gene rs424243 single-nucleotide polymorphism with preeclampsia.
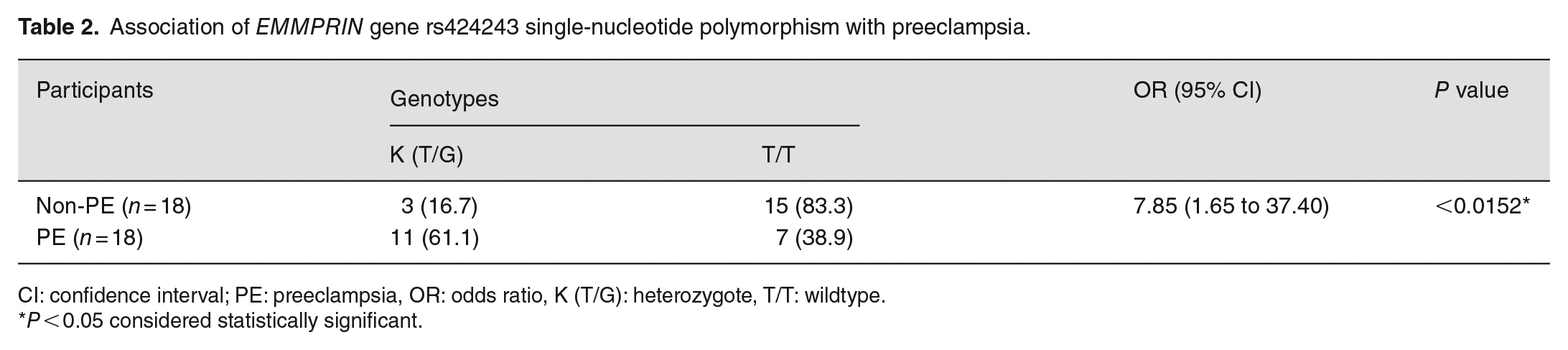
CI: confidence interval; PE: preeclampsia, OR: odds ratio, K (T/G): heterozygote, T/T: wildtype.
P < 0.05 considered statistically significant.
Discussion
Patients diagnosed with PE carried EMMPRIN gene rs424243T/G variant, and the polymorphism increased the risk of PE. To the best of our knowledge, this case–control study is first to establish an association between the EMMPRIN gene polymorphism and PE. Although the role of the identified single-nucleotide polymorphism in the patients is not clear, variants of the gene have been implicated in pathogenesis of several human diseases,27,28 and the link was attributed to the physiological functional regulation of the gene. The EMMPRIN as a type I integral receptor binds to several ligands, 27 and the extracellular immunoglobulin-like structures are crucial for trophoblast invasion and prevention of pregnancy-related complications through induction of metalloproteases.
This study reports decreased activity of MMP-2 in pregnant women diagnosed with PE compared with pregnant women without PE. This result supports earlier study that showed a reduced MMPs activity in PE patients. 29 A decreased MMP-2 activity has been implicated in poor degradation of the ECM, inadequate remodeling of spiral arteries, and restriction of uterine growth and expansion. 30 It has been demonstrated that decreased MMP-2 expression negatively affected endocrine gland–derived vascular endothelial growth factor–induced trophoblast invasion. 31
Interestingly, other studies have shown higher serum MMP-2 levels in PE-affected pregnant women than their normotensive counterparts. 32 The increase level of MMP-2 and associated PE could be explained probably by imbalanced activity of the enzyme and low level of TIMPs as implicated in cancer metastasis. 28 Although MMP-2 proteolytic activity is tightly controlled under normal conditions to prevent tissue destruction, factors including plant extracts and sedentary lifestyle could affect expression level and imbalanced proteolytic activity of the enzyme.33,34
This study supports previous research that showed an elevated blood pressure and urine protein in women with PE. 35 Hypertension is both a risk factor and a consequence of PE; however, pregnant women with pre-existing hypertension are more at risk of developing PE. 36 Other risk factors associated with PE include family history, nulliparity, multiple gestation, history of diabetes, obesity, age of mother, impaired glucose tolerance, cesarean delivery, and race.36–38 However, this study showed no significant difference between the mean BMI, age, and gestational age when PE-affected women were compared with the normotensive counterparts. Pre-pregnancy BMI and gestational weight gain have been reported as independent risk factors for PE, and obesity has been suggested to be a useful diagnostic index. 39
Greater proportion of the patients showed a minimal 300 mg/24 h urine protein (proteinuria 1+). Urine protein levels have been linked with worse pregnancy outcomes, and these include delivery nearly 2 weeks earlier, higher rates of cesarean section, pre-labor cesarean section, and requirement for magnesium sulfate, and the levels could be used as a surrogate marker for more severe disease. 39 Comparatively, pregnant women diagnosed with proteinuria show increased risk of pregnancy complications than those who have been diagnosed with chronic or gestational hypertension but without proteinuria. 39 The small sample size remains the main limitation of this study. Association between MMP-2 activity, other risk factors of PE, and the gene polymorphism were not determined due to the small sample size for this study. Another limitation is that the assays used in this study have not been validated for clinical applications.
Conclusions
This preliminary study reports EMMPRIN gene variant rs424243 SNP and a decreased activity of MMP-2 in women with PE compared with normotensive counterparts. Further study with larger sample size is required to establish an association between the gene polymorphism and MMPs activity and other risk factors of PE.
Footnotes
Acknowledgements
We thank all patients who participated in the study and members of the Virology Laboratory, Department of Biochemistry, Cell and Molecular Biology, West African Centre for Cell Biology of Infectious Pathogens, University of Ghana for their support in running the assays.
Authors’ Contributions
EAT and OQ design the work; DA and POG conducted the experiments; EAT, OQ, and SS analyzed data and interpreted the study; DA, POG, KA-B, and NAA wrote the manuscript. All authors reviewed the manuscript and approved the submitted version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical clearance was obtained from the Ethical and Protocol Review Committee of the School of Biomedical and Allied Health Sciences, College of Health Sciences, University of Ghana with ethics identification no. SBAHS/AA/MLAB/10667713/2022-2021.