
Abstract
Rationale
Seizure medication must be taken regularly to be effective; seizures often result from missed doses. Numerous barriers can delay people with epilepsy (PWE) from obtaining medication on time.
Methods
Two surveys were designed, one for PWE and their caregivers and one for healthcare providers (HCPs). Surveys were delivered electronically and data analysis was descriptive.
Results
Medication unavailability was the most common barrier reported. Additional barriers in order of decreasing frequency included: the message “too soon to refill,” insurance coverage, prescription delay, and cost. For non-active drivers, transportation was a barrier. Sequelae of delayed medication access included: stress, emergency medication utilization, and hospitalization. Access to seizure medications was recognized as a problem by 95% of HCP surveyed, most frequently attributed to insurance barriers and cost. Over 10% of HCP reported a patient death from a medication access issue.
Conclusion
The American Epilepsy Society's Position Statement on medication access supports reducing obstacles that delay obtaining medication through a multifaceted approach. It recommends elimination of unnecessary regulatory barriers, cost containment and insurance reform, supply chain transparency, practice management guidance, and ongoing research.
Introduction
Epilepsy is a common, chronic health condition with significant morbidity and premature mortality that affects over 3.4 million people in the United States.1–3 Medication is the mainstay of treatment for epilepsy, providing seizure freedom in two-thirds of individuals when appropriate medications are taken as prescribed. 4 Antiseizure medication (ASM) is not curative but needs to be taken consistently to maintain efficacy. 5 A single missed or delayed dose can result in a breakthrough seizure, with immediate consequences including reduced quality of life, injury, loss of driving privileges, missed school and work, and even death. 6
Medication nonadherence is a common challenge in epilepsy management,5,7,8 with reported rates from 18 to 79%.8,9 Nonadherence results in increased healthcare utilization and costs, and increased mortality.10,11 Adherence to ASMs is multifactorial, including access to care as well as intending to and remembering to take medication. No adherence strategy can succeed if the medication itself is unavailable when needed. Several factors make obtaining medications challenging for people with epilepsy (PWE). PWE are more likely to lack transportation, use public health insurance, and have difficulty affording medication.3,12 Additionally, many ASMs are controlled substances, requiring more frequent prescriptions due to restrictions on refills and days supplied. These requirements create narrow windows for requesting and picking up medications. 13 These challenges are compounded by availability delays: supply chain issues, pharmacy refill restrictions, and stocking practices. 14
The American Epilepsy Society (AES) Treatments Committee Medication Access Workgroup was established in 2023 in response to the recognition of these challenges. Literature review revealed need for more information on causes and consequences to identify priorities for systemic improvement. Two online surveys captured perspectives from, 1) PWE/caregivers and 2) healthcare providers (HCPs).
Methods
Survey questions were developed using input from HCPs and caregivers, targeted literature review, and prior related studies. PWE, caregivers, and HCPs evaluated the surveys for face and content validity. The study protocol was approved by the Albany Medical College IRB. No incentives were offered.
Voluntary participation was solicited electronically from PWE and caregivers via epilepsy advocacy organizations and from HCPs via professional society listservs and online communities. Surveys are provided in Appendix A. All survey items were optional due to the potentially sensitive nature of responses.
Data was collected from September 27, 2024, through January 15, 2025, using REDCap hosted at Albany Medical College.15,16 Data analysis was qualitative. Free-text responses were independently coded by reviewers, with discrepancies resolved by consensus or adjudicated by a third reviewer when needed. Additional information is available in Table 1.
Survey Design Methodology and Participation.
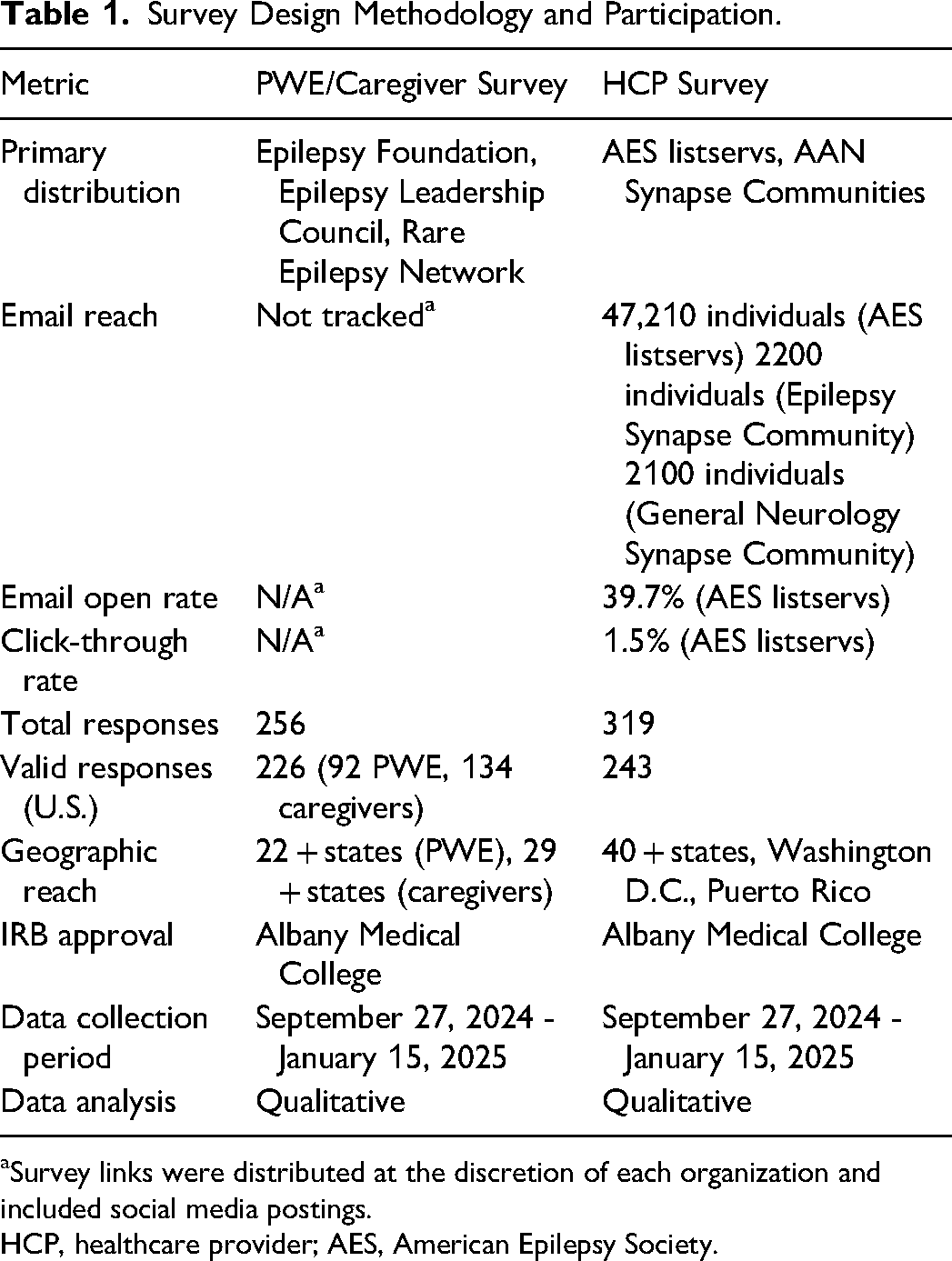
aSurvey links were distributed at the discretion of each organization and included social media postings.
HCP, healthcare provider; AES, American Epilepsy Society.
People With Epilepsy / Caregiver Survey Results
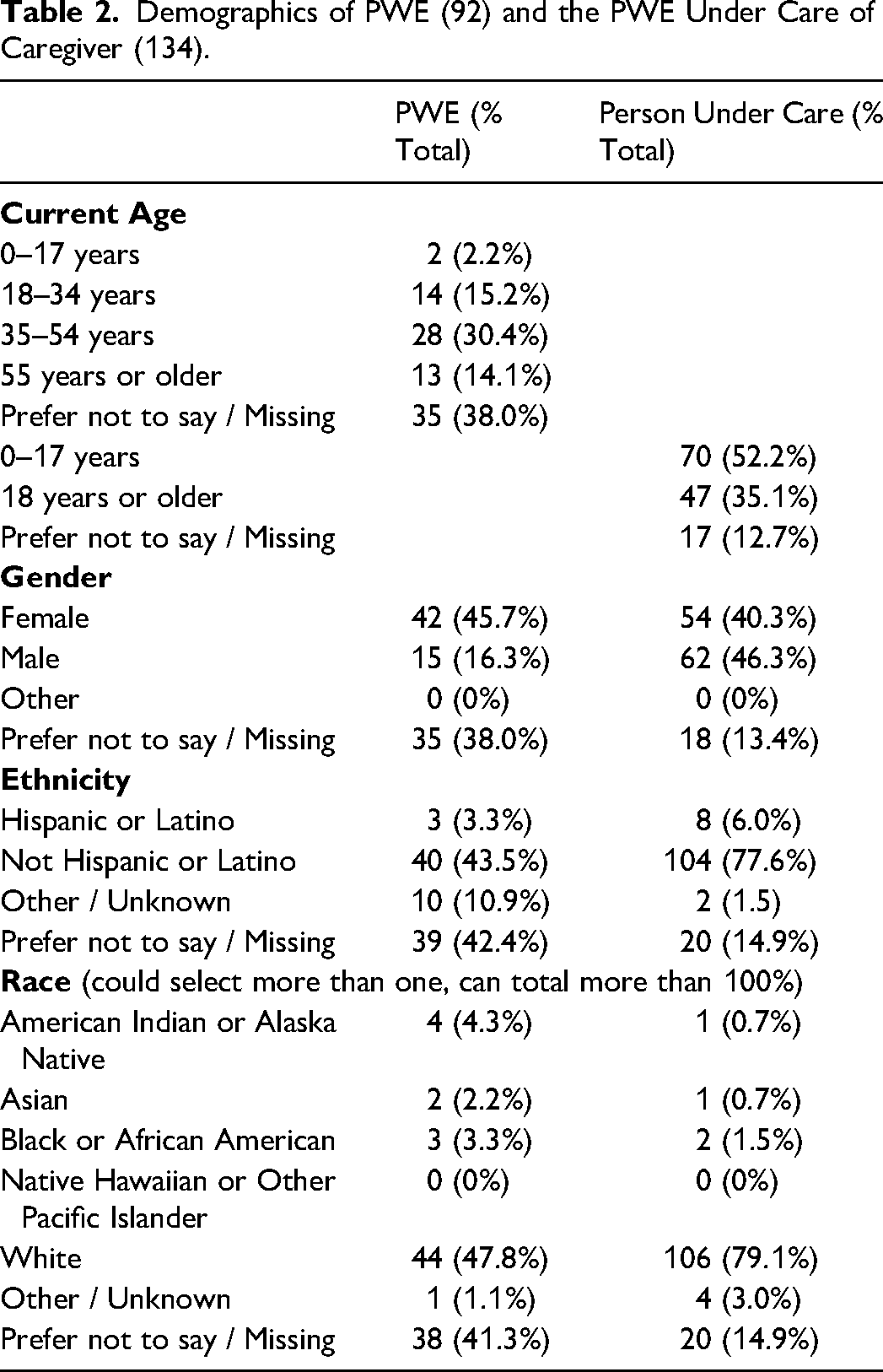
There were 256 respondents to the PWE/caregiver survey. Four did not identify either as a PWE or caregiver, and 29 never used seizure medication; both were excluded. Three PWE also identified as caregivers. The final analytic sample included 92 PWE and 134 caregivers. Respondent demographic and epilepsy characteristics are shown in Tables 2 and 3. Available zip code data indicated representation from at least 22 and 29 U.S. states among PWE and caregivers, respectively. Reported difficulties, management strategies, and consequences of missed dose(s) are shown in Figure 1. Free-text responses are summarized in Supplementary Table S1. Of the 92 respondents who had used ASMs, 60 (65.2%) reported having trouble filling or refilling a prescription; 21 (22.8%) reported no difficulty, and 11 (12.0%) did not respond. The most common difficulty was being told it was “too soon to refill,” despite need (34, 37%). The second most common difficulty was “medication not available” when needed (23, 25%), followed by insurance coverage (21, 22.8%). Overall, 15 respondents (16.3%) listed transportation as a barrier. Among respondents who were not active drivers 33% (9/27) cited transportation as a barrier, compared with 7.1% (2/28) of active drivers.
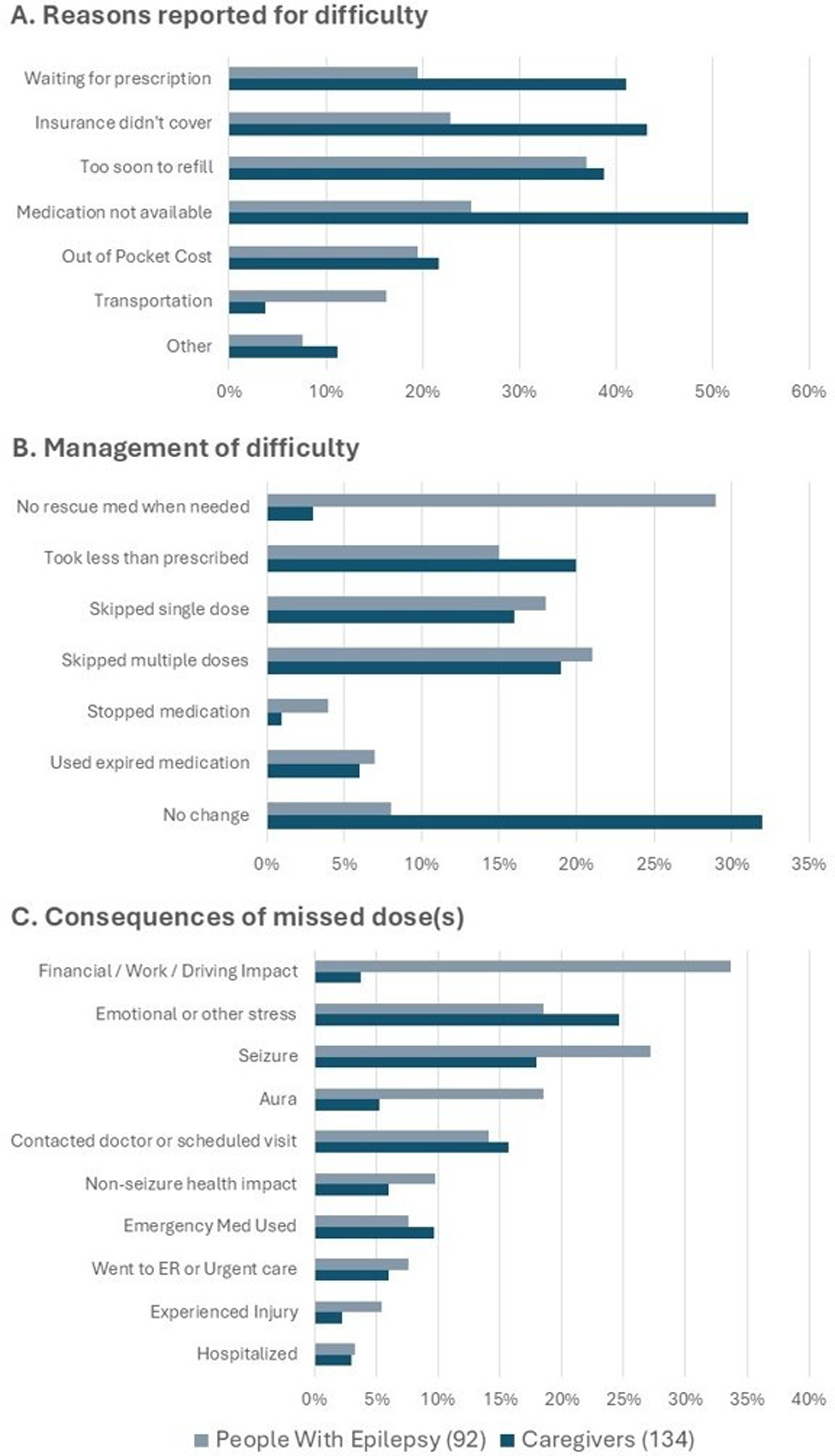
PWE and Caregiver Responses on Medication Access 190 × 355 mm (96 × 96 DPI).
Demographics of PWE (92) and the PWE Under Care of Caregiver (134).
Descriptors of PWE (92) and the PWE Under Care of Caregivers (134).
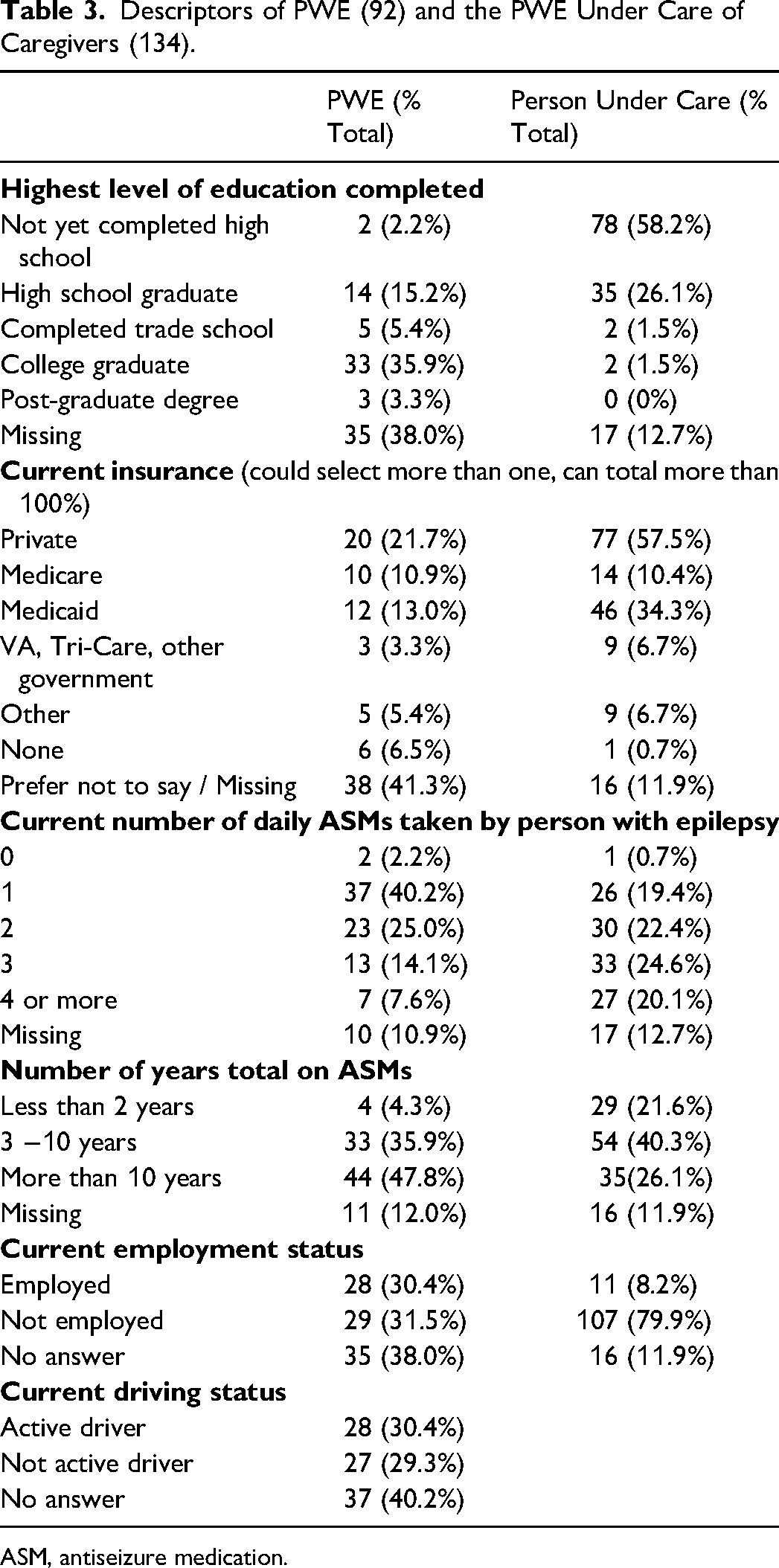
ASM, antiseizure medication.
As a result of difficulties obtaining medication, 27 respondents (29.3%) reported not obtaining rescue medication when needed, and 19 (20.7%) indicated skipping multiple doses. Reported consequences included financial impact (31, 33.7%) and breakthrough seizures (25, 27.2%). 17 Of the 134 caregivers who provided ASMs to PWE, 97 (72.4%) reported having difficulty obtaining medication at least once. The most common reason was medication unavailability (72, 53.7%), although other reasons were also frequently reported. Despite these challenges, 43 caregivers (32.1%) reported making no change. Reported consequences included stress (33, 24.6%) and seizures (24, 17.9%).
Healthcare Provider Survey Results
There were 319 unique responses in the HCP survey; three respondents were not HCPs and were excluded. Of the remaining respondents, 10 were located outside the U.S.; 17 provided invalid zip codes, and 46 did not provide zip codes. Only the 243 responses with valid US zip codes were included in the analysis, which showed representation from at least 40 U.S. states as well as Washington D.C. and Puerto Rico.
Respondents identified as epileptologists (149, 61.3%), neurologists (33, 13.6%), nurse practitioners or physician assistants (36,14.8%), or “other” (25, 10.3%), with further descriptors provided in Table 4.
HCP Characteristics (243).
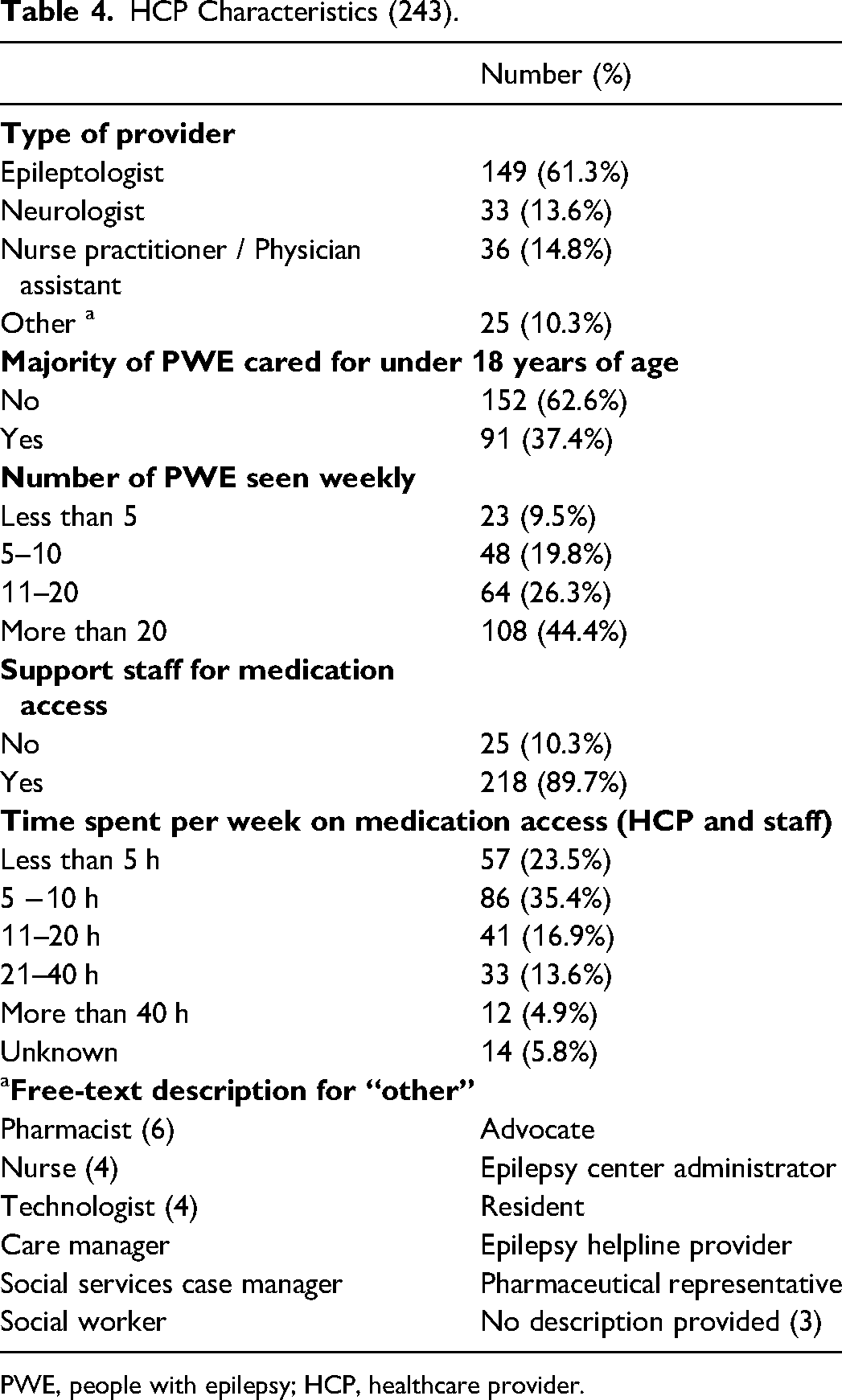
PWE, people with epilepsy; HCP, healthcare provider.
Figure 2 summarizes HCP perceptions of factors affecting care for PWE. 32 free-text responses were submitted under “other” causes of seizure medication access issues. Controlled substance regulations (11) were the most frequently cited issue, followed by limited ASM stock (7). Detailed data are provided in Supplementary Figure S2.
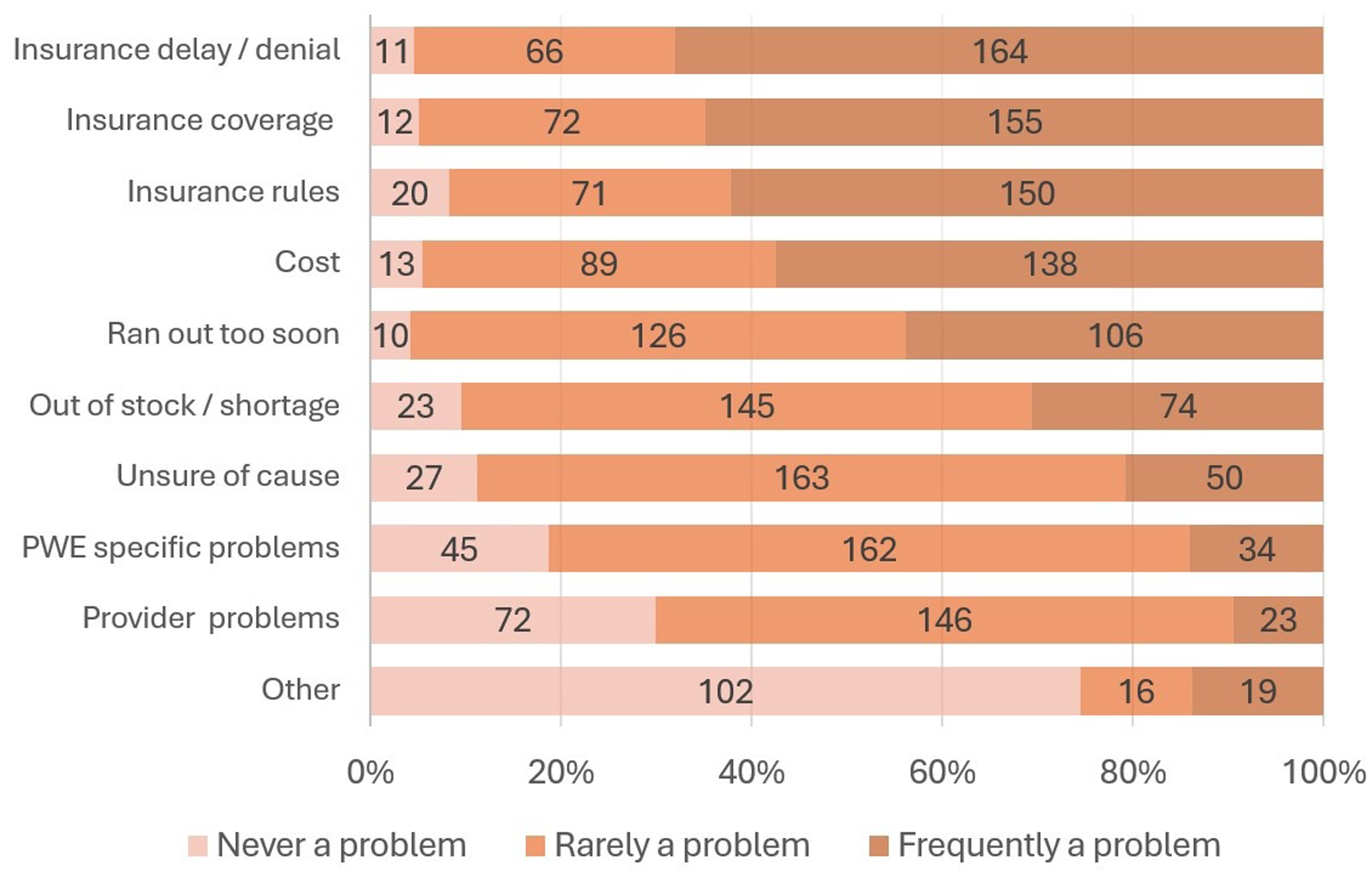
HCP Frequency of Access Concerns 228 × 165 mm (96 × 96 DPI). HCP, healthcare provider.
Overall, 231 HCP (95.1%) reported that access to ASMs was a problem, with 155 (63.8%) identifying it as a major concern. Additionally, 133 respondents (54.7%) reported being asked at least once by an insurance company to consider medication inappropriate for the patient (Supplementary Figure S3). Regarding sequelae of medication access issues limited to the past year, HCPs reported seizures (217, 89.3%), emergency room (ER) visits (191, 78.6%), unplanned clinic visits (134, 55.1%), urgent care visits (70, 28.8%), injuries (75, 30.9%), and deaths (8, 3.3%). 26 (10.7%) of HCPs were aware of a medication access issue ever leading to death of their patient. Finally, HCPs were invited to provide additional comments at survey completion. 52 (21%) submitted a total of 80 comments. The most common issues included insurance challenges (25), pharmacy distribution considerations (14), and administrative burdens (12), with selected responses in Supplementary Table S4.
Comparative Themes—Shared Concerns and Differing Priorities
Medication access was widely recognized as a significant concern among PWE, caregivers, and HCP, with common consequences including seizures, emergency healthcare utilization, and injuries due to not getting medication on time.
The experience of PWE and caregivers differed notably. Many caregivers were caring for children with epilepsy (70, 52.2%) and tended to care for individuals taking multiple daily ASMs. This difference likely accounts for caregivers reporting higher rates of difficulties across most barriers, except transportation. Caregivers also appeared to employ more compensatory strategies, as evidenced by their higher rate of reporting “no change” necessary compared to PWE.
HCPs cited insurance and cost as the most frequent barriers, though cost did not emerge as a top concern for PWE or caregivers. HCPs also reported concern about medication availability (eg, “out of stock/not available” or “too soon to fill”) and provider-related issues, but these were less frequently noted by PWE and caregivers, suggesting a relative lack of awareness for the frequency of these issues.
Discussion
Timely access to medication is a necessity and the most basic building block for medication adherence. However, multiple barriers limit PWE's ability to obtain medication promptly. These survey results provide insights into underlying barriers and resulting consequences.
65% of PWE and 72% of caregivers reported difficulty filling ASM prescriptions, resulting in negative financial consequences, stress, and seizures. Emergency medication use, injuries, and hospitalizations were also commonly reported. Nearly all HCP surveyed recognized medication access as a significant issue for PWE.
Medication Access Barriers
One notable finding, which has not been extensively evaluated in previous research, is the frequency of the “too soon to refill” message limiting medication access. This message was reported by 37% of PWE, 39% of caregivers, and 44% of HCP. Refills may be restricted due to legal, pharmacy, or insurance regulations. Many ASMs are categorized by the Drug Enforcement Administration (DEA) as Schedule III, IV, or V controlled substances, imposing limits on dispensed quantities and refill timing (often 2 days or less), which can vary by state and pharmacy. For daily medications, there is a narrow window of time between prescription filling and pick up before a dose is missed, and early refills for lost/damaged medication or travel may be denied. Newer and branded ASMs, which are often more expensive and less commonly stocked by pharmacies, may be particularly affected by these regulations, leading to delays in obtaining medication. Additionally, Schedule III and IV prescription transfers between pharmacies are permitted once. While this is an improvement passed by the DEA in 2023, 18 it is insufficient to address issues of medication access given current pharmacy stocking practices. When faced with these constraints, PWE may run out of medication, or need to search for alternative pharmacies, which can be difficult due to limited transportation, particularly in rural areas. These logistical challenges further burden HCPs who often must send prescriptions to the alternate pharmacy. DEA scheduling has been recognized by others as a significant barrier, 13 and de-scheduling, as done with fenfluramine and cannabidiol, could improve access, though concerns about abuse potential for some ASMs remains. 19
Cost was another significant barrier, with 20% of the PWE and 22% of caregivers reporting difficulty due to out-of-pocket expenses. Cost was also recognized by 57% of HCPs as a frequent barrier and is considered a primary obstacle to medication access globally. 20 High drug costs are not unique to epilepsy 21 and are a significant challenge in the current healthcare system. As newer medications tend to be more expensive, the pipeline of new drug approvals for epilepsy leads to cost challenges, including insurance coverage, need for prior authorizations (with greater paperwork burden to providers, delays, and system expense), 22 and higher out-of-pocket costs. The National Health Interview Survey, an annual health survey of US households that included epilepsy questions in 2015 and 2017, identified that excessive out-of-pocket medication costs can lead PWE to obtain and take less medication than prescribed, delay care and have difficulty paying bills compared to those without epilepsy. 12 In our study, 23% of PWE and 43% of caregivers reported delays due to lack of insurance coverage, with insurance identified by HCPs as the most frequent barrier to timely medication access. These findings underscore the role of insurance design and coverage limitations as structural drivers of nonadherence. Interestingly, a U.S. study of nearly 11,000 adults with epilepsy examining long-term costs of care found that ASM nonadherence was associated with higher overall healthcare costs, despite savings from reduced prescription drug spending. 11 Greater examination of the costs of nonadherence may help establish common ground for meaningful insurance policy reform.
Effects of Barriers
Seizures, increased healthcare utilization, and even death are possible sequelae from missed doses. In our survey, PWE reported experiencing seizures (27%) and ER visits (8%) after a missed dose(s). A postal survey of 661 PWE found similar results: 45% with missed doses reported consequent seizures 23 and another study associated a medication possession ratio of <0.8 with 21% higher risk of seizure. 24 The RANSOM study, a retrospective open-cohort analysis of Medicaid claims data, found a threefold increased mortality in those with nonadherence, with non-adherent time periods associated with significantly higher incidence of ER visits, hospitalizations, injuries from motor vehicle accidents, and fractures. 10 Another claim-based study found similar findings with ASM nonadherence associated with an increased likelihood of hospitalization and ER admission. 11 Seizures can lead to death, and our HCP survey disturbingly revealed that over 10% reported at least one patient death from a medication access issue.
The negative impact of seizures on quality of life is well-documented and can be “immediate and devastating.” 25 Accordingly, 25% of caregivers reported emotional or other stress due to difficulties filling medication. Our findings align with previous research 26 showing that non-drivers are more likely to report transportation as a barrier to obtaining medication. A 1997 survey of people with moderately severe epilepsy identified driving, independence, and employment as the most important concerns, 27 noting that a single seizure can lead to loss of driving privileges. Access to medication is therefore critical in maximizing the quality of life for PWE.
Limitations
Our surveys have several limitations. First, there is inherent self-selection bias in survey participants, potentially motivated by frustrations. Likewise, the caregivers surveyed managed more daily medications than average epilepsy populations. Both could have resulted in a higher frequency of reported barriers.
However, the distribution lists targeted audiences that were connected to epilepsy support networks, which can provide guidance on navigating through these barriers, potentially making these an under-reporting of true difficulties. In addition, web-based surveys are more likely to be completed by those with higher education, internet access, and computer skills, and our surveys did not have a paper option to reach those without access. Similarly, the surveys were not provided in any languages other than English, limiting completion to those with English proficiency or access to translation. For these reasons, our results may underestimate barriers, as education, support networks, and electronic resources can be invaluable to overcome medication access issues.
Many survey participants chose not to provide demographic characteristics, limiting characterization of our responders. Most HCP responses were from epileptologists, which may not reflect primary care or general neurology experience. Overall low response rates to the surveys suggest possible non-response bias.
Finally, these surveys clarified the difficulty of getting medications filled on time but did not evaluate the challenges of establishing care, medication understanding, remembering to take medication, side effects, and comorbid conditions that are also critical elements in epilepsy treatment.
Despite these limitations, the surveys reflect the barriers encountered in the populations sampled, are consistent with other studies, and clearly demonstrate evidence of systemic burden and need for change.
Next Steps
Missed medication doses have far reaching consequences, including death. Obtaining medication on time must be a priority for insurers, pharmacies, governing bodies, HCPs, and the epilepsy community. The following position statement was created by the AES Medication Access Workgroup to highlight these critical concerns and present a framework for positive change.
American Epilepsy Society Position Statement
The AES is committed to improving outcomes for PWE. ASMs are an essential component of epilepsy care, and timely access is critical. In AES surveys, 65% of PWE and 72% of caregivers reported difficulty obtaining medications, with 95% of HCPs recognizing access as a problem. Cost can lead to PWE taking less medication
12
and nonadherence leads to higher healthcare expenses, despite savings from reduced cost of medication.
11
Missed medication leads to seizures, ER visits, injuries, and hospitalizations.10,11,23,24 11% of surveyed HCPs reported patient death resulting from medication access delay. Meaningful change requires coordinated action from clinicians, insurers, regulators, pharmacy associations, legislators, and advocacy groups. The AES supports coordinated efforts among these stakeholders to eliminate unnecessary barriers to medication access through the following principles:
Regulatory Reform:
Rationale: Survey data revealed “too soon to refill” as the most common barrier reported by PWE (37%), caregivers (39%), and HCPs (44%). Controlled substance regulations were the most frequently cited issue in HCP free-text responses (34%), with DEA scheduling creating narrow refill windows that lead to missed doses when pharmacies lack stock.
Improve Availability:
Rationale: Medication unavailability was the second most common barrier for PWE (25%) and the most common barrier for caregivers (54%), indicating widespread supply chain disruptions affecting timely access.
Insurance Reform:
Rationale: Insurance was identified by HCPs as the most frequent barrier to medication access. In our survey, 55% of HCPs reported being asked by insurers to prescribe medications inappropriate for their patients. Insurance coverage barriers affected 23% of PWE and 43% of caregivers.
Streamline prior authorization Eliminate step-therapy requirements that contradict evidence-based epilepsy management Advocate for automatic continuation of medication coverage Transparency of coverage and copayment when selecting an insurance plan Cost Containment:
Rationale: Cost barriers affected 20% of PWE and 22% of caregivers for out-of-pocket expenses. HCPs identified cost as a frequent barrier (57%), highlighting the need for pricing transparency and cost controls.
Practice Support and Education:
Rationale: Access barriers resulted in breakthrough seizures (27% of PWE), skipped doses (21% of PWE), inability to obtain rescue medications (29% of PWE), and significant emotional stress (25% of caregivers).
Research:
The AES remains committed to promoting research and surveillance on access-related outcomes
Conclusions
Medication access barriers are widespread and significant per PWE, caregivers, and HCP. Survey findings demonstrate need for action to reduce modifiable barriers and risks. Even with established care, medication is not always obtained promptly to prevent missed doses. Obtaining medication is a crucial step for medication adherence and relies on a multitude of factors, many beyond the patient's or provider's control. Missed medication increases the cost of care and burdens HCP staff. Action plans, advocacy, education, and awareness are critical to reducing complications related to missed doses. Further research is needed to clarify the most effective strategies to reduce missed medications. There is an urgent and critical need to implement systemic changes before another person with epilepsy dies unnecessarily.
Supplemental Material
sj-docx-1-epi-10.1177_15357597261435471 - Supplemental material for On Time Saves Lives: Survey Insights and Position Statement from the American Epilepsy Society on Barriers to Antiseizure Medication Access
Supplemental material, sj-docx-1-epi-10.1177_15357597261435471 for On Time Saves Lives: Survey Insights and Position Statement from the American Epilepsy Society on Barriers to Antiseizure Medication Access by Marjorie E. Bunch, Jessica Falco-Walter and Sasha Alick-Lindstrom, Abrar O. Al-Faraj, Brandy E. Fureman, James Herbst, Lisa C. Garrity, Shilpa Klocke, Alain Lekoubou, Lara V. Marcuse, Lauren Orciuoli in Epilepsy Currents
Supplemental Material
sj-docx-2-epi-10.1177_15357597261435471 - Supplemental material for On Time Saves Lives: Survey Insights and Position Statement from the American Epilepsy Society on Barriers to Antiseizure Medication Access
Supplemental material, sj-docx-2-epi-10.1177_15357597261435471 for On Time Saves Lives: Survey Insights and Position Statement from the American Epilepsy Society on Barriers to Antiseizure Medication Access by Marjorie E. Bunch, Jessica Falco-Walter and Sasha Alick-Lindstrom, Abrar O. Al-Faraj, Brandy E. Fureman, James Herbst, Lisa C. Garrity, Shilpa Klocke, Alain Lekoubou, Lara V. Marcuse, Lauren Orciuoli in Epilepsy Currents
Supplemental Material
sj-docx-3-epi-10.1177_15357597261435471 - Supplemental material for On Time Saves Lives: Survey Insights and Position Statement from the American Epilepsy Society on Barriers to Antiseizure Medication Access
Supplemental material, sj-docx-3-epi-10.1177_15357597261435471 for On Time Saves Lives: Survey Insights and Position Statement from the American Epilepsy Society on Barriers to Antiseizure Medication Access by Marjorie E. Bunch, Jessica Falco-Walter and Sasha Alick-Lindstrom, Abrar O. Al-Faraj, Brandy E. Fureman, James Herbst, Lisa C. Garrity, Shilpa Klocke, Alain Lekoubou, Lara V. Marcuse, Lauren Orciuoli in Epilepsy Currents
Supplemental Material
sj-docx-4-epi-10.1177_15357597261435471 - Supplemental material for On Time Saves Lives: Survey Insights and Position Statement from the American Epilepsy Society on Barriers to Antiseizure Medication Access
Supplemental material, sj-docx-4-epi-10.1177_15357597261435471 for On Time Saves Lives: Survey Insights and Position Statement from the American Epilepsy Society on Barriers to Antiseizure Medication Access by Marjorie E. Bunch, Jessica Falco-Walter and Sasha Alick-Lindstrom, Abrar O. Al-Faraj, Brandy E. Fureman, James Herbst, Lisa C. Garrity, Shilpa Klocke, Alain Lekoubou, Lara V. Marcuse, Lauren Orciuoli in Epilepsy Currents
Supplemental Material
sj-pdf-5-epi-10.1177_15357597261435471 - Supplemental material for On Time Saves Lives: Survey Insights and Position Statement from the American Epilepsy Society on Barriers to Antiseizure Medication Access
Supplemental material, sj-pdf-5-epi-10.1177_15357597261435471 for On Time Saves Lives: Survey Insights and Position Statement from the American Epilepsy Society on Barriers to Antiseizure Medication Access by Marjorie E. Bunch, Jessica Falco-Walter and Sasha Alick-Lindstrom, Abrar O. Al-Faraj, Brandy E. Fureman, James Herbst, Lisa C. Garrity, Shilpa Klocke, Alain Lekoubou, Lara V. Marcuse, Lauren Orciuoli in Epilepsy Currents
Footnotes
Acknowledgments
The authors would like to acknowledge the American Epilepsy Society, with workgroup formation supported by the Treatments Committee led by John Stern, MD, MA, FAES with initial collaboration facilitated by former AES employee Joy Keller, MS, RD, MSLIS. Additional acknowledgement and appreciation to Shawna Strickland, PhD, CAE, RRT, FAARC for subject matter expertise on survey development.
Appreciation goes to the respondents for taking the time to complete the surveys, as well as the institutions that assisted with survey distribution, including the American Epilepsy Society, American Academy of Neurology, Epilepsy Foundation, Epilepsy Leadership Council, and Rare Epilepsy Network. The authors also express appreciation for statistical analysis provided by Paul J. Feustel, PhD.
Author Contributions
All authors reviewed and approved the final manuscript. MEB was responsible for the study conception and survey creation, first draft manuscript, data analysis and processing, and revision and editing. JFW and SAL assisted in survey creation, data analysis and processing, manuscript preparation, and revision and editing. AOAF and BEF assisted with manuscript preparation, data analysis and processing, and revision and editing. JH, LCG, SK, AL, and LO assisted in study conception, survey creation, manuscript preparation, data analysis and processing, and revision and editing. LVM assisted in study conception, survey creation, and manuscript revision and editing.
Disclosure & Ethical Statement
No pharmaceutical company contributed to or reviewed this manuscript in any stage of development. Dr Fureman is the owner and principal of Neuroscience Navigators, LLC. No other authors have any disclosures relevant to this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.