
Abstract
Drug-resistant epilepsy (DRE) may lead to substantial morbidity, impaired quality of life (QoL), and increased mortality. Clinicians increasingly use surgical interventions to manage DRE, but uncertainty remains regarding their comparative benefits and harms across epilepsy syndromes. We conducted 4 systematic reviews and meta-analyses to inform the American Epilepsy Society (AES) and Congress of Neurological Surgeons (CNS) guidelines on surgical management of DRE. We searched MEDLINE, Embase, and CENTRAL from inception to August 2024 for randomized controlled trials (RCTs) and nonrandomized studies (NRS). We evaluated (1) resective or ablative surgery versus medical therapy in drug-resistant mesiotemporal lobe epilepsy (DR-MTLE); (2) resective or ablative surgery versus medical therapy in drug-resistant neocortical epilepsy (DR-NE); (3) callosotomy versus vagus nerve stimulation (VNS) in developmental and epileptic encephalopathies (DEEs) with drop attacks; and (4) ablative versus resective surgery in hypothalamic hamartoma (HH). The panel prioritized the following critical outcomes: seizure freedom, QoL, neuropsychological, neuropsychiatric, and social outcomes, and serious adverse events. We assessed certainty of evidence using the Grading of Recommendations Assessment, Development and Evaluation approach. We included 47 studies comprising 4868 participants. In DR-MTLE, moderate-certainty evidence from RCTs showed that anterior temporal lobectomy (ATL), compared with medical therapy, probably increases seizure freedom and improves QoL. The evidence was very uncertain regarding the effects of selective amygdalohippocampectomy, laser interstitial thermal therapy (LITT), and radiosurgery in patients with DRE. In DR-NE, very low-certainty evidence suggested that seizure freedom may occur after resective surgery. However, we did not identify any eligible studies evaluating ablative surgery in this population. In DEE, very low-certainty evidence suggested that, when compared to VNS, callosotomy may improve seizure outcomes but may also increase serious adverse events. In HH, evidence for LITT and radiosurgery was found to be very uncertain. Across reviews, the most common reason for downgrading the certainty of evidence was risk of bias and imprecision. Moderate-certainty evidence supports ATL in selected patients with DR-MTLE. For other surgical approaches and epilepsy syndromes, the evidence remains very uncertain, highlighting the need for better comparative studies.
Keywords
Introduction
Drug-resistant epilepsy (DRE) is defined as the failure of 2 appropriately selected and tolerated antiepileptic (antiseizure) medications to achieve sustained seizure freedom, either as monotherapy or in combination. 1 Approximately 36% of patients with epilepsy develop DRE, and nearly 20% of newly diagnosed cases will become drug resistant. 2
The etiologies of DRE are heterogeneous and include mesiotemporal sclerosis, focal cortical dysplasia, epileptogenic tumors, genetic epilepsies, and acquired brain injuries,3,4 affecting both pediatric and adult populations.5,6 Recurrent and uncontrolled seizures may disrupt neurodevelopment in children, contribute to progressive cognitive decline in adults, and are associated with psychiatric comorbidities and impaired quality of life (QoL) across age groups.7,8
Management options for DRE include continued medical therapy, resective surgery, ablative procedures including laser interstitial thermal therapy (LITT) and radiosurgery, and neuromodulation therapies such as vagus nerve stimulation (VNS), deep brain stimulation (DBS), and responsive neurostimulation (RNS).9–13 Current guidelines recommend referral to specialized epilepsy centers following failure of 2 antiseizure medications and consideration of surgical management in appropriate candidates.12,14 Although resective procedures such as anterior temporal lobectomy (ATL) have been used for decades, newer and less invasive approaches, including LITT, selective amygdalohippocampectomy (SAH), and radiosurgery, have expanded the surgical options available to patients with DRE. The primary goals of treatment are seizure freedom and improvement in QoL.15–17
Despite increasing use of surgical interventions, the evidence informing clinical practice remains limited and of low quality due to heterogeneity across studies related to populations, interventions and reported outcomes. Also, some existing recommendations are based on evidence that was not systematically identified, assessed and synthesized, or on outdated systematic reviews, and focus primarily on seizure outcomes, with less emphasis on other patient-important outcomes, such as QoL, neuropsychological, and neuropsychiatric outcomes.9,13,18 Thus, uncertainty persists regarding the comparative effectiveness and safety of different surgical approaches on patient-important outcomes used for decision-making. These limitations underscore the need for a comprehensive and up-to-date synthesis of the available evidence.
Thus, we conducted 4 systematic reviews to evaluate the effectiveness of resective and ablative surgical approaches, across key clinical contexts in DRE including mesiotemporal and neocortical epilepsy, epileptic encephalopathies with drop attacks, and hypothalamic hamartomas (HHs). These reviews informed the guideline development effort on surgical management of DRE by the American Epilepsy Society (AES) and Congress of Neurological Surgeons (CNS).
Methods
We reported these systematic reviews in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist 19 (Supplemental Material S1). We registered our protocol in PROSPERO (CRD42024494990).
We addressed 4 systematic review questions prioritized by the guideline panel from AES and CNS. The population, intervention, comparator and outcome (PICO) questions are detailed below:
PICO 1: How do resective or ablative surgical procedures, including ATL, SAH, LITT or radiosurgery, compare to medical therapy for the treatment of patients with drug-resistant mesiotemporal epilepsy, including hippocampal sclerosis? PICO 2: How does resective or ablative epilepsy surgery compare to medical therapy for treatment of patients with drug-resistant neocortical epilepsy? PICO 3: How does callosotomy (complete or partial) compare to VNS for treatment of patients with drug-resistant drop attacks (ie, seizures causing sudden falls, such as atonic, or tonic seizures) associated with developmental epileptic encephalopathies (DEEs) (eg, Lennox-Gastaut Syndrome [LGS], West Syndrome/infantile spasms, Ohtahara Syndrome)? PICO 4: How does LITT or radiosurgery compare to surgical resection for the treatment of patients with HHs?
The AES/CNS guideline panel selected and prioritized patient-important outcomes through outcome ranking surveys and panel discussions. Prioritized outcomes across all 4 reviews included (1) improvement in seizure outcomes (seizure freedom), (2) neuropsychological outcomes (verbal memory, naming receptive language, verbal fluency, and IQ in adults and children; as well as psychomotor development and daily activities in children), (3) neuropsychiatric outcomes (personality changes, depression, anxiety, psychosis in adults and children, and behavior changes in children), (4) social outcomes (employment and driving in adults, schooling and social functioning in children), (5) QoL, and (6) serious adverse events (including sudden unexpected death in epilepsy [SUDEP], permanent and unexpected neurological deficits, medical or surgical complications or adverse events).
Eligibility Criteria
We included published randomized controlled trials (RCTs) and comparative and noncomparative nonrandomized studies (NRSs), including prospective and retrospective cohort studies and case series. For studies with between-group comparisons, we included studies regardless of sample size. For studies reporting only within-group (before–after) comparisons, we included studies with sample sizes of ≥100 participants for the first 2 systematic reviews and ≥30 participants for the last 2 systematic reviews. We considered studies eligible if at least 70% of participants represented our population of interest. We excluded studies with follow-up durations of less than 1 year. Specific eligibility criteria for each systematic review are described in Supplemental Material S3.
Search Strategy
For each systematic review, we searched Ovid MEDLINE, Embase, and CENTRAL from inception to August 29, 2024 (Supplemental Material S2). Previously published search strategies 20 informed the searches for the first 2 reviews. We did not apply any language or study design restrictions. In December 2024, we consulted with the AES and CNS guideline panel to identify potentially relevant studies not captured through our electronic database searches.
Study Selection
Following training and calibration, pairs of reviewers independently screened titles and abstracts and subsequently full-text articles using Covidence software (https://covidence.org/). We resolved disagreements through discussion or consultation with a third reviewer when necessary.
Data Collection
Pairs of reviewers completed training and calibration exercises using a standardized data extraction form. One reviewer extracted the data, and a second reviewer verified all extracted information. 21 We resolved discrepancies through consensus and, when necessary, consultation with a third reviewer.
We extracted data on study and participant characteristics, intervention details, and outcomes measured using any validated instrument at any reported follow-up time. We categorized follow-up periods as short-term (1 to <2 years postoperatively), medium-term (≥2 and ≤5 years), and long-term (> 5 years).
Risk of Bias Assessment
Pairs of reviewers assessed risk of bias for all outcomes across included studies. One reviewer performed the assessment, and a second reviewer verified all judgments. 21 For RCTs, we used Cochrane RoB 2.0 tool to rate studies as definitely low, some concerns, or high across the tool's 5 domains: randomization, deviations from intended intervention, missing outcome data, measurement of the outcome, and selection of reported results. 22 For NRSs, we used ROBINS-I and rated studies as low, moderate, serious across 7 domains: confounding, selection of participants, classification of the intervention, deviation from intended intervention, missing data, measurement of the outcome, and selection of reported results. 23
Data Synthesis
We followed Cochrane guidance for data synthesis.24,25 When appropriate, we conducted meta-analyses using the DerSirmonian-Laird random effects method 26 ; otherwise, when meta-analysis was not possible, we summarized the reported effect estimates of the included studies. 25
For dichotomous outcomes, we used the Mantel-Haenszel method and summarized effects as risk ratios (RRs), odds ratios (ORs), or proportions of events, as appropriate. We calculated absolute effects per 1000 patients using the baseline risk from the control group of the included studies.
For continuous outcomes, we applied the inverse-variance method and summarized effects as mean differences (MDs) when possible. When outcomes were measured using different instruments, we converted estimates to the instrument considered most familiar and interpretable. We calculated 95% confidence intervals (CIs) for all estimates.
We conducted analyses using STATA 27 and DataParty (https://dataparty.ca/).
Subgroup and Sensitivity Analyses
For all systematic reviews, the guideline panel prioritized reporting intervention effects separately for adult and pediatric populations, irrespective of statistical heterogeneity. We analyzed studies including mixed-age populations (<70% adult or pediatric participants) separately and compared results with the primary analyses. Studies with ≥70% adult or pediatric participants were included in their respective subgroup analyses.
We planned the following subgroup analyses as detailed below:
Systematic review 1:
Age: Pediatric (12 years through <18) versus adults (>18 years). Mesiotemporal sclerosis is considered very rare in patients less than 12 years old.
Systematic review 2:
Age: Infants (<2 years) versus pediatric (2 through <18 years) versus adults (>18 years).
Systematic review 3:
Population Subgroups:
Age: Infants (<2 years) versus pediatric (ages 2 through <18 years) versus adults (ages >18 years) Seizure type: Drop attack/drop seizures and atonic seizures versus not Condition: Patients with DEE, and West syndrome/infantile spasms, and Ohtahara syndrome, versus patients with LGS.
Systematic review 4:
Population ages: Infants (<2 years), versus pediatric (ages 2 through <18 years), versus adults (ages >18 years).
We hypothesized that intervention effects on seizure outcomes would be larger among infant and pediatric populations, individuals with drop-attack seizures, and those with LGS. However, due to limited data availability, subgroup analyses were not feasible. We did not plan to conduct any sensitivity analyses. 28
Certainty of Evidence Assessment
We assessed the certainty of evidence using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach. 29 Following contemporary GRADE guidance for questions addressing intervention effects, including those informed by observational studies, all bodies of evidence initially began at high certainty 30 and could be rated down due to risk of bias, imprecision, inconsistency, indirectness, or publication bias.28,31–34
In all reviews, we used the null effect as our single threshold to make a judgment regarding imprecision (1 for relative measures, 0 for absolute measures, and MDs or mean changes). We did not establish a minimally important difference to infer whether an effect was clinically important or not. We assessed the effects of epilepsy surgery on health outcomes as causal effects rather than associations, including when evidence originated from observational studies not explicitly designed for causal inference. Consistent with GRADE guidance for intervention questions, we defined the target question, 35 clarified its causal intent, and assessed the certainty of the evidence. 36
We constructed Evidence Profile tables using GRADEpro for each PICO question. 37 Whenever possible, we reported relative and absolute estimates of effect per outcome.
Results
Search Results
For systematic reviews 1 and 2, we screened the titles and abstracts of 19 724 unique citations and the full texts of 1277 articles. As for systematic reviews 3 and 4, we screened 9022 unique titles and abstracts and 751 full texts. Figure 1 summarizes the search and selection process for the 4 reviews. Individual PRISMA flowcharts for each review are available in Supplemental Material S4.
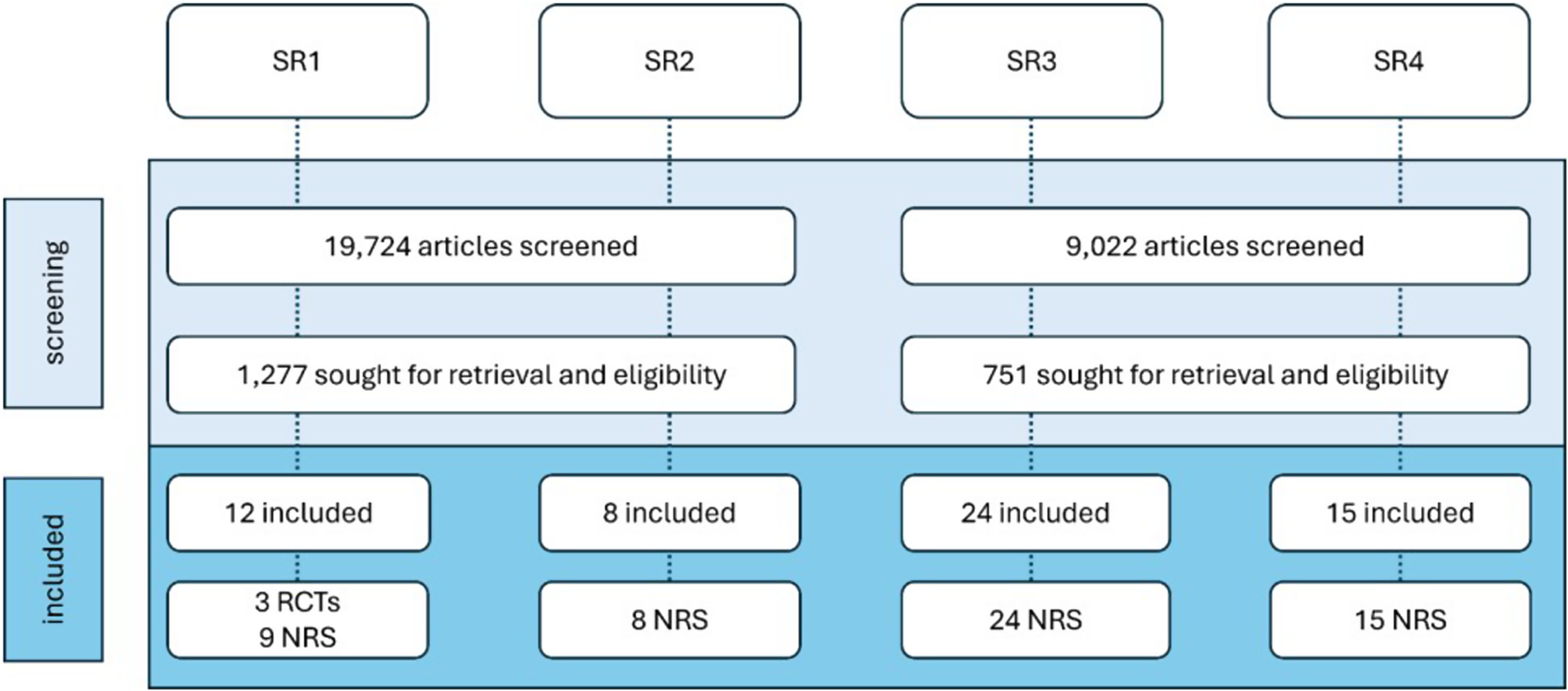
Summary of study selection process per systematic review.
Systematic Review 1: Resective or Ablative Surgery Versus Medical Therapy in Patients With DR-MTLE
We included 3 RCTs38–40 and 9 NRS41–49 comprising a total of 1810 participants. Across studies, the mean age was 38 years and 51% of participants were female. Six studies38,39,41–44 evaluated ATL, 1 NRS 45 evaluated SAH, another 4 NRSs46–49 assessed LITT, and 1 RCT 40 assessed radiosurgery; for the radiosurgery trial, we used only data from the radiosurgery arm. Supplemental Table S5 provides a summary of characteristics of included studies.
We found the included RCTs to be at high risk of bias due to concerns with outcome measurement, deviation from intended intervention and missing outcome data; and the included NRS studies to be at critical risk of bias due to confounding, missing outcome data and concerns with outcome measurement (Supplemental Material S6, Supplemental Figures S3 and S4).
Below, we present the effects of the interventions per comparison, on the outcomes that the AES/CNS guideline panel considered key for decision-making. Tables 1–4 provide the evidence profiles for the key outcomes. We provide the effects on all other outcomes judged as important for decision-making in Supplemental Material S1 (Supplemental Material S7) and the forest plots for all related meta-analyses (Supplemental Material S8).
Comparison 1: ATL Versus Medical Therapy
Seizure freedom. When compared to medical therapy, moderate-certainty evidence suggests that ATL probably increases freedom from all seizures, including auras, at short-term follow-up (RR 15.00, 95% CI [2.08 to 108.23]; RD 350 per 1000, 95% CI [27 to 1000]; n = 1 RCT 39 and 80 participants; 1-year follow-up), and freedom of disabling seizures at short-term (RR 7.67, 95% CI [2.50-23.51]; RD 550 per 1000, 95% CI [112 to 1000]; n = 1 RCT 39 and 80 participants; 1-year follow-up) and medium-term follow-up (RR 34.50, 95% CI [2.18 to 545.02]; RD 838 per 1000, 95% CI [30 to 1000]; n = 1 RCT 38 and 38 participants; 2-year follow-up).
Additionally, low-certainty evidence suggests that ATL may increase seizure freedom at short-term (RR 5.10, 95% CI [2.67 to 9.75]; RD 563 per 1000, 95% CI [229 to 1000]; n = 1 NRS 41 and 1034 participants; mean follow-up 1 year), medium-term (RR 4.58, 95% CI [3.61 to 5. 80]; RD 580 per 1000, 95% CI [423 to 778]; n = 3 NRS42–44 and 838 participants; 2 to 5 years follow-up) and longest follow-up (RR 4.36, 95% CI [3.16 to 6.02]; RD 601 per 1000, 95% CI [386 to 897]; n = 2 NRS42,43 and 424 participants; 10 to 17 years follow-up).
QoL. When compared to medical therapy, moderate-certainty evidence suggests that ATL probably improves QoL [measured with the QoL in Epilepsy-89 tool (QOLIE-89); score range 0 to 100; higher scores indicate better QoL] at short-term (MD 17.53, 95% CI [11.91 to 23.14]; n = 2 RCTs38,39 and 118 participants; 1-year follow-up) and medium-term follow-up (MD 8.5, −1.00 to 18.1; n = 1 NRS 41 and 38 participants; 2-year follow-up).
Serious adverse events. Low-certainty evidence suggests that ATL probably increases the risk of permanent, unexpected neurological deficits (decline in verbal memory that interfered with the patients’ occupation), at short-term follow-up (RR 4.00, 95% CI [0.19 to 85.99]; RD 38 per 1000, 95% CI [−10 to 1000]; n = 1 RCT 39 and 80 participants; 1-year follow-up).
Other outcomes. We are very uncertain about the effects of ATL on all-cause mortality, medical or surgical complications, neuropsychological outcomes (verbal memory and naming), neuropsychiatric outcomes (depression and psychosis), and social outcomes (employment and driving) (Supplemental Material S7).
We did not identify eligible studies reporting on the other prioritized patient-important outcomes including SUDEP, medical or surgical complications (intracerebral hemorrhage with neurological deficits), neuropsychological outcomes (receptive language, verbal fluency, IQ), or neuropsychiatric outcomes (personality changes, anxiety).
Comparison 2: SAH Versus Medical Therapy
Seizure freedom. When compared to medical therapy, very low-certainty evidence from a single NRS 45 (n = 19) suggests that SAH may increase seizure freedom (absence of seizures that caused impairment of consciousness), at medium-term follow-up (RR 14.25, 95% CI [0.95 to 214.03]; RD 133 per 1000, 95% CI [−1 to 1000]; 2 years follow-up).
QoL. When compared to medical therapy, very low-certainty evidence from a single NRS 45 (n = 12), suggests that SAH may improve QoL [measured with the QoL in Epilepsy Inventory (QOLIE-10); score range 10 to 50; higher scores indicate worse QoL) at medium-term follow-up (MD −10.5, 95% CI [−21.61 to 0.61]; n = 12; 2-year follow-up).
Neuropsychological outcomes. When compared to medical therapy, very low-certainty evidence from a single NRS 45 (n = 19) suggests that SAH may decrease verbal memory (Verbaler Lernund Merkfähigkeitstest; z-scores; higher scores indicate improvement in verbal memory) at medium-term follow-up (MD −16.02, 95% CI [−30.96 to −1.08]; mean follow-up 2 years) and Intelligence Quotient (IQ) scores may decrease (Hamburg-Wechsler Intelligence Test for Adults - Revision, z-scores; higher scores indicate better IQ) at medium-term follow-up (MD −3.36, 95% CI [−15.5 to 8.78]; mean follow-up 2 years).
Other outcomes. We are very uncertain about the effects of SAH on neuropsychiatric outcomes (depression) and social outcomes (employment) (Supplemental Materials S1 and S7).
We did not identify eligible studies reporting on the other prioritized patient-important outcomes including permanent, unexpected neurological deficits (excluding visual field deficits, expected with some surgical procedures), all-cause mortality, SUDEP, medical or surgical complications (brain infection, intracerebral hemorrhage with neurological deficits, serious adverse events), neuropsychological outcomes (naming, receptive language, verbal fluency), neuropsychiatric outcomes (personality changes, anxiety, psychosis), or social outcomes (driving).
Comparison 3: LITT Versus Medical Therapy
Seizure freedom. In participants undergoing LITT, very low-certainty evidence from a meta-analysis of 3 NRS46–48 (n = 434) suggests seizure freedom, classified as Engel I, may occur in 52% (225/434) participants at short-term follow-up (1 year).
All-cause mortality. Very low-certainty evidence from 2 NRS47,48 (n = 412) suggests that 2% (8/412) participants may die over medium-term follow-up (median follow-up of 3.75 years) after undergoing LITT.
Serious adverse events. Very low-certainty evidence from a single NRS 47 (n = 277) suggests SUDEP may occur in 0.4% (1/277) of participants at short-term follow-up (1-year follow-up) after undergoing Magnetic-Resonance-Image-guided-LITT (MRgLITT). While another NRS 48 (n = 135) suggests it may occur in 3% (4/135) participants at medium-term follow-up after undergoing LITT (median follow-up 3.5 years). Similarly, very low-certainty evidence from a single NRS 47 (n = 277) suggests medical or surgical complications, defined as symptomatic intracranial hemorrhage, may occur in 0.4% (1/277) participants after undergoing MRgLITT at medium-term follow-up (median follow-up 4 years).
Neuropsychological outcomes. Very low-certainty evidence from one NRS 46 (n = 40) suggests there may be little to no change in verbal memory (measured with Rey Auditory Verbal Learning Test) at short-term follow-up after undergoing LITT (mean change from baseline 0.91, 95% CI [−0.32 to 2.14]; 1-year follow-up).
Other outcomes. We are very uncertain about the effects of LITT on all-cause mortality, SUDEP, and medical or surgical complications (symptomatic intracranial hemorrhage) (Supplemental Material S7).
We did not identify eligible studies reporting on the other prioritized patient-important outcomes including permanent, unexpected neurological deficits (excluding visual field deficits, expected with some surgical procedures), medical or surgical complications (brain infection, serious adverse events), QoL, neuropsychological outcomes (naming, receptive language, verbal fluency, IQ), neuropsychiatric outcomes (personality changes, depression, anxiety, psychosis), or social outcomes (employment, driving).
Comparison 4: Radiosurgery Versus Medical Therapy
All outcomes were informed by single-arm data from the radiosurgery arm of one RCT 40 comparing radiosurgery versus ATL. We analyzed only data from participants who underwent radiosurgery.
Seizure freedom. Very low-certainty evidence from the radiosurgery arm of one RCT 40 (n = 31) suggests there may be seizure freedom classified as Engel I in 13% (4.31) participants after undergoing radiosurgery at short-term follow-up (1 year).
Serious adverse events. Very low-certainty evidence from the radiosurgery arm of one RCT
40
(n
QoL. When measured with the QOLIE-89 instrument, very low-certainty evidence from the radiosurgery arm of one RCT 40 (n = 23) suggests there may be an improvement in QoL in the short-term (mean change 0.57, 95% CI [−0.05 to 7.19]; 1-year follow-up) and medium-term follow-up (mean change 7.61, 95% CI [−0.30 to 15.47]; 3 years follow-up) after undergoing radiosurgery.
Neuropsychological. When measured with the California Verbal Learning Test, very low-certainty evidence from the radiosurgery arm of one RCT 40 (n = 14) suggests there may be an increase in verbal memory in the short-term (mean change 0.6, 95% CI [−1.32 to 2.53]; 1-year follow-up), but a decline at medium-term follow-up (mean change −0.38, 95% CI [−2.00 to 1.23]; 3 years follow-up) after undergoing radiosurgery.
Other outcomes. We did not identify eligible studies reporting on the other prioritized patient-important outcomes including all-cause mortality, SUDEP, medical or surgical complications (brain infection, intracerebral hemorrhage with neurological deficits), neuropsychological outcomes (naming, receptive language, verbal fluency, IQ), neuropsychiatric outcomes (personality changes, depression, anxiety, psychosis), or social outcomes (employment, driving).
Systematic Review 2: Resective or Ablative Surgery Versus Medical Therapy in Patients With DR-NE
We included 8 NRS50–57 and a total of 1867 participants. Across studies, mean age was 25 years among adults, with 48% female. Four NRS50,51,54,57 reported the neocortical temporal lobe as the most frequent surgical lobe location among participants, while 3 NRS52,53,56 reported the frontal lobe. One NRS 55 did not report a surgical location. A summary of study and participant characteristics is available in Supplemental Material S5, Supplemental Table S2.
We found the included studies to be at critical risk of bias due to prognostic factor imbalances, lack of a control group, and concerns with outcome measurement (Supplemental Material S6, Supplemental Figure S5).
Below, we present the summary of effects of the interventions per comparison, on the outcomes that the AES/CNS guideline panel considered key for decision-making (Table 5). We provide the effects on all other outcomes judged as important for decision making in Supplemental Material S1 (Supplemental Material S9).
Comparison 1: Resective Surgery Versus Medical Therapy
Seizure freedom. For seizure freedom classified as Engel I, we found very low-certainty evidence from 2 NRS,51,54 comprised of around 80% pediatric participants, suggesting that 57% (255/446) participants may achieve seizure freedom after undergoing resective surgery at short-term follow-up (1 year). Very low-certainty evidence from one adult NRS 57 suggests that 65% (72/110) participants may achieve seizure freedom classification Engel I at short-term follow-up. At the longest follow-up (6 years), very low-certainty evidence from 4 NRS51,52,54,55 with 80% pediatric participants, suggests that 51% (304/591) participants may achieve seizure freedom) after resective surgery. Very low-certainty evidence from 2 NRS52,56 suggests that 61% (61/124) adult participants may achieve seizure freedom Engel Ia at the longest follow-up (6 years).
Serious adverse events. At the longest follow-up (6 years), very low-certainty evidence from 2 NRS52,55 suggests that 3.3% (7/211) pediatric participants may present with permanent, unexpected neurological deficits after resective surgery. Very low-certainty evidence from 1 adult NRS 52 suggests that 1.5% (1/66) of participants may experience these deficits.
In terms of medical or surgical complications at the longest follow-up, very low-certainty evidence from one pediatric NRS 55 (n = 171) suggests that participants may not experience intracranial hemorrhage after undergoing resective surgery, but brain infection may occur in 0.58% (1/171) participants (5 years follow-up). Another NRS 56 with mixed-age participants, suggests that, after undergoing radiosurgery, 5.2% (3/58) of participants may have a surgical complication (3.5% had cerebrospinal fluid leak and 1.7% had a site infection; 6 years follow-up), but the evidence is very uncertain.
All-cause mortality. Very low-certainty evidence from 2 NRS with 359 participants (171 pediatrics, 55 188 mixed population 53 ) suggests there may be no deaths reported after resective surgery.
QoL. When measured with the QOLIE-89 instrument, very low-certainty evidence from a single NRS 57 with 110 adult participants suggests that there may be an improvement in the QoL at short-term follow-up (mean change 10.8, SD 3.97; 1-year follow-up) after resective surgery.
Neuropsychological outcomes. Very low-certainty evidence from one NRS 55 comprised of pediatric participants suggests there may be an improvement in cognitive status (measured with multiple instruments; unspecified) in 48% (43/171) participants, and a decline in 3% (5/171) participants at medium-term follow-up (5 years) after resective surgery. For adults, one NRS 52 suggests that 41% (27/66) participants may have cognitive improvement (measured with a standard neuropsychological test battery; unspecified), 6% (4/66) may worsen, and 35% (23/66) may have no change at the longest follow-up (median of 9 years), but we are very uncertain.
Other outcomes. We are also very uncertain about the effects of resective surgery on neuropsychiatric outcomes (behavior) and social outcomes (employment and school performance) (Supplemental Material S9).
We did not identify eligible studies reporting on the other prioritized patient-important outcomes including long-term mortality, SUDEP, neuropsychological outcomes (verbal memory, naming receptive language, verbal fluency, IQ), neuropsychiatric outcomes (personality changes, anxiety psychosis), or social outcomes (driving).
Comparison 2: Ablative Surgery (LITT and Radiosurgery) Versus Medical Therapy
We did not identify any eligible studies reporting on these interventions.
Systematic Review 3: Callosotomy Versus VNS in Patients With DR-Drop Attack, LGS or DEE
For this review, we followed the panel's decision to report intervention effects separately for adult and pediatric populations. We included 8 NRS58–65 comprising 221 adult participants and 16 NRS66–81 comprising 459 pediatric participants (<18 years). Among pediatric studies that reported on age and sex, the mean age was 10.2 years66-68,70-81 and 32% were females.66,68,69,71–76,78–80 Among adult studies, the mean age of participants was 22.3 years58–64 and 33.3% were female.58–63
Regarding underlying diagnoses, 6 adult NRS58–60,62–64 and 3 pediatric NRS73,76,81 included participants with drop attacks. LGS was reported in one NRS 61 comprising adults and 7 NRS66,67,69,71,72,75,80 comprising pediatric participants. Three68,74,77 included pediatric participants with West Syndrome and other epileptic encephalopathy syndromes. Four65,70,78,79 did not report underlying diagnoses. The systematic review included all types of callosotomies; however, the included studies did not consistently report outcomes by callosotomy type (anterior, posterior, or complete). Therefore, we report outcomes for all types together.
Detailed study and patient characteristics are provided in Suppemental Table S3.
We judged the included studies to have a critical risk of bias primarily due to the absence of comparison groups and concerns regarding prognostic imbalance (Supplemental Material S6, Supplemental Figure S6).
Below, we report the effects of the interventions by population group for the outcomes considered by the AES/CNS panel as key for decision-making (Tables 6 and 7). Other outcomes considered important but not key, are reported in Supplemental Material S11.
Population 1: Pediatrics
Seizure freedom. Very low-certainty evidence from 3 NRS71,72,78 suggests that complete seizure freedom may occur in 14% (14/102) participants in the short-term (1-year follow-up) and one NRS 75 found that all participants (n = 16) achieved drop-attack freedom also in the short-term (mean follow-up 1.5 years) after undergoing callosotomy.
When compared to VNS, very low-certainty evidence suggest that there may be an increase in seizure freedom (all seizures) at medium-term follow-up (OR 2.18, 95% CI [0.58 to 8.27], RD 82 per 1000, 95% CI [−33 to 346]; n = 3 NRS66,68,69 and 103 participants; 2.5 years follow-up) and in drop-attack freedom (OR 4.26, 95% CI [0.19 to 97.49]; RD 195 per 1000, 95% CI [−66 to 815] more; n = 1 NRS 69 and 17 participants; 2 years follow-up). Additionally, very low-certainty evidence from a single NRS 67 with 31 participants, suggests that there may be little to no difference in seizure freedom (all seizures) at longest follow-up (OR 0.81, 95% CI [0.05 to 14.28]; RD −13 per 1000, 95% CI [−68 to 452]; 5.8 years follow-up).
Serious adverse events. Very low-certainty evidence from one comparative NRS 69 with 24 participants, suggests that, when compared to VNS, there may be little to no difference in unexpected neurological deficits among those undergoing callosotomy at medium-term follow-up (OR 0.72, 95% CI [0.01 to 39.52]; RD −3 per 1000, 95% CI [−10 to 275]; 2 years follow-up). Very low-certainty evidence from 6 NRS,71,74,77–80 however, suggests that permanent, unexpected neurological deficits may occur in 2.7% (5/183) participants at medium-term follow-up (mean follow-up 3 years) after undergoing callosotomy.
With very low-certainty evidence, one NRS 66 with 44 participants, suggests that, when compared to VNS, there may be little to no difference in all-cause mortality among participants undergoing callosotomy at medium-term follow-up (OR 0.84, 95% CI [0.02 to 44.05]; RD −2 per 1000, 95% CI [−10 to 298]; 2 years follow-up). Also, 7 NRS70,71,74,77–80 suggest that medical or surgical complications may occur in 18% (38/211) participants after undergoing callosotomy at short-term follow-up (1 year).
QoL. Very low-certainty evidence from one NRS 66 and 44 participants suggests that when compared to VNS, callosotomy may have little to no effect on QoL (as reported by participants) at medium-term follow-up (OR 0.88, 95% CI [0.17 to 4.51]; RD −17 per 1000 participants, 95% CI [–359 to 112]; 2 years follow-up). However, very low-certainty evidence from 4 NRS59,71,78,79 suggests there may be an improvement in QoL (as reported by participants) in 58% (90/155) participants at medium-term follow-up (4 years) after undergoing callosotomy.
Neuropsychiatric. Very low-certainty evidence from 3 NRS74,77,80 suggests there may be behavior improvement in 63% (41/65) participants at medium-term follow-up (3 years) after undergoing callosotomy.
Other outcomes. We are also very uncertain about the effects of callosotomy on medical or surgical complications (brain infection, intracranial hemorrhage), neuropsychological (developmental status, IQ) and social outcomes (starting education) (Supplemental Material S11).
We did not identify eligible studies reporting on the other prioritized patient-important outcomes including SUDEP, neuropsychological outcomes (verbal memory, naming, verbal fluency, receptive language), or neuropsychiatric outcomes (anxiety, depression, psychosis).
Population 2: Adults
Seizure freedom. We found very low-certainty evidence from a single NRS 58 suggesting that seizure freedom, classified as Rathore I to IV, may occur in 54% (13/24) participants, while drop-attack freedom Rathore Class II may occur in 17% (4/24) participants at short-term (1-year follow-up). Very low-certainty evidence from 2 NRS59,62 suggests that 9% (6/68) participants may achieve complete seizure freedom at medium-term follow-up (mean follow-up 3 years) after undergoing callosotomy. Also, with very low certainty, 2 NRS63,64 suggests that drop-attack freedom may occur in 45% (28/62) participants at the longest follow-up (mean follow-up 9.88 years) after undergoing callosotomy.
Serious adverse events. Very low-certainty evidence from 3 NRS58,59,62 suggests that 3% (3/96) participants may experience permanent, unexpected neurological deficits at medium-term follow-up (mean follow-up 2.97 years). Also, evidence from 3 NRS59,61,62 suggests that 21% (18/87) participants may experience serious adverse events at medium-term follow-up (mean follow-up 3.3 years) after undergoing callosotomy.
QoL. Very low-certainty evidence from 2 NRS59,61 suggests that there may be an improvement in QoL, as reported by participants, in 45% (19/42) participants at medium-term follow-up (mean follow-up 3.3 years), and 2 NRS63,64 suggest there may be an improvement in QoL in 55% (34/62) participants at the longest follow-up (mean follow-up 9.9 years) after undergoing callosotomy.
Other outcomes. We are also very uncertain about the effects of callosotomy on all-cause mortality, medical or surgical complications (brain infection, intracranial hemorrhage), neuropsychological outcomes (verbal fluency, IQ), neuropsychiatric outcomes (personality changes), and social outcomes (work/school, employment) (Supplemental Material S11).
We did not identify eligible studies reporting on the other prioritized patient-important outcomes including SUDEP, neuropsychological outcomes (verbal memory, naming receptive language), neuropsychiatric outcomes (anxiety, depression, psychosis), or social outcomes (driving).
Systematic Review 4: Ablative Surgery Versus Resective Surgery in Patients With HH
We included 15 NRS82–96 comprising 511 participants. Across 14 studies, the mean age was 16.5 years, while one study 85 reported an age range from 5 months to 20 years. Fourteen studies82–92,94–96 reported that 33.4% of participants were female. Five NRS82–86 evaluated LITT and 10 NRS87–96 assessed radiosurgery.
We judged the included studies to be at critical risk of bias primarily due to the absence of comparison groups, prognostic imbalance, and lack of adjustment for important confounders (Supplemental Figure S6, Supplemental Figure S7).
We present below the effects of the interventions by comparison for the outcomes considered by the AES/CNS panel as key for decision-making (Tables 8 and 9). Other outcomes considered important but not key, are reported in Supplemental Material S13.
Comparison 1: LITT Versus Resective Surgery
Seizure freedom. Very low-certainty evidence from 3 pediatric NRS82,83,86 suggests that seizure freedom Engel I may occur in 72% (112/156) participants at short-term follow-up (mean follow-up 1.2 years) after undergoing LITT. Additionally, very low-certainty evidence from one NRS 85 with mixed population, suggests that freedom of gelastic seizures may occur in 93% (66/71) participants at short-term follow-up (1 year) after undergoing MRgLITT.
Serious adverse events. Very low-certainty evidence from 2 pediatric NRS82,83 suggests that serious adverse events may occur in 2% (2/105) of participants at short-term follow-up (mean follow-up 1.2 years) after undergoing LITT. Very low-certainty evidence from 2 NRS83,86 suggests there may be no deaths (n = 109) in participants at short-term follow-up (1 year) after undergoing LITT.
Other outcomes. We are also very uncertain about the effects of LITT on serious adverse events in mixed populations (adults and pediatrics), and medical or surgical complications (pediatrics and mix populations) (Supplemental Material S13).
We did not identify eligible studies reporting on the other prioritized patient-important outcomes including SUDEP, medical or surgical complications (brain infection, intracranial hemorrhage with neurological deficits), neuropsychological outcomes (verbal memory, naming, receptive language, verbal fluency, IQ), neuropsychiatric outcomes (personality changes, depression, anxiety, psychosis), and social outcomes (employment, driving).
Comparison 2: Radiosurgery Versus Resective Surgery
Seizure freedom. In pediatric studies, very low-certainty evidence from a single comparative NRS 88 suggests that, when compared to resective surgery, radiosurgery may reduce seizure freedom Engel I at medium-term follow-up (RD −400 per 1000, 95% CI [−790 to 10]; n = 14; 1.2 years follow-up), while very low-certainty evidence from 2 NRS93,94 suggests that seizure freedom Engel I may occur in 290 per 1000 (n = 34) participants at medium-term follow-up (2 years) after undergoing radiosurgery. In adult studies, very low-certainty evidence from a single comparative NRS, 87 suggests that when compared to resective surgery, radiosurgery may increase seizure freedom Engel I at medium-term follow-up (OR 2.62, 95% CI [0.31 to 21.91]; RD 224 per 1000, 95% CI [−170 to 617]; n = 33; 5 years follow-up).
Serious adverse events. Very low-certainty evidence from a single NRS 87 including adults, suggests that when compared to resective surgery, radiosurgery may reduce permanent, unexpected neurological deficits at medium-term follow-up (RD −30 per 1000, 95% CI [−300 to 240]; n = 36; 5 years follow-up). In pediatric populations, a single NRS, 94 suggests that there may be no permanent, unexpected neurological deficits after radiosurgery (n = 10 participants, mean follow-up 3 years), but we are very uncertain.
For all-cause mortality, very low-certainty evidence from a single NRS 93 comprising pediatric participants (n = 15), suggests there may be no deaths after undergoing radiosurgery at short-term follow-up (1 year). In adult populations, very low-certainty evidence from one NRS 87 suggests that, when compared to resective surgery, radiosurgery may reduce mortality at medium-term follow-up (RD −110 per 1000, 95% CI [−390 to 170]; n = 40; 5 years follow-up). Very low-certainty evidence from a single NRS 90 including mixed populations suggests that SUDEP may not occur after undergoing radiosurgery at the longest follow-up (6 years).
For medical or surgical complications, very low-certainty evidence from one NRS 93 including pediatric participants (n = 15) suggests that brain infection and intracranial hemorrhage may not occur after radiosurgery at short-term follow-up (1 year). In adult populations, very low-certainty evidence from one comparative NRS 87 suggests that, when compared to resective surgery, radiosurgery may reduce brain infection (RD −60 per 1000, 95% CI [−330 to 220]; n = 40; 4.8-year follow-up) and intracranial hemorrhage (RD −170 per 1000, 95% CI [−460 to −120]; n = 40; 4.8 years follow-up) at medium-term follow-up.
We are also very uncertain about the effects of radiosurgery on QoL, neuropsychological outcomes (verbal memory, naming, receptive language, verbal fluency, IQ), and neuropsychiatric outcomes (behavior changes, personality changes) (Supplemental Material S13).
We did not identify eligible studies reporting on the other prioritized patient-important outcomes including social outcomes (driving and employment).
Discussion
Summary of Findings
These 4 systematic reviews synthesized the best available evidence on resective, ablative, and neuromodulation procedures for patients with DRE and informed the AES/CNS guideline on surgical management of DRE. Across all reviews, the certainty of evidence ranged from moderate to very low.
In patients with drug-resistant mesiotemporal lobe epilepsy (DR-MTLE), moderate-certainty evidence showed that ATL, compared with medical therapy, probably increases seizure freedom and improves QoL. Evidence evaluating SAH, LITT, and radiosurgery was limited and of very low certainty.
In DR-NE, very low-certainty evidence suggested that seizure freedom may occur after resective surgery; however, the effects on seizure outcomes, QoL, neuropsychological outcomes, and harms are uncertain. We did not identify studies of sufficient sample size evaluating ablative procedures in this population.
As for DEE with drop attacks, very low-certainty evidence suggested that callosotomy may improve seizure outcomes compared with VNS, although serious adverse events may occur. In HH, evidence for LITT and radiosurgery was also of very low certainty.
Research in Context
Our findings align with several recent systematic reviews evaluating epilepsy surgery in specific populations and procedures, including reviews of minimally invasive approaches for MTLE,97,98 surgery for HH, 99 and callosotomy for DRE drop-attacks. 100 These reviews similarly found that surgical interventions may improve seizure outcomes, 20 although confidence in the evidence remained limited by the predominance of NRS and methodological limitations, as GRADE is not used consistently. To our knowledge, this is the first review synthesizing the comparative effectiveness of epilepsy surgery across different DRE conditions.
Strengths and Limitations
These reviews addressed clinically relevant questions and patient-important outcomes prioritized by the AES/CNS guideline panel. The main strength of these reviews is the methodological rigor, including the use of the GRADE approach to evaluate the certainty of evidence across outcomes.
The main limitations relate to the available evidence rather than the review process itself. Most evidence originated from NRSs at serious or critical risk of bias, frequently affected by unadjusted confounding, lack of comparison groups, and inconsistent outcome measurement and reporting. Many studies included small sample sizes and wide CIs, resulting in serious or very serious imprecision. Heterogeneity across populations, interventions, and follow-up durations also limited pooling and interpretation of findings. Also, studies inconsistently reported patient-important outcomes, particularly social, neuropsychiatric, and long-term quality-of-life outcomes, and insufficient data prevented us from conducting any subgroup analyses.
Implications for Research and Practice
We identified moderate-certainty evidence that suggests that ATL probably increases seizure freedom and improves QoL in patients with DR-MTLE. This finding can help inform practice with higher confidence in the effects of the intervention and further research addressing this question may not be needed. However, for other surgical approaches and epilepsy syndromes that were prioritized by the panel, clinicians may need to interpret the findings cautiously as the evidence base provides very low certainty in the effect estimates. When evidence is of very low certainty, the true effects may differ substantially from the observed estimates. In such situations, decision-making should place greater emphasis on contextual factors beyond the certainty of evidence, including patient values and preferences, acceptability of the intervention, feasibility, resource requirements, availability of local expertise, and equity considerations. Thus, when patients are considering surgical management options for DRE, shared decision-making is necessary.
Future research should prioritize well-designed comparative studies with adjustment for confounding factors, standardized outcome reporting, and longer follow-up. Also, studies should consistently report patient-important outcomes, including QoL, neuropsychological and neuropsychiatric outcomes, and social functioning, across both pediatric and adult populations.
Conclusion
These systematic reviews provide a comprehensive and up-to-date synthesis of the evidence on surgical management strategies for DRE. Moderate-certainty evidence supports ATL for selected patients with drug-resistant mesial temporal lobe epilepsy. For other surgical approaches and epilepsy syndromes, the evidence remains predominantly of very low certainty, limiting confidence in estimates across patient-important outcomes.
Given the substantial uncertainty in the available evidence, clinicians and patients should integrate patient values and preferences, feasibility, acceptability, resource use, and local expertise into shared decision-making regarding the surgical management of DRE. High-quality comparative studies with standardized reporting of patient-important outcomes are needed to better inform future guideline recommendations and clinical practice.
Supplemental Material
sj-pdf-1-epi-10.1177_15357597261459808 - Supplemental material for Surgical Management in Patients With Drug-Resistant Epilepsy: A Summary of Four Systematic Reviews and Meta-Analyses
Supplemental material, sj-pdf-1-epi-10.1177_15357597261459808 for Surgical Management in Patients With Drug-Resistant Epilepsy: A Summary of Four Systematic Reviews and Meta-Analyses by Yetiani Roldan, Barbara C. Jobst, Daniela Garcia-Aquino, Dina Ghandour, Mei Bou Nasif, Taylor Duda, Alexandra Eid, Shannon Hart, Mohamad Kesserwan, Amanda Martyniuk, Melissa Lannon, Golbarg Saber, Christopher Saouda, Sunjay Sharma, Victoria Vinarsky, Shawna L. Strickland, Robyn M. Busch, Jennifer L. Hopp, Jorge Gonzalez-Martinez, Gregory Bergey and Andrea J. Darzi in Epilepsy Currents
Footnotes
Abbreviations
Acknowledgments
We thank Alexandria Brackett for the deveolpment of the initial search strategy, Kaitryn Campbell for her assistance in developing and refining the literature search strategies, and Julie L. Higham from the GUIDE Group for her support with guideline management and coordination activities. We also thank the members of the AES and CNS guideline panel for their clinical expertise and input during the guideline process that these systematic reviews were designed to inform. We would specifically like to acknowledge David Bauer, Angela Price, James L. Bernat, Pete Engel, Satya Gedela, David Gloss, Aatif M. Husain, Robert A. McGovern, Guy McKhann, Douglas R. Nordli Jr., John D. Rolston, Richard Shane, Dennis Spencer, and Howard L. Weiner for their contributions to the guideline panel discussions and review process.
Author Contributions
Yetiani Roldan: conceptualization, methodology, investigation, formal analysis, data curation, project administration, visualization, writing—original draft, and writing—review and editing; Barbara C. Jobst: conceptualization, supervision, and writing—review and editing; Daniela Garcia-Aquino: investigation, data curation, and writing—review and editing; Dina Ghandour: investigation, data curation, and writing—review and editing; Mei Bou Nasif: investigation, data curation, and writing—review and editing; Taylor Duda: methodology, formal analysis, and writing—review and editing; Alexandra Eid: investigation, data curation, and writing—review and editing; Shannon Hart: investigation, data curation, and writing—review and editing; Mohamad Kesserwan: investigation, data curation, and writing—review and editing; Amanda Martyniuk: investigation, data curation, and writing—review and editing; Melissa Lannon: investigation, data curation, and writing—review and editing; Golbarg Saber: investigation, data curation, and writing—review and editing; Christopher Saouda: investigation, data curation, and writing—review and editing; Sunjay Sharma: investigation, data curation, and writing—review and editing; Victoria Vinarsky: investigation, data curation, and writing—review and editing; Shawna L. Strickland: writing—review and editing; Jennifer L. Hopp: conceptualization and writing—review and editing; Robyn M. Busch: conceptualization and writing—review and editing; Jorge Gonzalez-Martinez: conceptualization, supervision, and writing—review and editing; Gregory Bergey: conceptualization, supervision, writing—review and editing; Andrea J. Darzi: conceptualization, methodology, investigation, visualization, formal analysis, supervision, and writing—review and editing.
All authors reviewed and approved the final article. YR and AJD had full access to the data for these reviews. YR and AJD shared the decision to submit for publication with BCJ, JG-M, and GB.
Data Availability
For original data, please contact the corresponding author Yetiani Roldan (roldany@mcmaster.ca). For statistical analyses and additional data, please refer to the online supplemental material.
Declaration of Conflicting Interests
The following authors declared these potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The methods team—YR, DG-A, DG, MBN, AE, AH, MK, AM, VV, ML, GS, CS, SJ, and AJD—declare no financial or intellectual conflicts of interest. Authors who also served as panel members for the surgical epilepsy guideline—BCJ, JG-M, GB, JLH, and RMB—disclosed all potential conflicts of interest in accordance with the AES conflict of interest management policy as part of the guideline development process. The following authors declared these potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Elsevier Publishing (GB, RMB), Up To Date Inc. (JLH), NEUROPACE, Inc (BCJ). SLS declares no financial or intellectual conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was commissioned and funded by the AES as part of work to inform upcoming epilepsy surgery guidelines. The funder contributed to defining the scope of the review, and writing the protocol, but otherwise had no role in the study design, data collection, data synthesis, or data interpretation.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.