
Abstract
Sullivan J, Valente K, Villanueva V, Strzelczyk A, Nabbout R, Nakagawa E, Zhang Y, Zolnowska M, Khan Y, Dong C, Hsiao S, Sheikh SI, von Rosenstiel P, Asgharnejad M, Murthy V. Epilepsia. 2026 Mar 5. doi: 10.1002/epi.70164. Epub ahead of print. PMID: 41784472. Objective: This study evaluated the efficacy, safety, and tolerability of soticlestat as adjunctive therapy in children and young adults with Dravet syndrome (DS). Methods: SKYLINE (NCT04940624) was a multicenter, randomized, double-blind, placebo-controlled, phase 3 trial that enrolled patients with DS aged 2–21 years with uncontrolled convulsive seizures (≥4/month despite adequate treatment). Participants received oral soticlestat 300 mg (weight adjusted) or matching placebo twice daily. The total study duration was 16 weeks, comprising 4-week dose titration and 12-week maintenance treatment periods. The primary endpoint was a comparison of monthly convulsive seizure frequency between baseline and the titration/maintenance periods. Key secondary endpoints included several modified Caregiver and Clinical Global Impression of Improvement (GI-I) scales for DS. Results: One hundred forty-four participants were randomized (71 placebo, 73 soticlestat) with a mean (SD) age of 10.3 (5.0) years; 72 (50%) were male, and 117 (81.3%) were receiving ≥3 antiseizure medications. Median change from baseline in convulsive seizure frequency over the full treatment period was −8.64% with placebo (n = 71) and −22.16% with soticlestat (n = 73), a difference of −15.64% (p = .061); in the maintenance treatment period, these changes were −11.99% with placebo and −23.29% with soticlestat, a difference of −14.29% (p = .089). The proportion of participants with ≥50% reduction in convulsive seizures was 9.9% with placebo and 27.4% with soticlestat (nominal p = .008). Soticlestat showed clinically meaningful results in the Caregiver and Clinical GI-I, and Clinical GI-I Seizure Intensity and Duration scales over the 16-week treatment period (all nominal p-values ≤ .004). The most commonly reported treatment-emergent adverse events related to study drug were somnolence, change in seizure presentation, decreased appetite, and insomnia. Significance: Although statistical significance was narrowly missed, soticlestat showed a numerical benefit over placebo for convulsive seizure decrease. Clinically meaningful benefits across multiple secondary endpoints were observed. No new safety concerns emerged.
Commentary
At least 85% of individuals with Dravet syndrome (DS), a developmental and epileptic encephalopathy (DEE), share high genetic risk factor homogeneity due to a pathogenic variant in SCN1A. DS accounts for roughly 1:15,000–1:40,000 epilepsy cases. 1 DS has a well-defined clinical course and high seizure burden (often with high treatment resistance), facilitating predictable clinical trial design. Furthermore, as a largely monogenic epilepsy, intense investigation on the genetic basis of DS has led several groups to produce mouse Scn1a variant models that recapitulate many clinical DS features, including spontaneous recurrent seizures (SRSs), heat-induced seizures, and significant premature mortality akin to clinical sudden unexpected death in epilepsy (SUDEP2,3). Accordingly, Scn1a+/− DS models have become an invaluable precision medicine discovery tool in recent years.
Brain cholesterol biosynthesis regulates a variety of distinctly critical neurological pathways. Neurons process and maintain cholesterol homeostasis. However, cholesterol does not readily pass the blood–brain barrier, thus neurons predominantly rely on de novo cholesterol synthesis within astrocytes for normal function. 4 Cholesterol is a critical component of synaptic membranes, modulating the localization and function of ion channels, receptors, and signaling complexes, thereby shaping both excitatory and inhibitory neurotransmission. The major cholesterol degradation product in the adult brain is a side-chain oxidation product, 24-OHC, which is produced by the neuron-specific cytochrome P450 enzyme CYP46A1 (aka, cholesterol 24-hydroxylase [CH24H]). CYP46A1 hydroxylation accounts for 75%–85% of brain cholesterol catabolism and turnover. Dysregulation of brain cholesterol has been implicated in diseases such as Alzheimer's, Parkinson's, Huntington's, and even epilepsy. Sufficient brain cholesterol concentration is critical to normal neuronal function such that inhibiting brain cholesterol catabolism is a rational therapeutic target for a variety of neurological diseases.
Given this unique neuron-specific biochemical pathway and brain-specific cytochrome P450 enzyme involved in critical neuronal homeostasis, soticlestat (SOT) was developed as a first-in-class CYP46A1 (CH24H) inhibitor for epilepsy.5,6 Sullivan et al 7 report the late-stage Phase III clinical trial results with SOT use in DS. In the preceding Phase II trial, SOT showed statistically significant, clinically meaningful reductions from baseline in median seizure frequency in DEE patients. 8 However, in the ensuing Phase III trial, SOT outcomes across all DS patients over the full treatment period barely missed the primary endpoint of conferring a statistically significant reduction in the median change from baseline convulsive seizure frequency (p = .061). However, SCN1A + DS patients showed statistically significant reductions in seizure frequency. Sullivan et al 7 report that specifically in SCN1A + DS carriers, the difference in median reduction in convulsive seizure frequency per 28 days between the SOT and placebo treatment groups was 17.38% (p = .045), whereas in DS patients without an SCN1A variant, the difference was just 3.01% (p = .713). Thus, this subgroup secondary analysis reveals that SOT was beneficial solely in SCN1A + DS patients.
While this Phase III trial failed to demonstrate significant benefit in all trial participants, 7 it reveals a critical preclinical epilepsy therapy development milestone. First, while the role of CH24H in epilepsy has not yet attracted widespread attention, the preclinical profile of SOT is unique and provides compelling predictive evidence to inform future clinical trials. SOT exhibits robust anticonvulsant activity and disease-modifying potential in a Scn1a haploinsufficient DS mouse model, 9 as well as other mouse acquired seizure models. 10 Second, SOT displays a preclinical profile that is distinctly unique from all other Food and Drug Administration-approved antiseizure medicines (ASMs; Table 1). 5 Whereas SOT exerts anticonvulsant efficacy in several well-characterized rodent epilepsy models defined by SRS and a “true” epilepsy phenotype, 5 SOT is entirely ineffective in the “traditional” acutely evoked screening models, such as MES, scPTZ, and 6 Hz, which have defined the ASM discovery landscape for decades (Table 1). 5 Furthermore, SOT does not block the acutely evoked established corneal kindled seizure, but does delay corneal kindling acquisition, reflecting a unique disease-modifying profile (Table 1). This present Phase III clinical failure with SOT in a DS patient population should, thus, be taken as clear evidence that Scn1a haploinsufficient DS mice specifically represent a predictive preclinical model well-suited to next-generation ASM discovery.
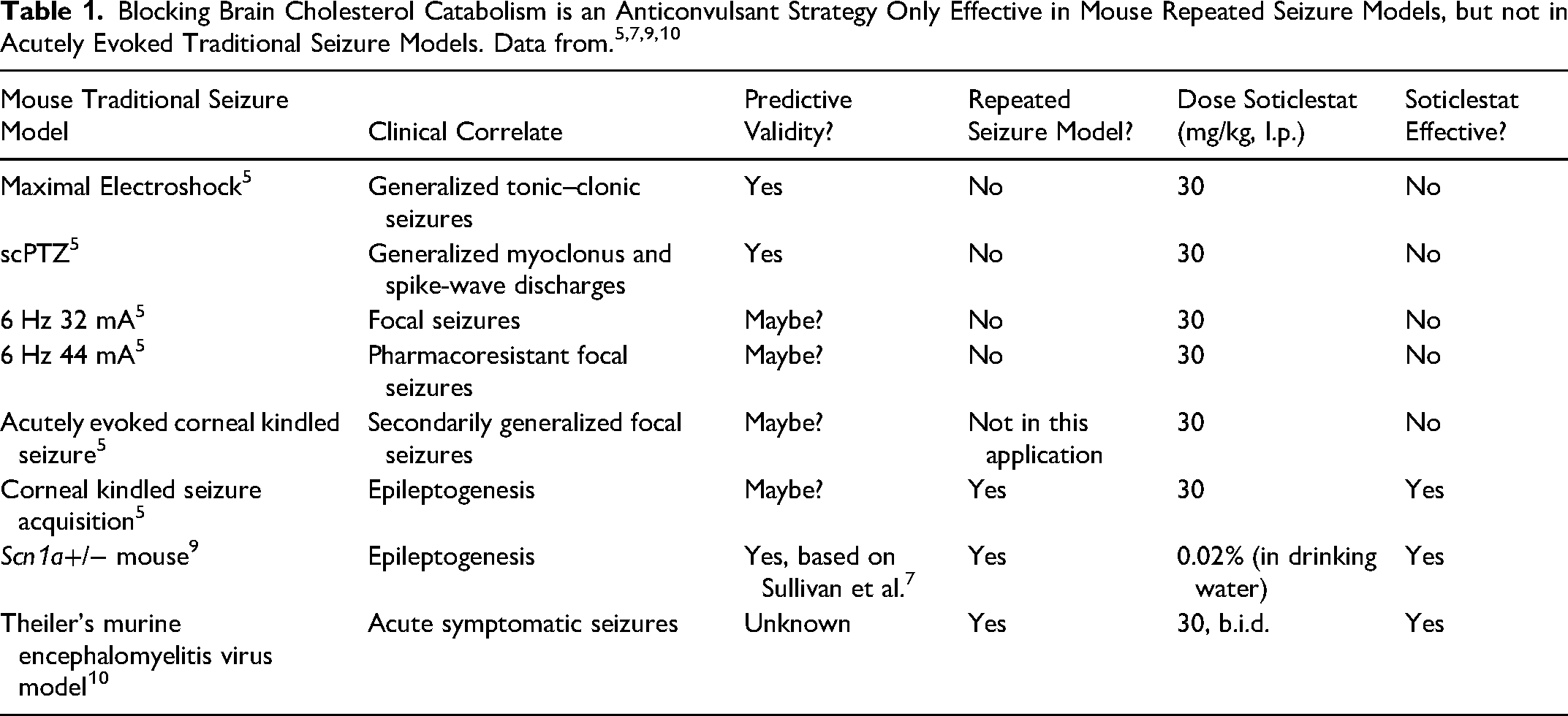
The “traditional” screening models (MES, scPTZ, amygdala kindling, and WAG/Rij/GAERS) represent the four highly predictive and clinically “validated” screening models. 10 One interesting hypothesis and outcome of the SOT clinical trial failure 7 is therefore that the Scn1a+/− DS mouse now represents a “fifth” clinically validated preclinical screening model. Importantly, multiple Scn1a models have provided foundational insight into the anticonvulsant and disease-modifying potential of already approved DS therapies, including cannabidiol (CBD) and fenfluramine (FFA). 10 The Phase III trial with SOT now reveals that the Scn1a+/− DS models are also particularly beneficial to identify impactful disease-modifying compounds, which distinctly differentiates DS models from “traditional” acute seizure induction models, such as MES, scPTZ, 6 Hz and acutely evoked corneal kindling (Table 1). 10 Notably, these other ASMs approved for DS (FFA and CBD) share interesting similarities in that both are effective in “traditional” rodent acute seizure models (MES, scPTZ, and kindling). Thus, unlike in the case of SOT, these traditional seizure models could have just as easily identified CBD and FFA. However, SOT does not work in these acute seizure paradigms (Table 1). As such, efficacy in Scn1a+/− DS models is a consistent feature for all three therapies, whereas there is differentiation in their efficacy in “traditional” screening models. In this way, SOT's preclinical profile bears some similarities to levetiracetam in its preclinical activity in “traditional” screening models, 10 albeit levetiracetam is effective in 6 Hz and kindling models, but provides the compelling justification that future ASM discovery efforts should increasingly integrate DS models. Whether other mouse monogenic epilepsy models can similarly successfully inform the preclinical to clinical translational progression herein observed with SOT remains to be established. However, this clinical failure altogether highlights a compelling potential clinical development strategy for treatment-resistant monogenic epilepsies.
Modern ASM discovery has been shaped by several critical inflection points. While “traditional” rodent acute seizure models (MES and scPTZ) have been indispensable to the identification of numerous therapies over many decades, the present clinical findings of meaningful seizure frequency reductions with SOT in SCN1A + DS patients provide paradigm-shifting evidence establishing the predictive validity of the Scn1a+/− mouse.9,10 The field must now move to increasingly rely on this and other syndrome-specific models in early ASM discovery. Continued reliance solely on traditional acute seizure models would represent a major missed opportunity that could negatively hamper future patient outcomes. This clinical trial failure 7 provides the definitive preclinical evidence that the underlying neurobiology in discrete treatment-resistant monogenic epilepsies is likely to uncover future clinically meaningful compounds.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.