
Abstract
Given the need for Latinx/a/o health care providers in the United States, understanding how students choose these fields is critical to achieving more equitable systems. This study uses community cultural wealth to investigate how Latina first-generation college students choose and pursue health care careers. Findings show that women employed multiple sources of capital to learn about career options, challenge inequalities in health systems, and to give back to family, especially to honor past and future generations of women.
Within the United States, Latinx/a/o 1 populations experience limited access to quality health care (Shavers et al., 2012; U.S. Department of Health and Human Services [HHS], 2018). This issue is systemic; the U.S. health care workforce lacks diversity (American Association of Medical Colleges [AAMC], 2019), and Latinx/a/o patients often face race-based prejudice and limited cultural competency among providers (Shavers et al., 2012; Terlizzi et al., 2019). Fewer than 6% of physicians in the United States are Hispanic (AAMC, 2019), with Hispanic and Latinx/a/o professionals similarly underrepresented in physician assistant (PA; 3%; Smith & Jacobson, 2016), nurse practitioner (NP; 3%; Chattopadhyay et al., 2015), and nursing (10%; Smiley et al., 2021) careers. Despite underrepresentation, the majority of Latinx/a/o adults report that it is important to have a health provider who shares or understands their culture (Terlizzi et al., 2019). As increasing numbers of Latinx/a/o students participate in U.S. higher education (National Center for Education Statistics, 2020), there is opportunity for education systems to better facilitate Latinx/a/o students’ interest, entry, and success into health programs and professions.
A growing body of research has explored the unique college and career development experiences of Latinx/a/o college students today (e.g., Chavira et al., 2016; Rios-Aguilar & Kiyama, 2012). Studies have also begun to investigate these experiences among Latinx/a/o students based on other intersecting identities as well, including gender (Gomez et al., 2001; Risco & Duffy, 2011; Rodriguez & Blaney, 2020; San Miguel & Kim, 2015; Sy & Romero, 2008); parental education (Moreno, 2021; Sánchez-Connally, 2018; Torres, 2004), and scientific discipline or occupational area (Johanssona et al., 2020; Loftin et al., 2012; Rincón & Rodriguez, 2021; Rivera-Goba & Nieto, 2007; Sparks et al., 2021; Zell, 2014).
Purpose of the Study
Given the need for Latinx/a/o health care professionals and the role of gender and parental education in influencing student academic and career experiences, this study focuses on the career development of Latina students who are the first in their families to pursue bachelor’s degrees (“first-generation students”). Using Yosso’s (2005) community cultural wealth (CCW) model, this phenomenological study explores how six Latina students employ multiple sources of capital to pursue and sustain their professional interests in nursing, NP, PA, and physician careers, asking: What forms of CCW do Latina undergraduate students employ in choosing and pursuing careers in health and medicine?
Latinx/a/o Student Career Development
Across research on Latinx/a/o student career development, family, community, and culture are consistently identified as critical in shaping students’ academic and professional values and goals, and in providing support and encouragement to promote their success, especially during difficult times (Chavira et al., 2016; Gomez et al., 2001; Johanssona et al., 2020; Moreno, 2021; Rios-Aguilar & Kiyama, 2012; Rivera-Goba & Nieto, 2007; Sy & Romero, 2008; Yosso, 2005). However, these same constructs are often absent from predominant career development models for college students, generating the need for research focusing on the career-related experiences, decisions, and development of Latinx/a/o students.
Although family and community often provide critical support to Latinx/a/o student career development processes, differences between students’ personal goals and cultural and familial expectations may also present challenges for Latinx/a/o students in the United States. Latinx/a/o students from families less acculturated to White society (Torres, 2004), who are the first in their families to attend college (Moreno, 2021), or who are from immigrant families (Chavira et al., 2016; Rios-Aguilar & Kiyama, 2012) may experience guilt associated with college participation, especially if they move away from home to attend. These students may also experience pressure to choose high-status or high-paying careers that would make their families proud and that would result in better economic opportunity than their parents had, especially if their parents immigrated to the United States for this purpose (Chavira et al., 2016; Rios-Aguilar & Kiyama, 2012).
Latina Women Students’ Career Development
For Latina women, the intersection of gender and ethnic or racial identity (and, in this study, first-generation college student identity) may additionally affect career decisions. Women’s work has been historically undervalued in U.S. society, with women tracked toward stereotypically feminine domains (e.g., caregivers) and excluded from economically and socially prestigious positions (Acker, 2006; Goldin, 2014). This dynamic can be observed across sectors, including health and medicine. Women—especially women of color—are underrepresented in the highest paying and most respected clinical and academic positions in medicine, such as surgeons or professors, and within positions of leadership (AAMC, 2019; Butkus et al., 2019).
Given the gendered context of many work and family structures, women may be more likely than men to navigate conflicts between personal goals and familial expectations, especially in contexts that uphold traditional gender roles. Latina college students often contribute to taking care of younger siblings and cousins and helping in the family home (Loftin et al., 2012; Sy & Romero, 2008; Torres, 2004). As a result, the expectation (and desire) of Latina students to help family may affect women’s ability to leave home for college or to pursue high-status careers, even when men family members receive support to do so (Gomez et al., 2001). In a study comparing Latinx/a/o men and women, Risco and Duffy (2011) found that women viewed career as a less salient part of their identity than men, often choosing careers based on personal interest and a drive to make a difference, while men emphasized choice, earnings, and autonomy.
Over time, the number of Latina women in college has increased, including those studying science and health fields (National Science Foundation, 2021). Latina students in science and health often see themselves as “trailblazers,” paving a pathway for Latinx/a/o students of the next generation (San Miguel & Kim, 2015). Latina women in science and health may also encounter racism and sexism and feel marginalized and isolated due to the underrepresentation of women—especially Latina women—in these settings (Johanssona et al., 2020; Rivera-Goba & Nieto, 2007; Rodriguez & Blaney, 2020; San Miguel & Kim, 2015). However, research consistently shows Latina women’s resilience and success in achieving their goals by finding mentors, joining student organizations, and forming informal networks in their field (Johanssona et al., 2020; Loftin et al., 2012; Rivera-Goba & Nieto, 2007; Rodriguez & Blaney, 2020; San Miguel & Kim, 2015; Sparks et al., 2021). Such resources may be critical for Latina first-generation students, many of whom depend on non-related adults and other information sources to navigate postsecondary and professional systems in health fields (Johanssona et al., 2020). Given their minoritization within these fields, Latina women are also often driven by the opportunity to prove themselves and to actively denounce racist and sexist stereotypes (Johanssona et al., 2020; Loftin et al., 2012; San Miguel & Kim, 2015).
Community Cultural Wealth
Yosso’s (2005) CCW serves as the theoretical framework for this study. In CCW, Yosso acknowledged the deficit framing of Bordieuan conceptualizations of cultural capital defined by dominant groups of society. Instead, Yosso used principles from critical race theory and funds of knowledge to form an asset-based model identifying of six forms of cultural wealth that racially minoritized students bring into education systems: aspirational, navigational, social, linguistic, familial, and resistant (Table 1).
Forms of Capital in Yosso’s (2005) Theory of Community Cultural Wealth.
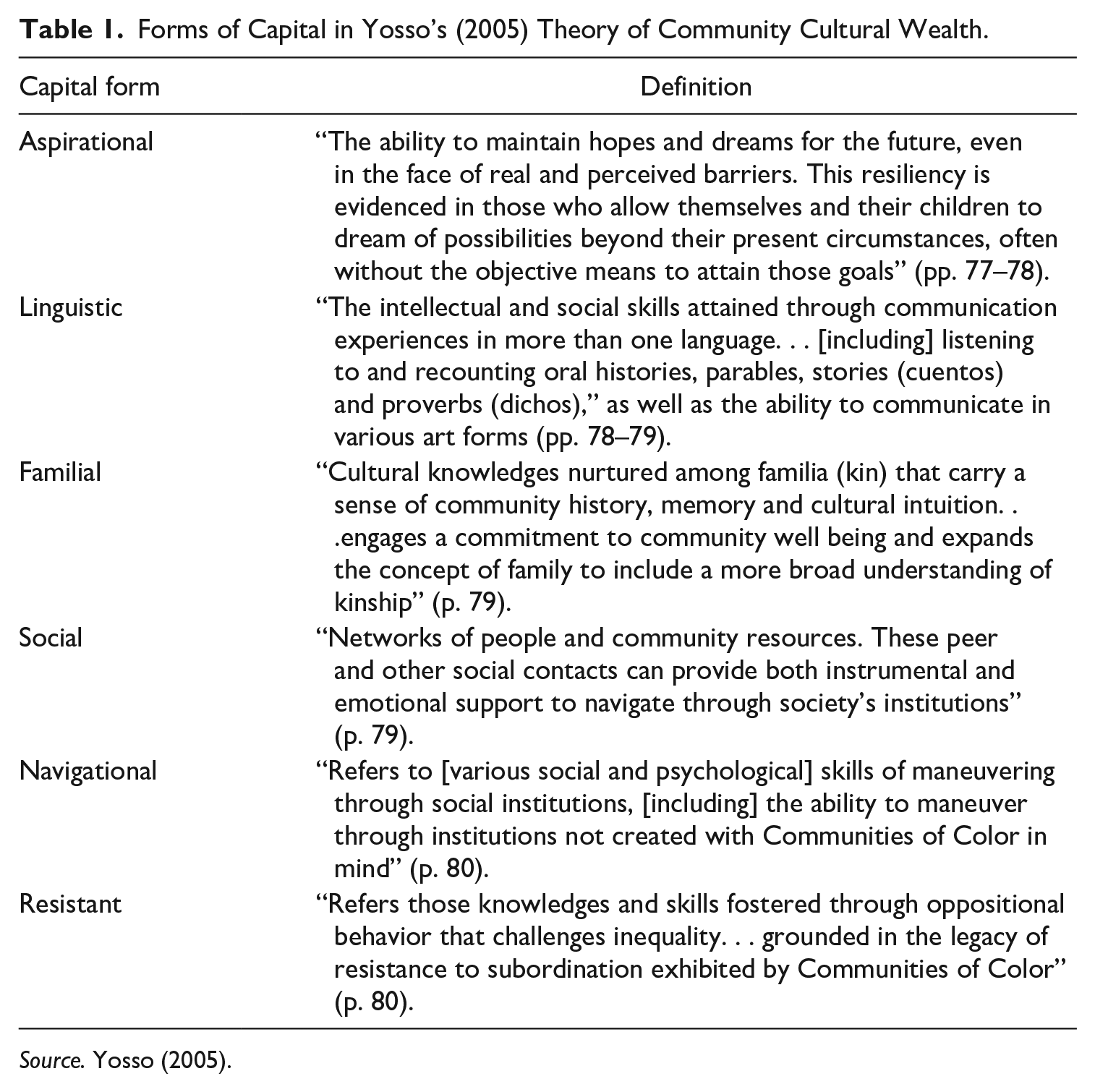
Source. Yosso (2005).
CCW frames a number of studies on Latinx/a/o college student experiences and career development. For example, Sánchez-Connally (2018) found that Latinx/a/o first-generation college students employed social capital to create support networks on their campuses and aspirational and resistant capital to sustain motivation. Rincón and Rodriguez (2021) found that undergraduate Latinx/a/o STEM (science, technology, engineering, and math) students used all six forms of capital to develop a culturally grounded STEM identity and persist in these fields. Zell (2014) found that Latinx/a/o health graduate students used multiple sources of capital to create congruence between their values and behaviors, develop and sustain career goals, build networks, use bilingualism and biculturalism to secure opportunities, see their success as a family endeavor, and disseminate knowledge to other Latinx/a/o students.
Method
This study is derived from a larger phenomenological study on first-generation college students. Phenomenology is a methodology used to understand and portray “meanings and essences” (Moustakas, 1994, p. 84) of a specific phenomenon by gathering comprehensive accounts of participant experiences. After data collection for the original study, I was struck by a subsample of participants; six of the seven Latina women who participated in the larger study aspired to careers in health care or medicine. Given this distribution and the societal need for Latinx/a/o health care professionals, I posed a research question focused on the phenomenon of Latina first-generation college students’ choice and pursuit of careers in health care and medicine.
Data Collection
This study took place at a private university in the northeast United States, where Hispanic and Latina women comprise 10% of the undergraduate student body. Participants were eligible for the original study if they were 18 or older, were enrolled as undergraduate students at the site institution, and had no parents or guardians with bachelor’s degrees. Staff members at the site institution served as gatekeepers and emailed study information to the membership of a large first-generation student organization at the site institution. Interested students completed an electronic interest survey to indicate their interest, report their demographics and education status, and respond to several open-ended prompts about their career goals (e.g., “Please briefly summarize your career/s of interest”). All eligible respondents were invited to participate. Six Latina women who aspired to careers in health and medicine participated in the original study (Table 2); they are the focal point of this research.
Participant Information.
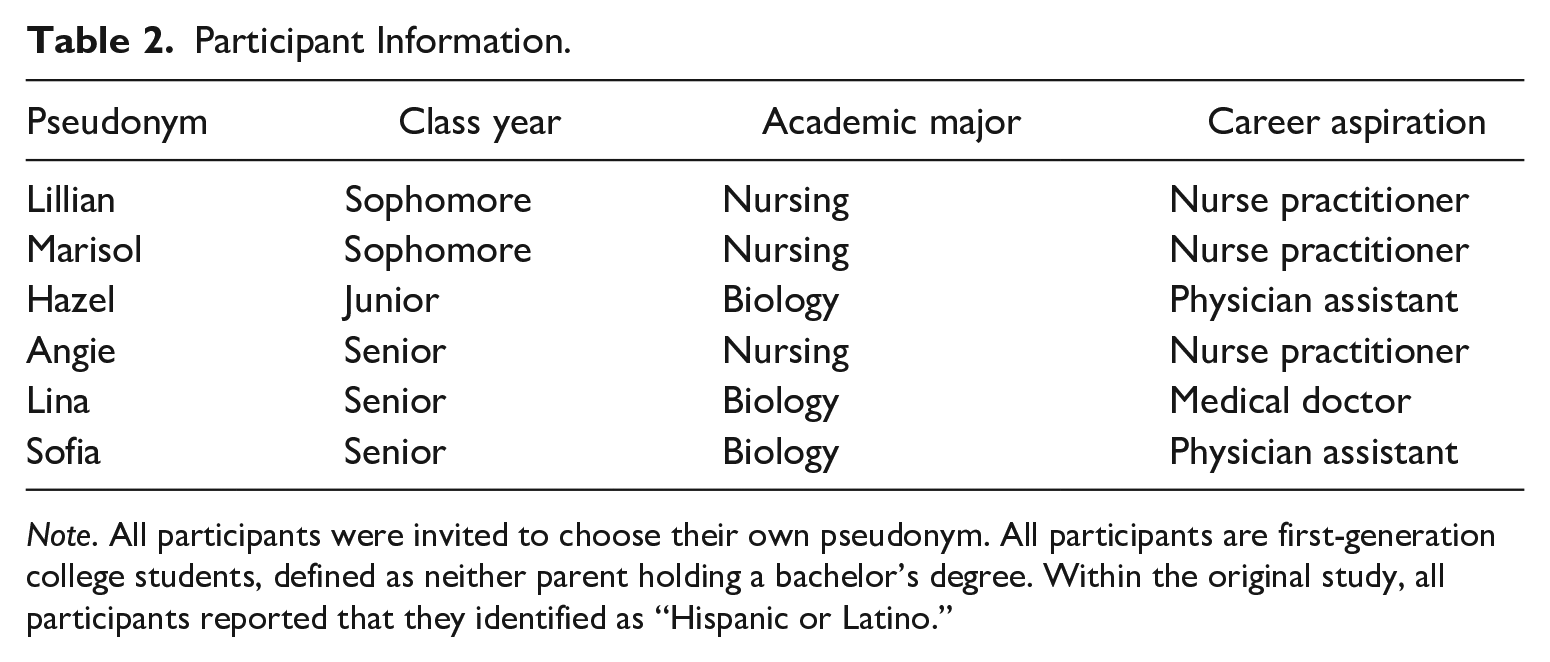
Note. All participants were invited to choose their own pseudonym. All participants are first-generation college students, defined as neither parent holding a bachelor’s degree. Within the original study, all participants reported that they identified as “Hispanic or Latino.”
All participants completed a 1-hour virtual semi-structured interview. Interviews started with a written activity where participants brainstormed key experiences in their education and career journeys. This activity (10–15 minutes) promoted recall and empowered participants’ voice by enabling them to choose their most important experiences without the priming of interview questions. After this activity, participants shared electronic copies of their written material and I asked participants to describe what they wrote during the activity. Following this conversation, subsequent interview questions addressed participants’ decision to attend college, college and major choice, college experiences, and career goals. One participant (Marisol) spent the full interview reflecting on the writing activity. Interviews were recorded, auto transcribed, and edited for accuracy. Participants were compensated with a US$20 Amazon gift certificate.
Data Analysis
Following Moustakas (1994), I first engaged in an epoche, acknowledging my positionality and setting aside prejudgments to approach the data freshly. However, unlike traditional phenomenology, I approached the present study from a post-structural paradigm, acknowledging that societal structures shaped by power, privilege, and oppression influence individual experiences, especially for marginalized groups (Jones et al., 2014), and used Yosso’s (2005) CCW to guide my analytic process. Thus, in phenomenological reduction, where all relevant data units are identified and bracketed, I considered data relevant when they aligned with at least one form of capital according to CCW. All forms of data, including open-ended survey responses, written reflections, and interview transcripts, were analyzed. Next, in imaginative variation, bracketed data are analyzed for themes that account for multiple meanings. In this stage, I examined patterns of capital co-occurrences, as nearly all data units were coded with more than one form of capital. In this process, I identified common co-occurrences of capital and analyzed the dimensions of these relationships, resulting in the themes below.
In analysis, I built trustworthiness via member checking, or asking participants for clarification throughout both data collection and analysis processes. In interviews, for example, protocol questions built directly on participants’ survey responses (e.g., “You indicated that the cost of college influenced your major choice. Can you say more about the relationship between college costs and your decision to major in biology?”). In addition, participants frequently shared unique details in either the written activity or in their verbal responses about the same experiences, with these multiple forms of data serving as complementary points of evidence and enabling triangulation in understanding individual experiences.
Positionality
I conducted this work as a white, non-Latina, non-Hispanic cis woman scholar. I do not share participants’ racial or ethnic identities, which limits my ability to understand their experiences firsthand. Throughout the analysis, I remained conscious of my own social identities, asking participants for clarification throughout data collection, and occasionally consulting them to confirm that my interpretation and analysis accurately represented their experiences.
Findings
All six forms of capital were observed across nearly every participant, demonstrating Latina first-generation college women’s resourcefulness and resilience in pursuing careers in health and medicine. Frequently, women used multiple sources of capital to choose and pursue health careers, including in learning about career options, challenging inequalities in health systems, and giving back to family, especially to honor past and future generations of women.
Learning About Careers in Health Care: Using Social and Aspirational Capital to Accrue Navigational Capital
As first-generation college students, participants were highly resourceful in collecting information to effectively navigate postsecondary education systems and to select careers that aligned well with their values and practical needs. Women actively built social capital in health care fields by talking to their personal health care providers, taking advantage of health-related academic experiences and student organizations, and seeking information online.
Several participants developed interests in health care careers based on interactions with their own providers. Sofia credited her pediatrician as “one of the reasons why I decided to go into medicine.” As a high school athlete, Lillian suffered a hip injury that ended her dreams of running in college but that also gave her firsthand insight into health careers: “Once I hurt my hip, I got to talk to a lot of the nurses. . . [I got to] see the hospital, see how nurses interact with patients.” Lillian continued, “hurting my hip was such a hard thing for me, I couldn’t run anymore and that was my life. But [my nurses] really just made me feel a lot better about it.” Marisol was also hospitalized as a high school student: [In high school], I became really sickly . . . it was scary, but it was also, I don’t know how to explain it, but I want to say exciting. . .I would see how they would do things . . . all these careers in the medical field I didn’t even know about until I was actually a patient. I learned a lot about medicine . . .that kind of gave me a heads up in the medical field.
While in the hospital, Marisol met an NP: “I had never heard of that career until I met her . . . she was really, really nice, really funny . . . I realized that I wanted to be just like her.” Marisol futher explained: Before, I was telling myself, “I’m going to be a doctor, I’m going to be a doctor.” But when I met her, I was like, “no, I want to be a nurse practitioner.” I had a doctor . . . but I barely saw [them] . . . [Nurse practitioner] is more what I want to do, be more patient focused, I feel like doctors just don’t have time for that.
Interactions with health care professionals helped participants to not only understand their interest in health and medicine but to identify career options that best fit their needs and goals.
Participants also built relationships with health professionals through opportunities facilitated by classes and student organizations. Lillian’s high school parenting development class visited a labor and delivery unit where she realized she wanted to work with infants and new mothers. In college, Lillian joined a nursing student organization and met a visiting neonatal NP: “I got to message her privately . . . she said she’ll mentor me when I’m a little older. I got a lot of connections through that club.” Sofia also made a connection when a PA visited her high school sports medicine club. Although she had initially planned to be a doctor, the PA’s visit piqued Sofia’s interest: “[In PA], there’s a lot more flexibility in what I study, what I specialize in, my work hours.” Sofia began talking to her own providers as well: “The medical group I go to now, I’m actually seen by a physician assistant.” By interacting with her PA during checkups, Sofia learned the process and timeline for applying to graduate school: “[I] just ask random questions whenever I go back into the doctor’s office.”
Participants frequently supplemented these interactions with online research. Once she identified an interest in health care, Lillian researched the differences between registered nurse, NP, PA, and physician careers to make an informed choice. For Lina, social media was also an important source of career information, especially in the absence of personal connections. Lina is worried that medical school is going to be a “huge learning curve” and is “nervous of what’s to come”: “I’m going to be the first one in my family to do this. . . I literally have no one else to be like, ‘Hey, what’s expected?’” To learn more, Lina began following two Latina medical students who blog about their experiences: I never really had someone to be like, “Oh wow, I want to be like them, I want to be that doctor,” or anything like that, just because I wasn’t really in those communities. . . Now with social media, you could see that there’s a lot more minorities in the medicine field. And it’s like “Wow, I want to be like them. They’re so cool.”
As first-generation students, women were highly resourceful, collecting career information from health care providers, educational and extracurricular settings, and by independently conducting online research to build their knowledge. For Lina, social media also served as a tool for finding role models in medicine who share her racial and gender identities.
Challenging Inequalities in Health Care: Resistant and Linguistic Capital as Sources of Aspirational Capital
For participants, the absence of Latinx/a/o and Spanish-speaking health care professionals within U.S. health systems served as an important source of motivation. As a 2-year old, Marisol had a “pretty bad case of pneumonia.” When Marisol’s mother took her to the hospital, there was no Spanish-speaking provider and her mother was unable to communicate that Marisol was allergic to antibiotics: “It was a big mess. . . my mom thought I was going to die.” As she grew up, Marisol also observed friends and family members experience limited access to quality health care in the United States and in México. In México, Marisol’s uncle and grandmother had both passed away as a result of medical errors, including a blood transfusion with the wrong blood type. Marisol attributed these issues to the lack of legal protections for patients: I saw the problems going on in México and I was like, “This is what I want to do. I want to be an advocate for the voiceless people who don’t know . . . this is not what’s supposed to happen.”
Lina also recounted her own interactions with health care systems starting at a young age. Lina’s mother “never trusted” doctors in the U.S.: “she wasn’t able to communicate with them, no one looked like her.” Instead, Lina got medical care while visiting family in Colombia: If something was wrong, like with my eyes . . . I would get [care] in Colombia. . .So, just the stress of having to get a whole [plane] ticket for the whole summer just to go to a doctor. I’m sure I’m not the only one that was doing this.
Lina realized that this may be common: “I’m sure a lot of people are going through the same thing,” which further inspired her goals: “I want to be that person for that group of people.’”
As a nursing student, Angie is currently participating in an externship where she has also noticed the lack of providers able to communicate with Spanish-speaking patients: There are actually no Hispanic nurses on my floor . . . that’s giving me even more reason to say, “I can do this.” There are a lot of Hispanic nursing assistants, but there’s no Hispanic nurse. All the nurses for all the Spanish patients we have had, they’re like, “I need you to come in and translate, I don’t know what she’s saying, I don’t know what’s wrong.”
Angie describes “health care equality” as a major source of career motivation, explaining the need for Spanish-speaking providers and high-quality care: “I want to be the provider where all my patients feel comfortable coming to me, not because they have to, but because they want to.” In this theme, participants identified issues in health systems that directly affect the Latinx/a/o community and recognized their own potential for helping to remedy these issues.
Making Family Sacrifice Worth It: Familial Capital as a Source of Aspirational Capital
For all six women, familial capital frequently served as a source of aspirational capital. Across interviews, each woman expressed gratitude for their parents working difficult jobs, taking care of them, and, for most, moving to the United States. Participants often described their pursuit of higher education and a reputable career as a way to thank and honor their parents. “It was known that I was going to college. . . I was repeatedly told that my mom and my dad both left their country to give us a better life” (Lina). Angie described her parents’ sacrifice as her “biggest motivator” and “reason why [she] keep[s] doing it”: “If your parents come here and sacrifice so much, that’s the least you can do. . . just repay them back with this gift of, ‘I did it.’” Hazel describes, “My entire life has been putting trust into my parents and also having conversations with them about experiences that they never got to experience.”
Participants’ drive to give back to family affected educational and career decisions in practical ways. Lina chose a career that was “for sure going to lead me to a path of success and that will allow me to live a nice life myself, allow me to provide for my family, and be a role model for society.” For Hazel, the need to make money was also important: “Being a child of immigrants, [my career] has to be something that makes money . . . you have to make your family sacrifice worth it.” Although she enjoyed English and science subjects, Hazel pursued a career in science: “Out of those two, science is the thing that’s going to make me the most money.”
All participants were very aware of the cost of their education. Lillian plans to follow the military careers of her father and siblings by joining the Air Force once she graduates: [The Air Force] will set me up well financially. I would have medical insurance, I would have money for graduate school, I would get to travel. So, I think that would be the best choice for me right out of college.
As Lillian suggested, the cost of graduate education frequently influenced participants’ goals. Although Hazel originally wanted to be a doctor, the sacrifice of time and money was too great: “I don’t want to spend my entire life in school.” She continued, I don’t want to be $200,000 in debt just to have some sort of reputable career. . . There has to be some other option that won’t cost me that much. . . My parents always tell me, “Debt is terrible. Don’t do it, try to avoid it.”
Hazel saw PA as an alternative that “basically [has] all the responsibilities a doctor has, you just don’t get to be called doctor. . . I can live with that.” For Hazel, being a PA is “reputable enough that my parents can go around and feel proud.” Sofia similarly described, [As a PA], you’re able to pay off loans pretty quickly . . . seeing the flexibility and the income. . .it makes more sense to me to [be a PA instead of a doctor] to achieve that final goal of being able to pay back my parents a little bit for their sacrifice.
As the only participant still aspiring to be a medical doctor, Lina was aware of the length and cost of medical school, a primary factor in her college choice: “Since I want to pursue a [medical degree] . . . I didn’t want to be too in debt. . . it doesn’t really matter where you go for [a bachelor’s], as long as it’s close to dirt cheap.” Across interviews, women discussed parental sacrifices that had enabled them to get a college education. Women also demonstrated concern about postsecondary costs, with the costs of graduate school shaping goals and dampening most participants’ interest in physician careers. For most, making sufficient money to support oneself and to give back to family was a higher priority than the social status of becoming a doctor.
The Strengths of Past, Present, and Future Generations of Women: Resistant and Familial Capital as Sources of Aspirational Capital
The lives of women’s family members and participants’ own identities as women often directly influenced their motivation and career aspirations. Marisol discussed the difficulty of navigating education systems as not only the first person in her family to attend college, but also as a woman facing gendered and ethnic stereotypes: Half of my family really believe in me . . . they were really excited to see where I go. But the other half, they kind of just played into the stereotypes like, “Oh, she’s probably not even going to graduate high school. Like, she’ll end up pregnant and stuff.” But to know that I surpassed that, I worked hard, and I proved them all wrong, it’s kind of satisfying.
Like Marisol, Sofia also felt like she was resisting stereotypes: You hear people say, “She has older cousins that graduated high school and now they have kids, they didn’t do anything with their lives” . . .There were a lot of people who were like, “Well, what makes her different?” . . . It was a little discouraging at first. But then at the same time I was like, “Well, I’m going to prove you wrong.” Going through college and everything like that, it’s intimidating because you know you have this pressure, I guess, of making sure things turn out right.
For participants, success in college and career was also a way to honor the women who came before them. Marisol’s grandmother had been a critical source of support: “Losing [my grandmother] . . .really hurt me because I really wanted her to come to my graduation from high school. I wanted to show her, like, ‘Everything I did was because you inspired me to do this.’” Lina also attributed her success to the generations of women who came before her: All my aunts, they never graduated, they’re all housewives. So, all the cousins, we’ve all expected to go to college and make a name for ourselves. . . We have fostered this, like, feminist attitude. We have been told that you can’t expect a man to provide for you. It’s a whole new world out there. You need to be able to fend for yourselves. . . So, going through college and getting college degrees, [this is] the path to do this.
Women also recognized their role in passing opportunities down to future generations, especially in serving as role models and sources of inspiration for young girls. Marisol describes, What I really want to be is just a role model for my family to show them I went past the misogyny. . . It wasn’t even a boy in my family who graduated high school and who is going to a four-year college, it’s me! I’m a girl, I’m working hard. I’m showing you that you can do this. . . you’re not just going to be a stay-at-home mom or stuff like that. Like, there’s other options for you.
Sofia is also eager to serve as a role model for younger family members and even plans to help her younger sister pay for college. Sofia hopes that her success, despite feelings of isolation and challenge, will help to make the path to college and careers easier for future generations: Having gone through college and hopefully grad school, I’ll be able show [my cousins] that it doesn’t really matter whether you’re the first or the last, you can achieve your dream . . . [I want to be] able to help them and able to guide them, so they have connections that they can reach out to . . .so they don’t feel like they’re kind of all alone, which is what I feel.
Lina was also motivated by the opportunity to inspire future generations: I’ve been telling people repeatedly that I am the face of my future generation, like what’s to come. [My grandchildren are] going to look back and be like, “Oh, my grandma did this, she did that” . . . At the end of the day, you always want to be able to put those that are coming in the future in the best possible place that you can put them in.
Within this theme, women situated their aspirations within a gendered familial context. Participants demonstrated resistant capital via their responses to prejudice, as they disproved negative stereotypes while simultaneously expressing awareness and gratitude for the achievements and sacrifices of the women who came before them. Participants were eager to honor past generations of women by serving as a role models for generations of girls ahead.
Discussion and Implications
Findings provide important insights into Latina first-generation college students’ decisions to pursue careers in health care and their pursuit of these goals. In many ways, findings support existing literature that identifies the resourcefulness and resilience of Latina women in health and science, and the importance of family, culture, and community in motivating women’s success (Johanssona et al., 2020; Loftin et al., 2012; Rincón & Rodriguez, 2021; Rivera-Goba & Nieto, 2007; Rodriguez & Blaney, 2020; San Miguel & Kim, 2015; Sparks et al., 2021; Sánchez-Connally, 2018; Zell, 2014). However, findings also contribute new knowledge by showing how Latina first-generation college students collect information and recognize the needs of an industry and profession. As the first in their families to attend college, women mostly sought career information from outside their families, with participants’ own health care providers and Latina providers with public social media accounts serving as key figures for information and inspiration. As a testament to women’s resourcefulness, even illness and injury served as opportunity for participants to engage with new providers and learn about health careers firsthand. High school and college-level student organizations and classes also provided career information in the form of site visits and guest speakers.
Interestingly, almost all women in this study originally wanted to become medical doctors, although most revised their goals to nursing, NP, or PA. Across participants, health care was described as a stable, well-paying industry that aligned with personal values and goals of giving back to family and community. Although women were drawn to the prestige of becoming a doctor, they were deterred by the temporal and financial commitments of medical school, and by the lack of direct patient care they perceived doctors to have. While nursing, NP, and PA career options may indeed fit participants’ interests, goals, and strengths, findings also illustrate how educational and health care systems deter minoritized students, especially women, from pursuing high-paying and prestigious careers in the health industry. Currently, fewer than 3% of physicians are Hispanic women (AAMC, 2019), despite the growing need for Latinx/a/o health and medical practitioners and providers (LaVeist & Pierre, 2014; Shavers et al., 2012; Terlizzi et al., 2019). Although most participants were interested in physician careers, interest waned as women learned about the requirements, timeline, and costs of medical school, and elements of the career perceived to be inconsistent with their values, especially achieving work/life balance and building strong patient and community relationships.
Overall, participants held a deep pride in their paths, expressing gratitude for the sacrifices of their parents and the previous generations of women in their families and expressing excitement for sharing their success with younger family members and children in the Latinx/a/o community. Consistent with existing research, findings also unfortunately revealed that participants faced gendered and racialized prejudice and feelings of isolation in navigating these paths (Johanssona et al., 2020; Rivera-Goba & Nieto, 2007; Rodriguez & Blaney, 2020; San Miguel & Kim, 2015). Yet, participants, remained focused on their own accomplishments and were fueled by the opportunity to prove others wrong and forge a new path ahead for themselves, and for their families. Through combining multiple sources of capital, participants embody a new generation of opportunity and success for women in their family, and in health care and medical fields, while also generating new sources of capital for future generations.
Recommendations for Practice
This asset-based examination reveals opportunities for improving practice to support the entry and success of Latina women in health and medical careers. First, findings illustrated the importance of education and community settings in building students’ career knowledge, especially for students who are the first in their families pursue and complete college degrees. Teachers, professors, and educational systems must offer course-based and extracurricular opportunities focused on career information, including guest speakers, site visits, and networking opportunities, as they enable students—especially first-generation students—to make informed decisions and build professional networks. Technology should also be leveraged toward this goal, especially to connect students with practitioners who share their social identities. Medical associations and health institutions can also support these efforts by providing financial incentives for health practitioners, especially those who hold minoritized racial identities, to engage with Latinx/a/o K–12 and postsecondary students to talk about their careers. Such engagement would be mutually beneficial, as helping future generations is a value commonly articulated by Latina women in health and medical fields, both in this study and beyond (e.g., Rivera-Goba & Nieto, 2007; San Miguel & Kim, 2015; Zell, 2014).
As physicians and other health practitioners with minoritized identities are desperately needed in the United States (HHS, 2018; Shavers et al., 2012), postsecondary institutions, including undergraduate programs, health graduate programs, and medical schools, must come together to reduce barriers to these careers for Latinx/a/o groups. While there is a promising movement to reduce the costs of medical school (e.g., Doubek, 2018), other barriers remain. In considering careers in health and medicine, participants were attracted to the financial stability and the opportunity to make an impact but were deterred by the fiscal and temporal costs of graduate and medical school programs. Several participants also perceived doctors to have limited opportunities to build meaningful relationships with patients. This study not only reveals avenues for amplifying career learning in K–12 and postsecondary settings, but also a need for health care reform. If health care fields want to effectively recruit Latina women and other minoritized populations into physician careers, these paths must be accessible, and the work must align with students’ values. Health care practice that centers patient experiences and community relationships would not only make physician careers more attractive for these participants, but it would also build community trust and contribute toward improving the quality of care.
Footnotes
Acknowledgements
I deeply appreciate the contributions of the participants in this study, as it was their incredible stories that led to this inquiry. I would also like to acknowledge Seton Hall University Higher Education PhD student Rebecca Wolk for her assistance in data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Participant stipends were from the author’s startup funds, provided by Seton Hall University.