
Abstract
Mary G. Jessome, Kimberly R. Huyser, Tom Einhorn, Tamara Chavez, Nicole Dawydiuk, Katherine A. Collins, and Michelle Johnson-Jennings on indigenous cultural practices and vaccine uptake.
Needles do more than play an integral role in the administration of vaccines: They stitch identity into the lives of Indigenous Peoples across Turtle Island (a term some Indigenous people use for the continent of North America, encompassing both Canada and the United States). The complex role of needles in promoting health and culture is exemplified by Indigenous participation in beadwork during the SARS-CoV-2 (COVID-19) pandemic. In 2021, roughly 18 percent of Indigenous people living on Turtle Island reported participating in beadwork. As Rhiannon Johnson explained in her 2020 article for the Canadian Broadcasting Corporation, “Traditional Crafters Indigenizing Face Masks during the COVID-19 Pandemic,” beadwork provided a way for some Indigenous people to connect with Indigenous culture during the pandemic by integrating traditional practices, designs, and materials like cedar and spruce needles into the masks they created. Through this work, they drew on culture as a source of resilience and flourishing. Beadwork linked Indigenous people to the Original Instructions that provide lessons on how to live in a state of respectful interdependence with the Earth, ancestral practices, and traditional territories amid ongoing challenges caused by intergenerational trauma, anti-Indigenous racism, and other life stressors.
Given its benefits, how can culture be used to address major health concerns among Indigenous Peoples? Do certain cultural practices relate differently to particular health behaviors among them? In this article, we begin to answer these questions by describing how participation in cultural activities relates to vaccination uptake among Indigenous people in the United States and Canada. Immunization is associated with risks ranging from fever to the development of autoimmune conditions, depending on the vaccination being administered. Health care providers and patients must always navigate the risks associated with vaccination. However, this risk–benefit analysis is complicated by immunizations becoming an increasingly politicized topic. In a 2025 JMIR Research Protocols article, Nazeem Muhajarine and his co-authors demonstrated that growing mistrust in government, public health, and the broader scientific enterprise created environments in which people were hesitant to get vaccinated. Building trust around vaccination risks is particularly urgent for Indigenous Peoples. Historical and ongoing anti-Indigenous racism and abuse by medical and governmental organizations exacerbate mistrust and pose significant barriers to vaccine uptake among these populations. As outlined by Mary Ellen Turpel-Lafond in a report titled “In Plain Sight: Addressing Indigenous-specific Racism and Discrimination in B.C. Health Care,” anti-Indigenous racism and abuse manifest through stereotyping and discrimination, which restrict access to care and contribute to poorer health outcomes among Indigenous Peoples.
As detailed in the Collective for Indigenous Engagement, Development, and Research’s 2021 Hearing Indigenous Voices Survey report, our data comes from the 2021 Hearing Indigenous Voices Survey (HIS). The HIS is a cross-sectional survey based on a convenience sample of Indigenous people living in the United States and Canada. We measured engagement in cultural activities using a question that asked respondents to report their participation in 19 cultural activities. We found that of 557 Indigenous respondents, 81 percent participated in at least one of the cultural activities. Socializing with other Indigenous people was the most frequently selected activity (47 percent). This was followed by eating or cooking Indigenous food (40 percent), attending powwows or other social gatherings (33 percent), knowing and sharing Indigenous history (32 percent), attending Indigenous ceremonies (28 percent), and hunting, fishing, or trapping (28 percent). Those who participated in at least one activity reported taking part in an average of four activities.
Socioeconomic and COVID-19-specific barriers likely shaped participation in the cultural activities listed above. As Claudie Péloquin and co-authors discussed in their 2017 article in the International Journal of Environmental Research and Public Health, barriers take many forms. They include financial constraints, lack of time, unsafe environments due to anti-Indigenous racism, and higher rates of illness and disease among Indigenous Peoples. For example, American Indians and Alaska Native men were 3.4 times more likely to die of chronic liver disease or cirrhosis than non-Hispanic white males.
COVID-19 also came with a unique set of challenges. As Mary G. Jessome and her collaborators explained in their 2025 article in the Journal of Primary Care and Community Health, public health policies, such as social distancing measures, made cultural activities involving large social gatherings (e.g., ceremonial sweats) less accessible for many Indigenous Peoples. The pandemic also worsened many pre-existing socioeconomic inequities, amplifying economic hardship among Indigenous communities. Thus, it is likely that financial barriers to cultural participation intensified during this period.
These barriers provide a possible explanation for why HIS respondents socialized with other Indigenous individuals and ate and cooked Indigenous foods at a higher rate than the other cultural practices (see Figure 1). Not only were these activities highly accessible before COVID-19, but they also remained relatively easy to access and integrate into daily living during the pandemic. In contrast to larger community events, socializing with other Indigenous individuals and cooking Indigenous foods were more compatible with social distancing requirements because these activities can be sustained with fewer people and take place in private homes (cooking) or outdoors (socializing). This is likely why, even among the top six cultural activities that Indigenous Peoples engaged in, these practices led by 14 and 7 percentage points, respectively.
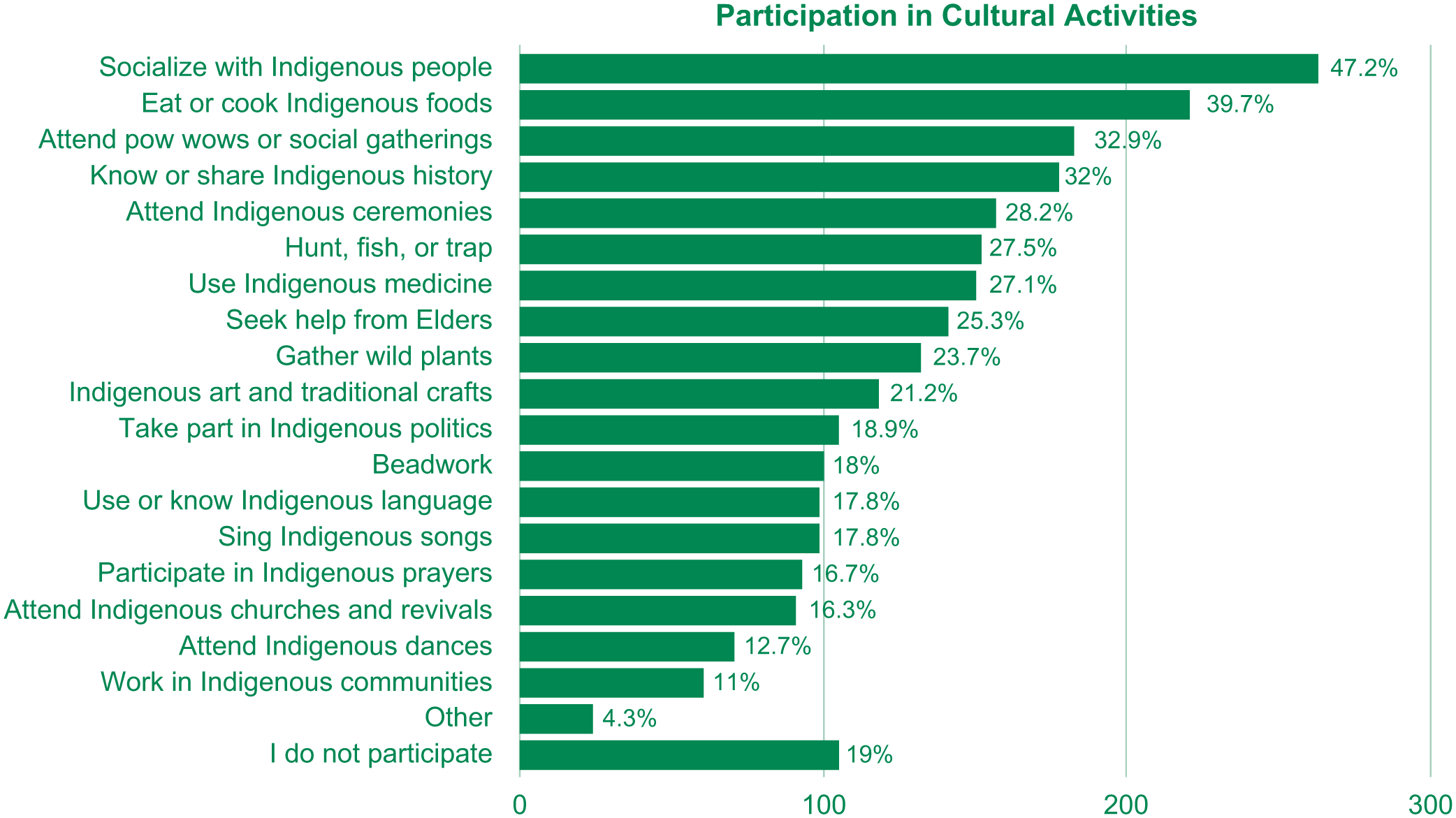
Indigenous Peoples’ Rate of Participation in Cultural Activities.
To understand how participation in various cultural activities is associated with vaccine uptake, we grouped the original list of practices into three clusters. The first group clustered large social gatherings, including attending ceremonies and powwows, seeking advice from Elders, and participating in other celebrations. The second group included activities such as hunting, gathering, and eating Indigenous foods. The third incorporated categories related to arts and crafts, as well as knowing and sharing Indigenous histories. Some respondents engaged in activities across multiple groups, while others, as discussed above, did not engage in any of them.
We used the three cultural activities cluster variables, along with other social and demographic indicators, to model whether a person had received at least one dose of the COVID-19 vaccine at the time of the survey. COVID-19 vaccines had been available to the adult population for roughly 18 months in both Canada and the United States at the time of data collection. Seventy-one percent of HIS respondents reported receiving at least one dose of a COVID-19 vaccine. Vaccination rates were significantly higher among Indigenous residents of Canada (84 percent) compared to residents of the United States (59 percent). We hypothesized that these differences were related to divergent national healthcare systems, varying levels of vaccine access, and differing attitudes regarding vaccination on either side of the border.
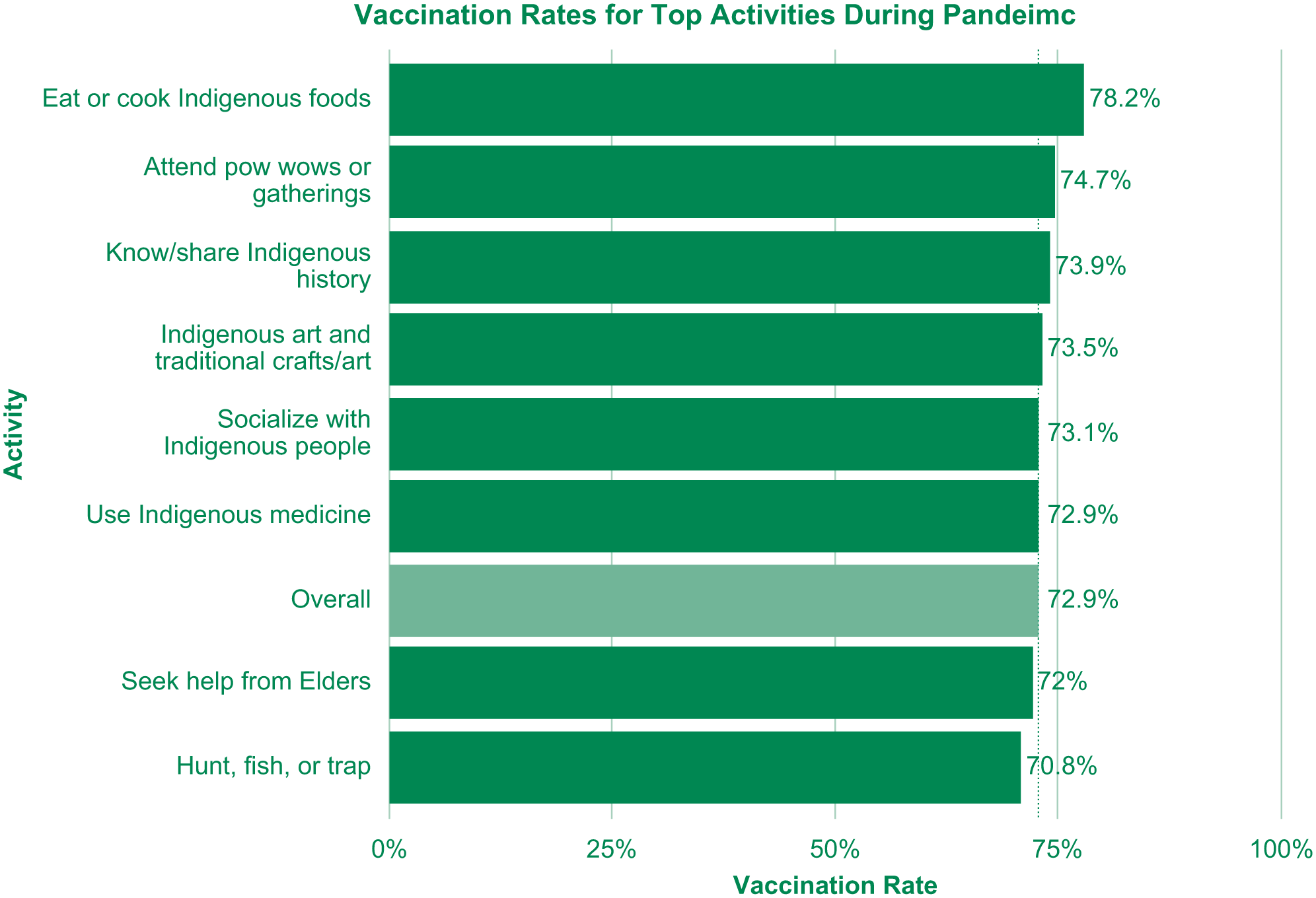
Vaccination Rates by Cultural Activities.
We accounted for social and demographic factors by adding measures of age, level of education, financial means, essential worker status, trust in public health mandates, trust in COVID-19 vaccinations, social media use, racialization (operationalized as whether one believes one is identified by others as Indigenous while walking down the street), and whether respondents were diagnosed with any chronic illness. (“Racialization” is the process by which someone is assumed to belong to a particular racial or ethnic group based on how they look.)
We found that age, education, financial means, two cultural activities clusters, and chronic illness were not related to whether a respondent had received at least one dose of the COVID-19 vaccine. However, racialization (being perceived as Indigenous), trust in vaccinations, trust in other public health mandates, social media use, and essential worker status had statistically significant relationships with vaccination. Notably, we found that respondents who reported that they were “never” or “not often” perceived as Indigenous were 2.5 times more likely to report having been vaccinated than those who reported that they were “sometimes” or “always” perceived as being Indigenous. This suggests that people who are frequently recognized as Indigenous may have avoided healthcare settings during COVID-19 as a way of escaping the racism that Indigenous individuals continue to face.
Greater trust in the safety and effectiveness of vaccines, as well as in public health measures, also increased the likelihood of vaccination. Specifically, trust in public health mandates was associated with double the likelihood of vaccination and trust in the safety and efficacy of vaccines was associated with about two-and-a-half times the likelihood. Additionally, using social media to get news about the pandemic reduced the odds by roughly one-third. The significance of trust in the COVID-19 vaccine and broader public health measures as a predictor of immunization is not surprising given past research on the topic. As Bipin Adhikari and colleagues wrote in their 2022 article in Vaccine: X, “trust is a fundamental element of acceptance of public health interventions. . . .” This includes, of course, vaccine uptake. Finally, and perhaps expectedly, respondents who were classified as essential workers during the pandemic were nearly twice as likely to be vaccinated.
Participation in cultural activities was also a statistically significant predictor of vaccination. Specifically, respondents who reported participating in beading, other traditional arts and crafts, and knowing and sharing Indigenous history had almost four times the odds of being vaccinated compared to those who did not report engaging in these activities.
Integrating cultural traditions into public health initiatives could facilitate vaccination uptake among Indigenous Peoples, ensuring they continue to thrive as anti-vaccination sentiments grow.
While the HIS data is only a convenience sample and does not provide the information necessary to identify why certain variables are associated with vaccination, a few relationships warrant further investigation. The insignificance of demographic and health variables like age, education, and chronic illness suggests that the intersection of public health policy and culture more strongly informed COVID-19 vaccination behaviors among Indigenous people. This finding contrasts with findings from non-emergency situations, where health status, resources, and background more directly inform behaviors, particularly among those with ongoing health concerns.
Cultural belonging is positively correlated with health as it strengthens Indigenous identity by providing a sense of belonging. However, Indigenous culture is not uniform: It is composed of practices and beliefs that benefit different dimensions of Indigenous health across settings. The patterns observed may reflect barriers confronted by Indigenous people during COVID-19 due to public health policies like social distancing. When large gatherings were not feasible during the pandemic, traditional arts and crafts could be done individually or were made accessible for groups online. As such, they might have served as a safe way of ensuring that community members remained connected, collectively engaging in the traditional beliefs and practices that they need to be well.
Culture alone cannot ensure positive health behaviors among Indigenous Peoples. Yet as political tides and public resources allocated to vaccination change, cultural activities continue to connect Indigenous Peoples to teachings, practices, and identity. Integrating cultural traditions into public health initiatives could facilitate vaccination uptake among Indigenous Peoples, ensuring they continue to thrive as anti-vaccination sentiments grow.