
Abstract
Leprosy is a neglected chronic infectious disease caused by obligate intracellular bacilli, Mycobacterium leprae and Mycobacterium lepromatosis. Despite multidrug therapy (MDT) success, leprosy accounts for more than 200,000 new cases yearly. Leprosy diagnosis remains based on the dermato-neurologic examination, but histopathology of skin biopsy and bacilloscopy of intradermal scraping are subsidiary diagnostic tests that require expertise and laboratory infrastructure. This minireview summarizes the state of the art of serologic tests to aid leprosy diagnosis, highlighting enzyme-linked immunosorbent assay (ELISA) and point-of-care tests (POCT) biotechnologies. Also, the impact of the postgenomic era on the description of new recombinantly expressed M. leprae–specific protein antigens, such as leprosy Infectious Disease Research Institute (IDRI) diagnostic (LID)-1 is summarized. Highly specific and sensitive molecular techniques to detect M. leprae DNA as the quantitative polymerase chain reaction (qPCR) and the loop-mediated isothermal amplification (LAMP) are briefly reviewed. Serology studies using phenolic glycolipid-I (PGL-I) semi-synthetic antigens, LID-1 fusion antigen, and the single fusion complex natural disaccharide-octyl (NDO)-LID show high sensitivity in multibacillary (MB) patients. However, serology is not applicable to paucibacillary patients, as they have weak humoral response and robust cell-mediated response, requiring tests for cellular biomarkers. Unlike ELISA-based tests, leprosy-specific POCT based on semi-synthetic PGL-I antigens and NDO-LID 1 antigen is easy to perform, cheaper, equipment-free, and can contribute to early diagnosis avoiding permanent incapacities and helping to interrupt M. leprae transmission. Besides its use to help diagnosis of household contacts or at-risk populations in endemic areas, potential applications of leprosy serology include monitoring MDT efficacy, identification of recent infection, especially in young children, as surrogate markers of disease progression to orient adult chemoprophylaxis and as a predictor of type 2 leprosy reactions. Advances in molecular biology techniques have reduced the complexity and execution time of qPCR confirming its utility to help diagnosis while leprosy-specific LAMP holds promise as an adjunct test to detect M. leprae DNA.
Impact Statement
Early detection and treatment are imperative to interrupt transmission and eliminate leprosy. Advances, limitations, and remaining challenges of traditional methods (histopathology, bacilloscopy), serologic and molecular tests to aid leprosy diagnosis are discussed. The most investigated and best standardized serologic tests use phenolic glycolipid-I (PGL-I) Mycobacterium leprae–specific antigen. Since the post genomic era, new recombinant protein antigens and fusion versions, such as leprosy Infectious Disease Research Institute (IDRI) diagnostic (LID-1), have been widely tested. The use of semi-synthetic PGL-I antigens coupled with hydrophilic protein carriers allowed the development of fast, low-cost, reproducible immunochromatography point-of-care tests (POCTs), such as the ML Flow. This test has been recently incorporated by the Brazilian Unified Health System (SUS) as an auxiliary serologic diagnostic test for leprosy contacts, as well as a polymerase chain reaction (PCR)–based technique to detect M. leprae DNA. The development of new platforms associating M. leprae molecular test and the POCT technologies can yield improved diagnostic tests for paucibacillary and multibacillary leprosy.
Introduction
Leprosy is a chronic granulomatous infectious disease caused by Mycobacterium leprae or Mycobacterium lepromatosis that affects predominantly the skin and peripheral nerves causing skin lesions, loss of sensation, and nerve damage that lead to permanent physical and social disabilities1–3 The transmission of M. leprae is considered to occur mainly through the upper airways requiring long and close contact with an untreated leprosy case, especially with high bacillary load. 4 The incubation period is long, on average 5 years, but often takes much longer and only a small percentage (estimated 5%) of individuals infected with M. leprae actually develop disease. 5 Leprosy is a neglected tropical disease associated with poverty, precarious housing and food, and persistent socio-economic inequalities that hamper leprosy control as a public health problem.
Although leprosy represents one of the most ancient human infectious diseases and despite the success of multidrug therapy (MDT) in reducing the number of registered leprosy cases worldwide, leprosy still occurs in around 120 countries, accounting for more than 200,000 new cases yearly. These data indicate that M. leprae continues to be transmitted among low-income populations, particularly in India, Brazil, and Indonesia which currently account for 74% of new cases of leprosy worldwide. 6 The World Health Organization, WHO Global Leprosy Strategy 2021-230 “Towards Zero Leprosy” aims “zero infection and disease, zero disability, zero stigma and discrimination.”7–9
Despite research efforts, leprosy diagnosis remains based on clinical signs and symptoms requiring the identification of skin lesion(s) with partial or total loss of thermal, painful, and/or tactile sensitivity, with or without thickened nerves; microscopic identification of M. leprae in an intradermal smear is considered a confirmatory test; however, a negative result does not exclude leprosy diagnosis. 10 The clinical diagnosis of leprosy requires experienced health-care professionals to differentiate it from other confounding skin diseases. 11 Moreover, during the chronic course of the disease, clinicians should be able to identify subtle acute immune-inflammatory symptoms associated with leprosy reactions (mainly Type 1 or Reversal Reaction and Type 2 or Erythema Nodosum Leprosum/ENL) that may appear before, during, or years after specific MDT. Leprosy reactions require prompt diagnosis and treatment to avoid irreversible nerve damage and incapacities. 12
Leprosy represents a spectral disease including a wide range of clinical, bacteriological, immunological, and dermato-pathological characteristics which depend on the profile of immune responses of the host to the bacilli. In one pole of the disease, patients with inflammatory Th1-type and Th17-type cellular immune responses can activate macrophages to destroy harboring bacilli.5,13 As a consequence of the effective leprosy-specific cell-mediated immunity (CMI), these patients have low bacillary load, weak humoral immune responses, and are known as paucibacillary (PB) leprosy. 14 On the other extreme of the spectrum, patients with prevailing activation of Th2-type and T regulatory cells are unable to activate leprosy-specific CMI but induce strong humoral immunity with robust production of specific antibodies that, however, are not able to destroy intracellular pathogens. As a consequence of the leprosy-specific T-cell anergy, skin macrophages are full of bacilli that multiply freely leading to multibacillary (MB) disease. 12 Patients with intermediary clinical forms between the extremes present a mixed immune profile of the polar forms. 5
The classification of leprosy cases has been an area of debate and the Ridley and Jopling (R&J) classification based on clinic, histopathologic, microbiologic, and immunologic features comprises tuberculoid (TT), borderline tuberculoid (BT), borderline-borderline (BB), borderline lepromatous (BL), and lepromatous leprosy (LL); the early presentation was referred to as indeterminate form (I). 15 MDT for leprosy consists of three-drug regimen with rifampicin, dapsone, and clofazimine for all leprosy patients, for 6 months period for PB and 12 months for MB leprosy. 9 Due to difficulties in performing adjunct exams, histopathology and bacilloscopy, in endemic countries, the WHO proposed a simple operational method of counting skin lesions to determine treatment as PB or MB leprosy: PB leprosy, ⩽5 lesions and absence of bacilli in a slit-skin smear; MB leprosy, >5 lesions or with nerve involvement (pure neuritis, any number of skin lesions and neuritis) or presence of bacilli in slit-skin smear despite the number of skin lesions. 16
Currently, there is no gold standard test for the laboratory diagnosis of all forms of leprosy or for the diagnosis of early asymptomatic cases or for the prediction of the risk of disease progression in exposed individuals. Therefore, leprosy diagnosis remains based on clinical manifestations and the lack of clinical expertise and of adjunct tests contributes to delayed diagnosis, misdiagnosis, and mistreatment that decisively favor the ongoing transmission of M. leprae. 16
Highly sensitive and specific molecular tests such as the quantitative polymerase chain reaction (qPCR) (real-time PCR) have been indicated as auxiliary diagnostic test for leprosy and for the surveillance of drug resistance. 9 More recently, the molecular technique known as loop-mediated isothermal amplification (LAMP) has been proposed for the specific and sensitive detection of M. leprae DNA; however, its use is still restricted to research purposes.17–19 Both qPCR and LAMP require costly laboratory procedures, reasonable infrastructure, and specialized technical expertise.20,21
Point-of-care tests (POCTs) that can be provided near or at the place of patient care can contribute to appropriate diagnosis, representing ideal diagnostic tests for tropical diseases that need to be affordable, sensitive, specific, field and user-friendly, rapid, equipment-free, and easily delivered. 22 As leprosy-endemic areas are mostly located in low-resource settings, field-friendly rapid tests are recommended. For leprosy control programs, the incorporation of POCTs, such as the lateral flow rapid test, in alignment with bacilloscopy and qPCR, has the potential to help the decentralization of leprosy diagnosis, early diagnosis before the appearance of disabilities, and contact tracing of newly diagnosed patients, potentially contributing to interrupt M. leprae transmission chain. 23 However, POCT is not recommended as a stand-alone diagnostic test, but as an adjunct for bacilloscopy and for the referral of suspected cases to a reference center. 24
This review summarizes the state of the art of serological tests to aid the diagnosis of leprosy, highlighting the enzyme-linked immunosorbent assay (ELISA) and POCT biotechnologies using the phenolic glycolipid-I (PGL-I) antigen and the impact of the postgenomic era on the production of new specific M. leprae antigens, such as the leprosy Infectious Disease Research Institute (IDRI) diagnostic-1 (LID-1). Other potential applications of serological tests are also presented. Finally, we briefly review the state of the art of molecular techniques for the detection of M. leprae DNA.
Bacilloscopy of intradermal scraping and histopathology of skin biopsy
Bacilloscopy involves microscopic examination of intradermal scraping from lesions, earlobes, and elbows, and its results are expressed by the bacilloscopic index (BI: a measure of the number of bacilli in the dermis expressed in a logarithmic scale). 25 Bacilloscopy can help diagnosis ascertainment and orient the operational classification of leprosy for PB and MB MDT, aid the differential diagnosis, and help diagnosis of suspected relapse cases.25,26 Histopathology of leprosy skin lesion biopsies requires experienced pathologist to identify granulomatous inflammatory involvement of the nerves, lympho-histiocytic or granulomatous infiltrates in mature or immature epithelioid presentations, and the Fite-Faraco (FF) staining can identify bacilli; however, they are rarely seen in PB patients.27–29 For both bacilloscopy and histopathology, collection of specimens is invasive, readings and the interpretation of slides are subjective, 30 and the training and maintenance of skilled professionals to perform these exams require quality-control monitoring.27,29 In this sense, user and field-friendly POCTs, as serologic and molecular tests represent valid alternatives to aid the clinical diagnosis of leprosy in endemic countries.
Serological diagnosis of leprosy: the state of the art
PGL-I serology: applications and limitations
Compared to bacilloscopy, histopathology, and molecular assays, serological methods are cheaper and easier to perform, representing a suitable choice for the auxiliary diagnosis of suspected cases of leprosy. 20 The PGL-I antigen, the major surface antigen specific of M. leprae, is composed by carbohydrates and lipids and induces the production of mainly IgM antibodies, besides a smaller proportion of IgG and IgA antibodies.31–33 The PGL-I antigen is highly stable when stored at room temperature. 34 The PGL-I comprises three carbohydrates: 3-O-methyl-rhamnose, 2,3-di-O-methyl-rhamnose, and 3,6-di-O-methyl-glucose which are glycosidically linked to a phenol group with a phthiocerol portion with mycocerosic acids. 31 Its immunologic epitopes are found in the trisaccharide portion of the molecule, mainly the terminal disaccharide which provides the specificity of the PGL-I antigen.31,34 M. leprae has never been grown in axenic cultures, and the extraction and purification of the native PGL-I from bacilli obtained from human skin lesions, and armadillo tissues or infected mouse footpads are laborious as it has low solubility in aqueous solutions. 31 New PGL-I analogs were engineered by coupling chemically synthesized di- or trisaccharide haptens to hydrophilic carriers, such as bovine serum albumin (BSA) or human serum albumin (HSA), which improved its water-solubility while maintaining its specificity31,35 and allowed antigen binding to polystyrene ELISA plates and to nitrocellulose membranes for lateral flow immunochromatographic assays.36–38
The major difference of most PGL-I synthetic glycoconjugates is the nature of the linker arm between the hapten and the carrier protein. The first chemically synthesized PGL-I antigen used in serological studies was the NDO-BSA (natural disaccharide-octyl-BSA) 31 followed by the NTO-BSA (natural trisaccharide-octyl-BSA) 32 and by the NTP-BSA (natural trisaccharide-phenylpropionyl-BSA). 35
PGL-I serology, especially employing its semi-synthetic di- and trisaccharide analogs NDO and NTP, respectively, represents the most investigated and the best standardized serologic test to detect specific antibodies to M. leprae. PGL-I serology mainly based on ELISA to detect IgM antibodies has been evaluated in several endemic countries throughout the world.23,39,40 In general, these studies showed that anti-PGL-I positivity reflects the bacillary load: most MB patients are seropositive, while the majority of PB patients are seronegative.38,41 Despite the limited application of anti-PGL-I serology for the diagnosis of all clinical forms of leprosy, it has been considered as an important adjunct tool for the operational classification of PB and MB leprosy.42,43
Studies from endemic countries have indicated that PGL-I serology can be a useful tool to monitor individuals at higher risk of developing leprosy such as household contacts, contributing to early diagnosis. Anti-PGL-I IgM antibodies are considered reliable markers of exposure to M. leprae, not necessarily infection or disease. Among household contacts, especially of MB index cases, PGL-I positivity is a known marker of higher risk to develop leprosy. A surveillance study among contacts that included PGL-I NDO ELISA showed that the seropositivity rate was significantly higher among those contacts living in the households where new cases emerged (34.8%) than among the contacts living in households where no new cases were detected (14.3%; P < 0.001). 44 However, a recent meta-analysis showed that among PGL-I seropositive contacts, more than half did not progress to disease manifestations. 45
The postgenomic era: the characterization of new M. leprae recombinant antigens and the discovery of new biomarkers for leprosy immunodiagnosis
Before the completion of the full sequence of the M. leprae genome in 2001, 46 the discovery of new diagnostic M. leprae antigens was hampered by the limited availability of source of antigens. In the postgenomic era, significant advances in bioinformatics, encompassing multiomics (genomics, proteomics, transcriptomics, metabolomics, lipidomics, etc.), allowed the identification of new M. leprae genes and proteins, carbohydrates, lipids, and revealed unique pathways of host–pathogen interactions. 47
For the diagnostic field, the postgenomic era was characterized by the description of several recombinantly expressed M. leprae protein antigens and synthetic peptides that were evaluated regarding their diagnostic potential for both T-cell assays and serology. 48 Among several recombinant M. leprae protein antigens screened, two highly immunogenic proteins, ML0405 and ML2331, were described to be recognized by IgG from LL and BL patients. These two antigens were fused into an antigen named LID-1 that has been tested in serologic studies from different endemic areas such as the Philippines, and coastal and central Brazil.49,50 The screening of the immunogenic potential for T-cell assays and serology of 36 new M. leprae recombinant proteins highlighted three proteins (ML0405, ML2055, and ML2331) that elicited both leprosy-specific CMI and humoral response, suggesting their potential use in the development of CMI tests and new serological tests. 51 During this period, studies searched for new protein antigens that could eventually be recognized with higher sensitivity by IgG from PB patients. However, as the list of new recombinant protein antigens screened for serology increased, it became clear that in leprosy patients, the profile of antibodies elicited by newly described M. leprae proteins reflected the pattern of response already described to PGL-I antigen: robust antibody production in MB patients and weak/moderate response in PB patients. The immunodiagnosis of PB leprosy patients requires markers associated with CMI; however, the ideal biomarker or combination of biomarkers for PB leprosy has not been identified.51,52 Extensive field evaluations of new M. leprae protein antigens in endemic and non-endemic regions have been important to validate their diagnostic potential to identify subclinical or early infections and their prognostic value in various endemic settings.
Following the PGL-I, the LID-1 chimeric fusion protein antigen represents the second most widely evaluated antigen for leprosy serology in endemic countries.53–55 Instead of searching for new antigens to replace the PGL-I, the current understanding has been to add new promising antigens to PGL-I aiming to improve its specificity, and especially its sensitivity. In this sense, the LID-1 antigen has been tested simultaneously or conjugated with PGL-I regarding its potential to improve leprosy serology. For this purpose, a new single fusion complex antigen, the NDO-LID was developed representing a conjugate of the natural PGL-I disaccharide-octyl and the LID-1 antigens. Considering the carbohydrate nature of the PGL-I epitope and the LID-1 protein, the use of the NDO-LID serology implies the detection of two antibody isotypes: IgM to NDO PGL-I and IgG to LID-1.54,56 A study for the detection of leprosy patients from Colombia showed that IgM detection to NDO-LID-1 showed greater sensitivity compared to the detection of IgM to PGL-I. 57 A surveillance study in a Brazilian endemic area including leprosy index cases and intradomiciliary and peridomiciliary contacts evaluated ELISA to NDO-BSA, LID-1, and ND-O-LID as adjunct diagnostic tools. Results showed higher seropositivity to LID-1, including among the incident leprosy cases. 53 In MB or PB leprosy patients from Yunnan, China, higher sensitivity was obtained by the use of ELISA NDO-LID compared to LID-1 and NDO-BSA. 55
A review and meta-analysis that compared the accuracy of leprosy ELISA tests with native PGL-I, NDO-BSA, and LID-1 showed that NDO-BSA serology was better regarding sensitivity, specificity, positive and negative predictive value, and diagnostic value especially among MB patients, while the use of LID-1 gave similar sensitivity (Table 1). 58 A systematic review on the sensitivity and specificity of serologic tests using M. leprae recombinant protein antigens for leprosy diagnosis showed that the NDO-LID antigen has been more accurate to identify new cases of leprosy in individuals from endemic and non-endemic areas and household contacts in Brazil, Colombia, and the Philippines, especially when combined with other biomarkers and confirmed that serology remained limited for the diagnosis for PB leprosy (Table 1). 59
Recent review articles on leprosy serology.
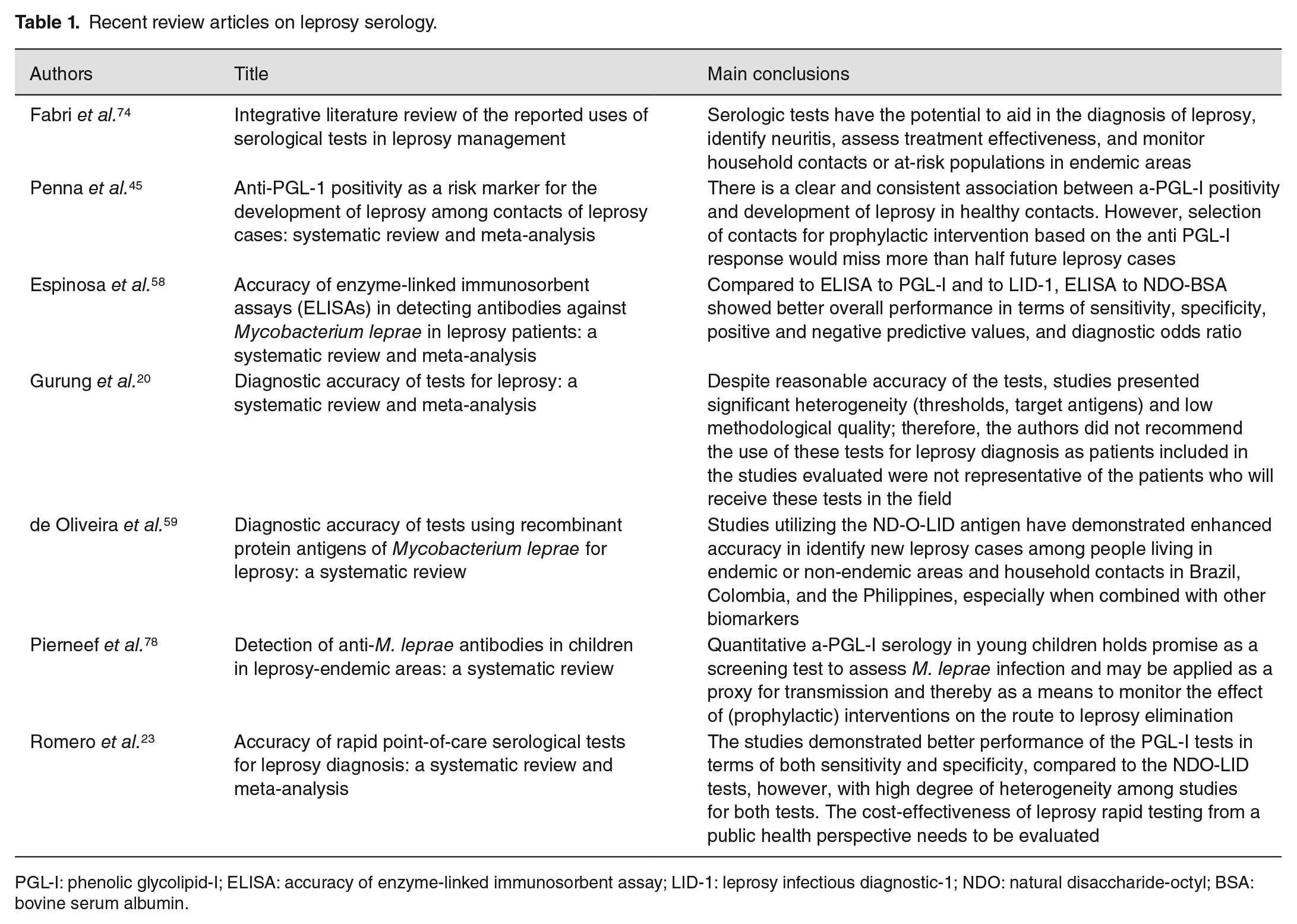
PGL-I: phenolic glycolipid-I; ELISA: accuracy of enzyme-linked immunosorbent assay; LID-1: leprosy infectious diagnostic-1; NDO: natural disaccharide-octyl; BSA: bovine serum albumin.
Besides IgM and IgG antibodies to M. leprae, studies have investigated the use of IgA serology to detect early disease or subclinical infection, however, with conflicting results.60,61 The potential advantages and disadvantages of incorporating the detection of IgA and IgG antibodies in the ML Flow have been previously discussed.62,63 Despite the unclear results about the advantage of the combined detection of IgG, IgM, and IgA antibodies, we cannot exclude the possibility that diagnostic kits capable of simultaneously detecting different isotypes to antigens based on PGL-I and LID-1 may provide better tools to identify contacts at greatest risk of becoming ill.
In the serodiagnosis of infectious diseases, especially using protein/peptide antigens, IgM production is always associated with the acute phase which is followed by isotype switch to permanent IgG production, in parallel with the decline of the IgM response throughout the chronic phase. Regarding antibody production to PGL-I antigen, although IgG and IgA production also occurs, the predominant IgM response is continuous and should not be misinterpreted as acute phase, recent exposure, or recent infection by M. leprae. IgM isotype is the main antibody class induced by carbohydrate antigens that are considered T-independent antigens, as is the case of the di- or trisaccharide epitope of the PGL-I antigen, regardless of the duration of the disease, infection, or exposure to M. leprae.
POCTs for leprosy
POCTs, traditionally based on lateral flow immunochromatography, can orient referral to leprosy experts and contribute to early diagnosis which may help to interrupt M. leprae transmission. POCTs have been used to aid the diagnosis of leprosy using whole blood obtained by non-invasive finger stick, and the results can be evaluated with the naked eye after 10–15 min.38,64 The results of a simple dipstick assay developed for the detection of IgM to NDO-BSA using whole blood of patients from an endemic area in the Amazon, Brazil, showed high agreement with ELISA results. 64 Later, a POCT using the NTP-BSA named ML Flow was developed and showed high agreement with ELISA results with >97% sensitivity for MB patients, <50% for PB patients, and 90.2% specificity. 38 A Brazilian study showed that ML Flow test was useful as an additional classification tool for PB and MB leprosy, as it reduced the number of cases that would have been treated as MB disease. 65 Two different versions of the anti PGL-I rapid tests were tested in Brazil and Nepal: the ML ICA that used NDO-HSA or NDO-BSA to detect IgM, IgG, and IgA antibodies, produced in Korea and the ML Flow test to detect IgM to the NTP-BSA (Omega Teknika Limited, Dublin, Ireland; Royal Tropical Institute, KIT, Amsterdam, the Netherlands). The results showed different performance of the tests in each population: the ML Flow test was the best POCT for the operational classification of PB and MB leprosy in Nepal, while in Brazil, the ML ICA test yielded better performance. 66
Other versions of the lateral flow test using different antigens have been described. A test based on dual path platform (DPP) using the ML0405, ML2331 antigens, and the LID-1 fusion construct was useful to aid the diagnosis of MB leprosy. 67 The construct conjugate of the NDO-BSA and LID-1 antigens was proposed to provide early and accurate leprosy diagnosis. 68 A rapid test that used NDO-LID on nitrocellulose membranes allowed the rapid and simultaneous detection of specific IgM and IgG antibodies, and the results recorded by a cell phone–based test reader platform (Smart Reader) showed increased sensitivity for the identification of PB and MB patients when compared to ELISA results. 54
An investigation using patient samples from the Philippines compared two lateral flow diagnostic tests: the SD Leprosy test that detected IgM antibodies to NDO-BSA (Standard Diagnostics, Yongin, South Korea) and NDO-LID test that detected IgM antibodies to NDO PGL-I and IgG antibodies to LID-1 (Orange Life, Rio de Janeiro, Brazil). Smart reader results showed that NDO-LID test provided objective, consistent results with improved sensitivity and specificity compared to the SD Leprosy test. 69 An screening study using ELISA NDO-BSA IgM and LID-1 IgG, the rapid test NDO-LID (RDT NDO-LID, Orange Life, Rio de Janeiro, Brazil) and clinical examination by a dermatologist showed low specificity and sensitivity of serology and therefore did not recommend these tests as stand-alone diagnostic tools. 70 A study compared two leprosy rapid tests: immunochromatographic visual immunogold OnSite Leprosy Ab Rapid test (Gold-LFA, CTK Biotech, San Diego, CA, USA) that detects IgM antibodies to NDO-HSA and IgG antibodies to LID-1 and the quantitative, luminescent up-converting phosphor test that detects IgM to NDO-HSA (UCP-LFA, Leiden University, Leiden, The Netherlands). 71 The performance of these tests assessed in independent cohorts from the Philippines (high BI MB patients), Bangladesh (low BI MB patients), and Brazil (school children) showed that both rapid tests corresponded well with BI, but the UCP-LFA showed higher sensitivity.
Two rapid tests (ML Flow for IgM to NTP-BSA and NDO-LID for IgM and IgG, Orange Life, Rio de Janeiro, Brazil) used for the distinction of leprosy cases from healthy individuals in the highly endemic Brazilian Amazon region 72 showed limited positive predictive value (<50%), but high negative predictive value, especially the ML Flow test (94.6%). This feature is important to exclude leprosy diagnosis and to help discriminate leprosy from other confounding skin conditions that are prevalent in the region.
Currently, the commercial production of leprosy ELISA and rapid tests described in previous studies seems to be discontinued. In addition, although the smart reader technology, or other portable digital readers, has not been consolidated in leprosy rapid tests, previous studies have shown that smart reader could improve POCT by providing more consistent results eliminating bias of subjective visual readings and interpretations, that require training and can be affected by several variables. The availability of the cell phone smart reader objective readings for leprosy POCT in the field could also allow the prompt transmission to a cloud of digital data and other related information, such as socio-demographic data. This would allow data to be readily downloaded at referral centers for record saving and epidemiologic analysis, and these data could also be transferred to off-site specialists for a rapid second opinion.
A recent systematic review and meta-analysis on rapid point-of-care serological tests for leprosy diagnosis reported that although the accuracy results were not conclusive, they showed that PGL-I tests performed better than the NDO-LID tests, both in terms of sensitivity and specificity; however, a high degree of heterogeneity was observed in studies for both tests (Table 1). 23
The Leprosy POCT ML Flow test has been recently approved by the Brazilian Public Health System (SUS) and by the Leprosy Control Program to be used only for contact surveillance and is currently being implemented throughout the country; however, the impact of this intervention in leprosy transmission requires time and evaluation. 73 This decision has been followed by academic technology transfer of ML Flow production protocols (SBS, UFG, Brazil) to a private industry (Bioclin, MG, Brazil) assuring large-scale, quality-controlled production of tests for public health use.
Other potential applications of serology for leprosy management
A review on the use of serological tests for leprosy management that included detection of neuritis, monitoring MDT efficacy, and monitoring household contacts or at-risk populations in endemic areas concluded that serological tests can contribute substantially to leprosy management (Table 1). 74 As serology reflects the bacillary load, studies investigated its usefulness to monitor the efficacy of MDT and as recurrence prognostic marker.75,76 A robust study in MB patients (3400 samples from 263 MB patients) described that MDT regimens (6 doses Unified-MDT/CT-BR and the Regular 12 doses-WHO MDT) lead to slow and gradual decrease of antibodies to PGL-I, NTP-BSA, LID-1, and NDO-LID in MB patients. 77
Another possible use of leprosy serology is to identify recent infection and transmission especially in young children as leprosy diagnosis among them indicates continuous and recent M. leprae transmission. As leprosy seropositivity in children is inversely correlated with age, children represent a suitable group for the sensitive evaluation of recent M. leprae infection. A systematic review on children (<15 years) without leprosy included serologic studies to different PGL-I antigens, detected by quantitative ELISA or UCP-LFA or by the qualitative rapid tests ML Dipstick, ML Flow, or NDO-LID (Table 1). 78 Analyses showed a high seroprevalence (14.9%) that declined with age. Despite the use of different antigens, methodologies, sample sizes, and variable cut-offs, analyses indicated that quantitative anti-PGL-I serology in young children seems a potential tool to assess recent M. leprae infection and can be used as a proxy for transmission orienting further postexposure prophylactic interventions to interrupt transmission.
The use of leprosy serology as a predictor of leprosy reactions has been also considered, 79 and in MB patients, higher susceptibility to develop ENL was reported in patients with persistent serum antibodies to LID-1. 80 ML Flow test baseline results in a cohort of patients enrolled in Brazilian endemic areas showed limited sensitivity and specificity to predict the development of leprosy reactions both Reversal Reaction and ENL. 40 Antibody responses to PGL-I, LID-1, and ND-O-LID evaluated at baseline by ELISA in reaction-free leprosy patients and enrolled and monitored for the development of leprosy reactions showed low sensitivity and specificity for Reversal Reaction prediction; however, anti-LID-1 serology at diagnosis showed prognostic value for ENL development in BI positive patients. 40 Analysis of anti NDO-BSA ELISA and the NDO-LID® rapid test in Brazilian reactional and reaction-free patients at diagnosis and for patients who developed ENL after diagnosis showed higher positivity rates for both tests in reactional patients. 81
Leprosy serology (ELISA anti-NTP-BSA PGL-I, anti-LID-1) was investigated as additional tool for the differential diagnosis in a highly endemic Brazilian area and indicated that LID-1 serology was useful to differentiate MB leprosy from other confounding dermatoses. 82 The use of leprosy serology for orienting surveillance and postexposure prophylaxis has also been examined. Leprosy contacts are at higher risk of manifesting leprosy and early diagnosis and treatment are key for control programs. Prophylaxis may include Bacillus Calmette–Guérin (BCG) vaccination or revaccination, and more recently, single dose of rifampicin chemoprophylaxis has been debated as an additional strategy to reduce transmission. 4 A systematic review and meta-analysis on PGL-I positivity among contacts and development of disease included cohort studies with at least 1-year follow-up, classification of healthy leprosy contacts based on anti-PGL-I positivity at baseline (different PGL-I antigens, ELISA, and ML Flow) and that considered the outcome as the clinical diagnosis of leprosy (Table 1). 45 This review confirmed the increased risk (three times) of anti PGL-I positive contacts to develop leprosy, but despite variations, the proportion of PGL-I positive leprosy cases at baseline was always under 50%. Therefore, the selection of contacts for chemoprophylaxis based on PGL-I positivity only, would miss more than half future leprosy cases, indicating that the incorporation of PGL-I serology into leprosy control programs to orient chemoprophylaxis requires confirmation. A systematic review and meta-analysis on the diagnostic accuracy of tests, both serologic and molecular for leprosy, concluded that despite reasonable accuracy of the tests evaluated, studies presented significant heterogeneity (thresholds, target antigens) and low methodological quality (Table 1). 20
In summary, the list of possible applications of leprosy serology goes beyond aiding diagnosis of new cases as it spans on monitoring MDT efficacy, for the differential diagnosis with other skin diseases, as a predictor of leprosy type 2 reactions, a biomarker of recent transmission in children and a surrogate marker of disease progression to orient chemoprophylaxis interventions in adults.
Molecular diagnosis of leprosy: state of the art
Several studies have shown that the detection of M. leprae DNA by polymerase chain reaction (PCR) can also contribute to the diagnosis of leprosy (Table 2). The sequencing of the pathogen genome enabled the selection of gene sequences that can be amplified with high specificity from a few M. leprae cells. 83 In PB patients, their low bacillary load compromises the sensitivity of the molecular diagnosis of leprosy, 20 but developments in molecular techniques have improved the sensitivity of the test in the identification of bacilli in subclinical infections and in PB patients. 84 However, the early diagnosis of leprosy by PCR in skin biopsy samples from patients in the TT pole or PB remains a challenge.
Recent molecular techniques for the detection of M. leprae DNA.
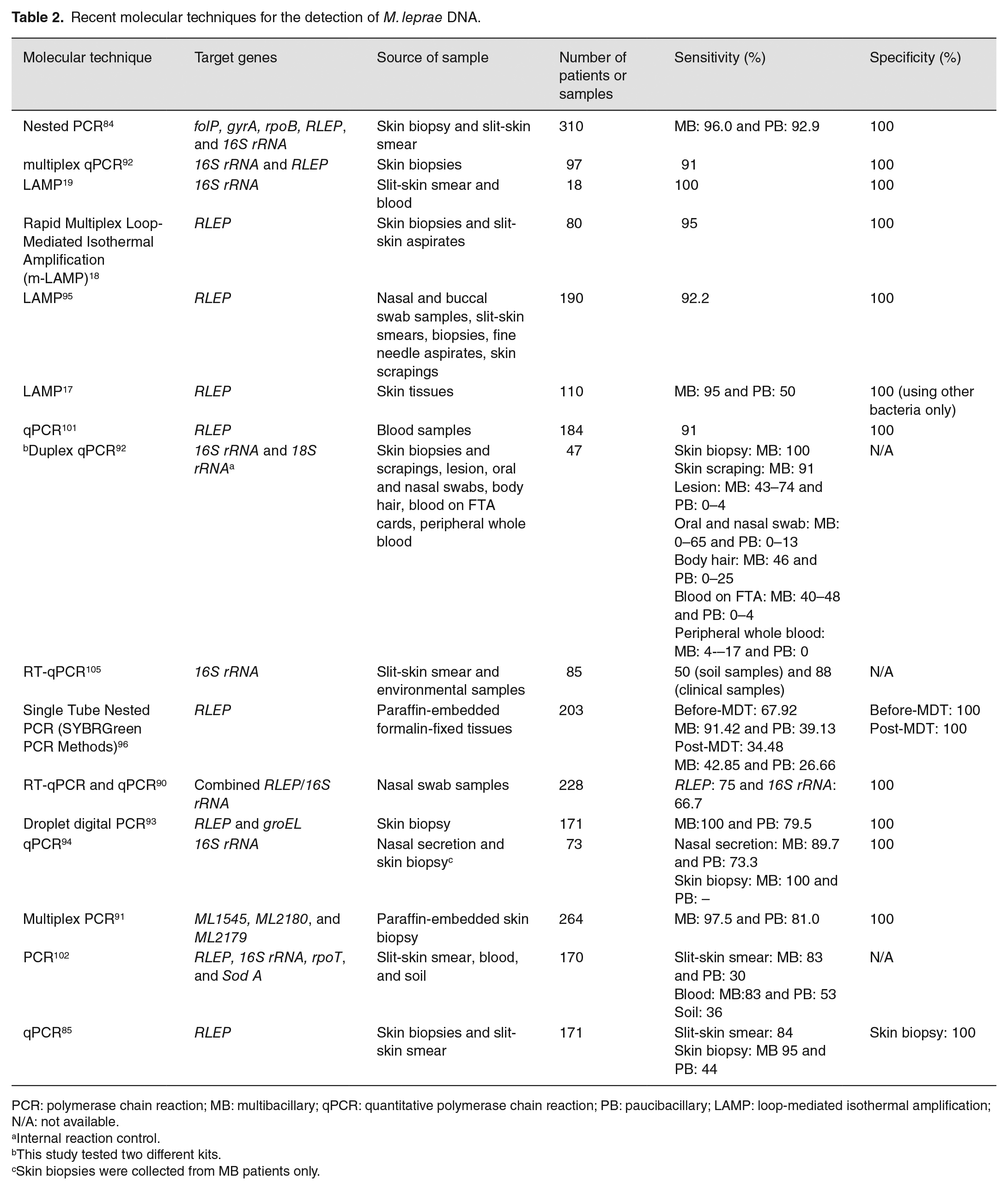
PCR: polymerase chain reaction; MB: multibacillary; qPCR: quantitative polymerase chain reaction; PB: paucibacillary; LAMP: loop-mediated isothermal amplification; N/A: not available.
Internal reaction control.
This study tested two different kits.
Skin biopsies were collected from MB patients only.
Conventional PCR has been replaced by qPCR which is faster, more sensitive and specific. 85 The qPCR qualitatively detects specific gene sequences of M. leprae, including among others, the repetitive sequences (RLEP), the Ag85B, and the gene encoding the 16S subunit of ribosomal RNA (rRNA) in samples of skin or nerve biopsies. 84 The M. leprae-specific repetitive element (RLEP) is a multicopy repeat sequence widely used as a target for the molecular diagnosis of leprosy. There are approximately 37 copies of RLEP on the M. leprae genome,83,86 and studies suggest 100% specificity of the RLEP qPCR for detecting M. leprae, making this target sequence the gold standard.19,87,88 However, the possible existence of homologous RLEP sequences in other yet unidentified, non-culturable mycobacteria may pose future challenges for the specificity of the assay. 89 RLEP sequence amplification by in-house qPCR in skin biopsies from patients with all clinical forms and reactional stages showed 84.92% sensitivity and the concordance between qPCR and BI was 87.30%. 85 In slit-skin smear, an alternative biologic specimen for the molecular detection of M. leprae, the sensitivity was 84.0% and the specificity was 100%. 85 Besides RLEP and 16S rRNA, 90 other target sequences described in the literature are the folP, gyrA, and rpoB genes, which are also used to identify drug resistant M. leprae. 84 The most recent studies in the molecular diagnosis of leprosy based on PCR variations are summarized in Table 2. The qPCR, 85 nested PCR 84 and variations such as multiplex,87,91 duplex, 92 and droplet digital (ddPCR) 93 have been reported for different M. leprae target sequences, with RLEP and 16S rRNA representing the most used ones.94–96 A study showed that multiplex PCR helps detect early leprosy cases and household contact surveillance for leprosy. 97
Nested PCR is useful for amplifying genes from samples with low bacillary load in PB patients, as this technique amplifies sequences within the amplicon generated in the first amplification round. 84 The use of two target genes in ddPCR (RLEP and groEL) considerably increased the sensitivity to detect M. leprae DNA in PB patients compared to qPCR (79.5% vs 36.4%). The specificity was 100% in both ddPCR and qPCR. 93 Approaches for the detection of multiple genes using pools of primers that are easily designed and synthesized increase the chance of identifying bacterial DNA and enhance the possibility of M. leprae DNA detection in samples from PB patients; however, these techniques require reasonable laboratory infrastructure and expertise.
The use of a qPCR kit for M. leprae has been recently approved in 2021 by the Brazilian Public Health System and by the Leprosy Control Program exclusively for the investigation of potential new cases among contacts of confirmed cases of leprosy. 73 This product called “IBMP Biomol Leprosy Kit” approved to aid leprosy diagnosis, reported 91% sensitivity and 100% specificity and uses target genes and their respective reporter labels 16S rRNA-FAM, RLEP-VIC, and 18S rRNA-Cy5 (internal control). 98
Success has been reported in the use of formalin-fixed, paraffin-embedded skin biopsy specimens for genomic DNA extraction and subsequent amplification of the M. leprae RLEP–based sequences. 96 Peripheral whole blood tested by M. leprae ML0024 qPCR in untreated leprosy patients and household contacts followed up for 7 years showed that contacts with positive PCR in blood at diagnosis of index cases are at higher risk of later leprosy onset. 99 However, other studies show that blood may not be a suitable specimen to detect M. leprae DNA in MB and PB patients90,99,100 in contrast with studies that succeeded detecting M. leprae in whole blood.19,101,102 Further studies are needed to evaluate the potential use of peripheral whole blood for the early molecular diagnosis of leprosy and to evaluate the relationship between blood bacillary load and the development of leprosy in contacts.
Saliva and nasopharyngeal swab sample collection is considered non-invasive, and studies about the use of these specimens for the molecular diagnosis are encouraged as their results may help the understanding of the airborne transmission of M. leprae. A study on M. leprae qPCR using nasal swabs from MB patients found that sensitivity for RLEP gene was 75% and 66.7% for the 16S rRNA gene while specificity was 100%. 90 M. leprae qPCR for the RLEP and the 85B genes using the hard palate mucosa scraping and nasal swab specimens from untreated leprosy patients and contacts reported similar sensitivity for both targets in both groups, indicating that buccal and nasal mucosa may be important sites of primary infection. 103 Results from a recent study showed a strong correlation of anti-PGL-I IgM levels in fingerstick blood and RLEP-qPCR positivity of nasal swabs. 104 In addition, DNA detection from saliva, nasal swab, and whole blood samples has the potential use for the early diagnosis and contact monitoring, as bacilli tend to be found in these sites during the incubation period. 92 However, it remains difficult to distinguish early infection in asymptomatic individuals, from healthy carriers.
Considering that the soil can be a reservoir of viable M. leprae cells, studies have investigated the presence of M. leprae DNA in environmental samples as this issue may potentially interfere with transmission. A qPCR investigation for RLEP, rpoT, SodA, and 16S rRNA genes in slit-skin smears, in blood of leprosy patients, and soil samples of patients and their surroundings reported that positivity for RLEP gene target was the highest in all the clinical (83%) and environmental samples (36%). The RLEP gene target was able to detect 53% of blood samples in BI-negative leprosy cases. 102 Another recent study using RLEP and 16S rRNA genes found 53% sensitivity in soil samples. 105 As these environmental investigations were carried out with small sample sizes, further studies should include larger and also evaluate the viability of M. leprae obtained from soil and environmental samples.
Since the bacillary load decreases with treatment, the detection of M. leprae DNA can be useful for monitoring MDT. However, studies have shown that the bacillary load tends to remain stable or show a small decrease within 2 years after starting MDT. 77 Thus, molecular tests for this purpose must carefully calculate the cut-off point.
LAMP is considered a highly sensitive and specific technique,17,19,87 that amplifies the target sequence in an isothermal reaction, usually at 60–65°C, and does not require thermal cyclers, agarose gel electrophoresis, or sequencing techniques. Positivity is evaluated by colorimetric method and visualized with the naked eye. 106 These features of the LAMP assay are valuable for a POCT aiming the early diagnosis of leprosy in remote places with restricted laboratory infrastructure, as it is the reality of most endemic regions. A LAMP-based point-of-care RLEP detection of M. leprae with 100% sensitivity and 92–100% specificity was described using a fast and easy-to-use portable fluorimeter that provides results in 45 min. 95 The ready-to-use RLEP-LAMP format can be considered an ASSURED test (affordable, sensitive, specific, user-friendly, rapid, equipment-free, delivered) applicable at the primary health-care level that could facilitate the early detection of leprosy index cases without the need of a reference laboratory. 95 Despite several repeated sequences of RLEP in the genome of M. leprae, these small sequences make the design of the panel of primers difficult for the implementation of LAMP.
Molecular diagnosis can also be useful in the operational classification of the disease since the amount of M. leprae DNA detected correlates with the bacillary load. The detection limit of the RLEP LAMP was determined as approximately 30 bacilli per sample, indicating a three times higher sensitivity than microscopy (104 bacilli per gram of tissue). 95 These findings indicate that using this methodology, PB patients could be reclassified as MB, especially BT patients or with low bacillary burden (BI > 1). Therefore, under treatment of MB patients, misclassified as PB, would be avoided by this method. Recent studies that have combined clinical examination of skin and peripheral nerves and the use of different exams, such as bacilloscopy, serology, and molecular tests have emphasized the importance of clinical expertise and the potential to improve early diagnosis by incorporating serology and PCR.104,105
Final considerations
Strong evidence demonstrates the high sensitivity of leprosy-specific serology, especially anti-PGL-I to identify MB leprosy patients who are considered the main source of transmission, therefore justifying its use and application for leprosy control programs. Currently, the traditional, specific, and low sensitivity methods to detect M. leprae such as bacilloscopy of skin smears and the FF bacilli staining on skin biopsies have been compared to new and more sensitive molecular tools for M. leprae DNA detection as qPCR and LAMP employing different gene targets and diverse biologic specimens (skin biopsies, intradermal scrapings, whole peripheral blood, saliva, buccal and nasal swabs). The consolidated and consistent data on the application of leprosy serology for MB patients together with new and promising improvements in molecular tests assure their use as valuable tools for the early and accurate diagnosis and for postexposure interventions. Early diagnosis and treatment are key strategies to reduce disabilities and to interrupt M. leprae transmission contributing to leprosy control in endemic countries.
Footnotes
Authors’ contributions
LL-L, DPS, MBTF, SB-S, and MMAS contributed to the conception and design. LL-L, DPS, and MMAS contributed to the acquisition of data. LL-L and MMAS contributed to the drafting the manuscript. LL-L, MMAS, and SB-S contributed to the revising the manuscript critically. LL-L, DPS, MBTF, MMAS, and SB-S contributed to the approval of the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Student’s fellowships were granted by the Brazilian Coordination for the Improvement of Higher Education Personnel (CAPES grant no. 388 88887.608185/2021-00 2021-2025) and the National Council for Scientific and Technological Development (CNPq grant no. 164180/2021-4), the Alliances Program for Education and Training (Scholarships Brazil – PAEC OAS-GCUB). MMdAS is a research fellow from the Brazilian Research Council/CNPq (“Bolsista de Produtividade em Pesquisa, grant no. 311986-2019-6).The Laboratory of Development and Production of Rapid Tests is supported by the Secretariat of Health Surveillance and Environment of the Ministry of Health (SVSA/MS), process 25000198995201989 TED156/2019.