
Abstract
The traditional approach for the treatment of restenosis of autogenous vein bypass has been revision of bypass with vein patch angioplasty, interposition jump graft, or thrombectomy procedures for those patients with extensive occlusive disease and limb-threatening ischemia. Endovascular intervention traditionally involves angioplasty of the graft; however, vessels with diffuse disease or extensive longitudinal lesions are generally difficult to revascularize utilizing this technique. Surgical revision of a threatened autogenous vein graft may carry a morbidity rate as high as 13.6%. We present a series of cases in which excimer laser atherectomy (LA) was used to recanalize an occluded autogenous saphenous vein bypass. Of the occluded vein bypasses failed angioplasty and were successfully atherectomized with LA measuring lengths of 35 and 30 cm, respectively. The infrainguinal has a 6-month follow-up, while the infragencular has a follow-up of 1 year, with resolution of presenting symptoms.
Introduction
The traditional approach for the treatment of restenosis of autogenous vein bypass has been revision of bypass with vein patch angioplasty, interposition jump graft, or thrombectomy procedures for those patients with extensive occlusive disease and limb-threatening ischemia. Autogenous vein bypass has been shown to produce acceptable results when distally anastomosed to the above-knee popliteal artery; however, restenosis of the autogenous conduits are significant. 1,2 Pulsatile arterial flow into the transposed veins leads to adaptive development of hyperplastic neointima, hence the change in lumen diameter. Remodeling of the wall structure may result in focal narrowing within the first 6 to 12 months, leading to reintervention or graft failure. 3 Endovascular intervention traditionally involves angioplasty of the graft; however, vessels with diffuse disease or extensive longitudinal lesions are generally difficult to revascularize utilizing this technique. Surgical revision 4 of a threatened autogenous vein graft may carry a morbidity rate as high as 13.6%. Advances in endovascular techniques and equipment have given surgeons the ability to cross total occlusions with minimal mechanical shearing force and nominal barotrauma to the vessel. Laser atherectomy (LA), a low barotrauma percutaneous intervention, is capable of treating long complex atherosclerotic or thrombotic lesions. We present a series of cases in which excimer LA was used to recanalize an occluded autogenous saphenous vein bypass.
Cases
Case 1
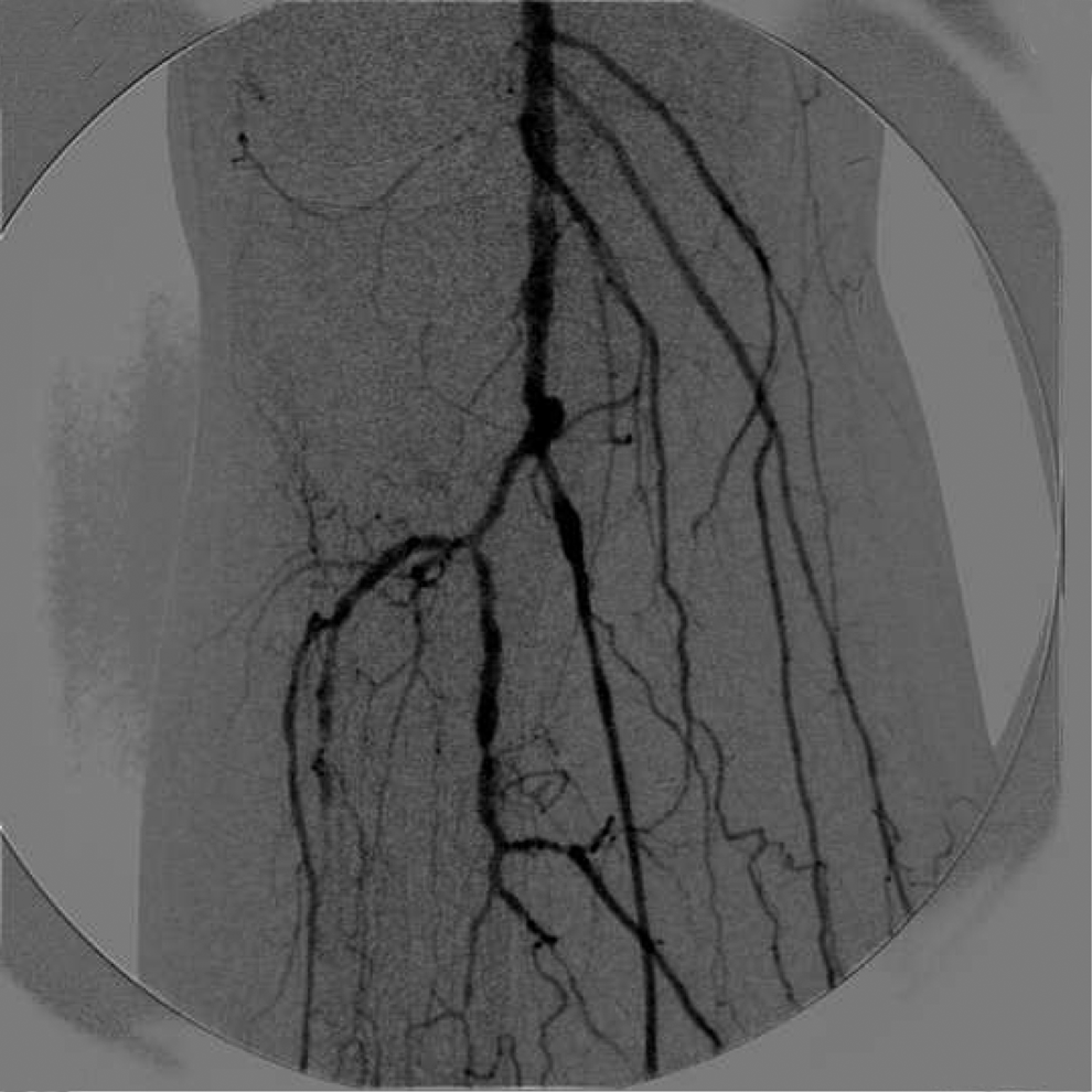
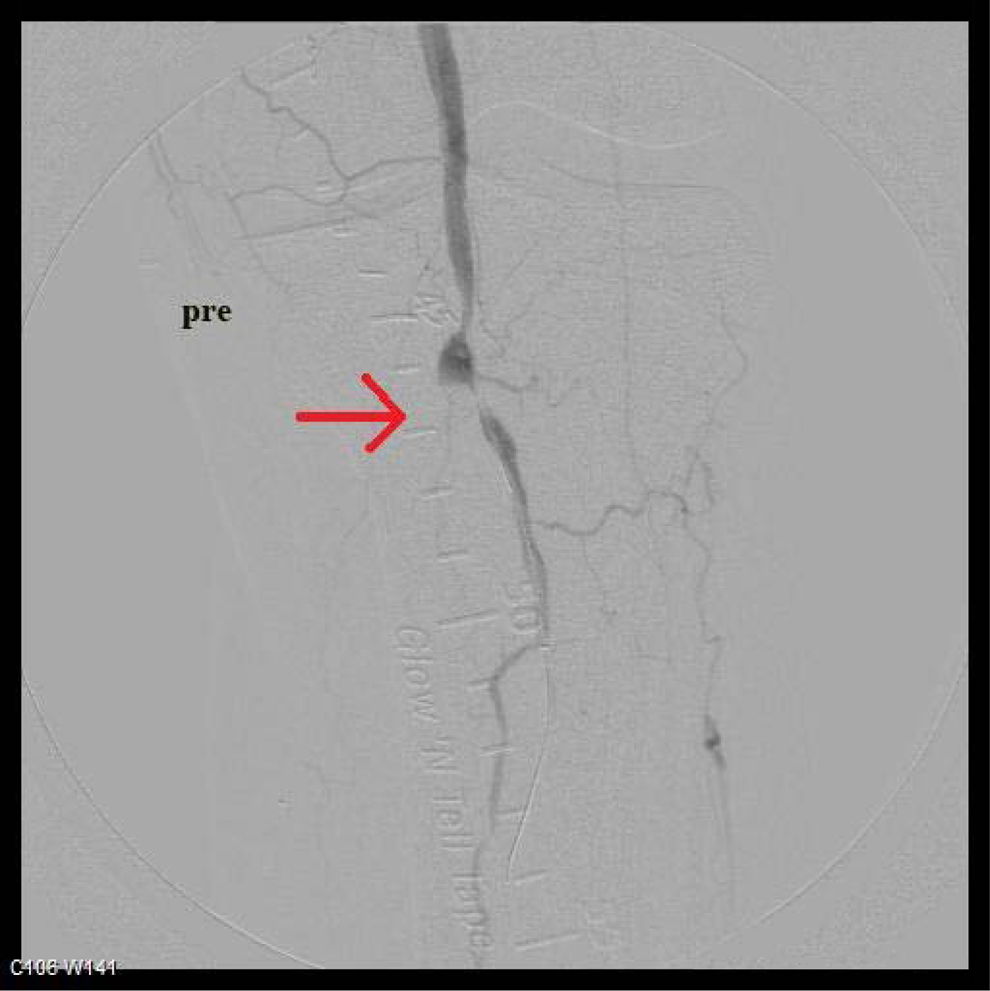
A 42-year-old female presented with a 1 week history of right lower extremity rest pain. Past medical history was significant for extensive peripheral vascular disease, end-stage renal disease, diabetes mellitus, hyperlipidemia, asthma, myocardial infracts ×2, cardiac artery bypass graft, cardiac stenting ×4, multiple deep vein thrombosis, left lower extremity femoral-popliteal bypass, right lower extremity third to fifth toe amputation, and right femoral-popliteal bypass with autogenous saphenous vein graft. Right lower extremity angiogram revealed occlusion of the bypass graft with reconstitution of the above the knee popliteal artery about a few centimeter proximal to the condyles. Below the knee popliteal artery was patent without evidence of the disease (Figure 1 ). Two-vessel run off with the peroneal artery and anterior tibial artery to the ankle. Initial attempts to angioplasty the occlusion were unsuccessful due to the long, complex nature of the stenosis. Subsequent over 0.14 wire, 0.9 mm Turbo Elite laser catheter (Spectranetics Corporation) was introduced and the occluded bypass graft measuring 35 cm in length was atherectomized to the popliteal artery. Next, 1.7 mm Turbo Elite laser catheter was used to fashion a bigger diameter. There was 3 mm channel that was created of the occluded bypass graft. Balloon angioplasty with 3 × 150 mm long balloon was carried out of the whole bypass graft with gentle inflation. Final angiogram revealed a patent reverse greater saphenous vein bypass all the way down the popliteal artery without evidence of stenosis (Figure 2 ). She was started on heparin 6 hours postoperatively then switched to coumadin. The patient was followed at a series of outpatient visits over 6 months during which time she remained asymptomatic; follow-up duplex at 6 months demonstrated patent venous bypass graft.

Patent tip of the graft with distal occlusion marked by arrow.

Patent reverse greater saphenous vein bypass toward the proximal end marked by arrows.
Case 2
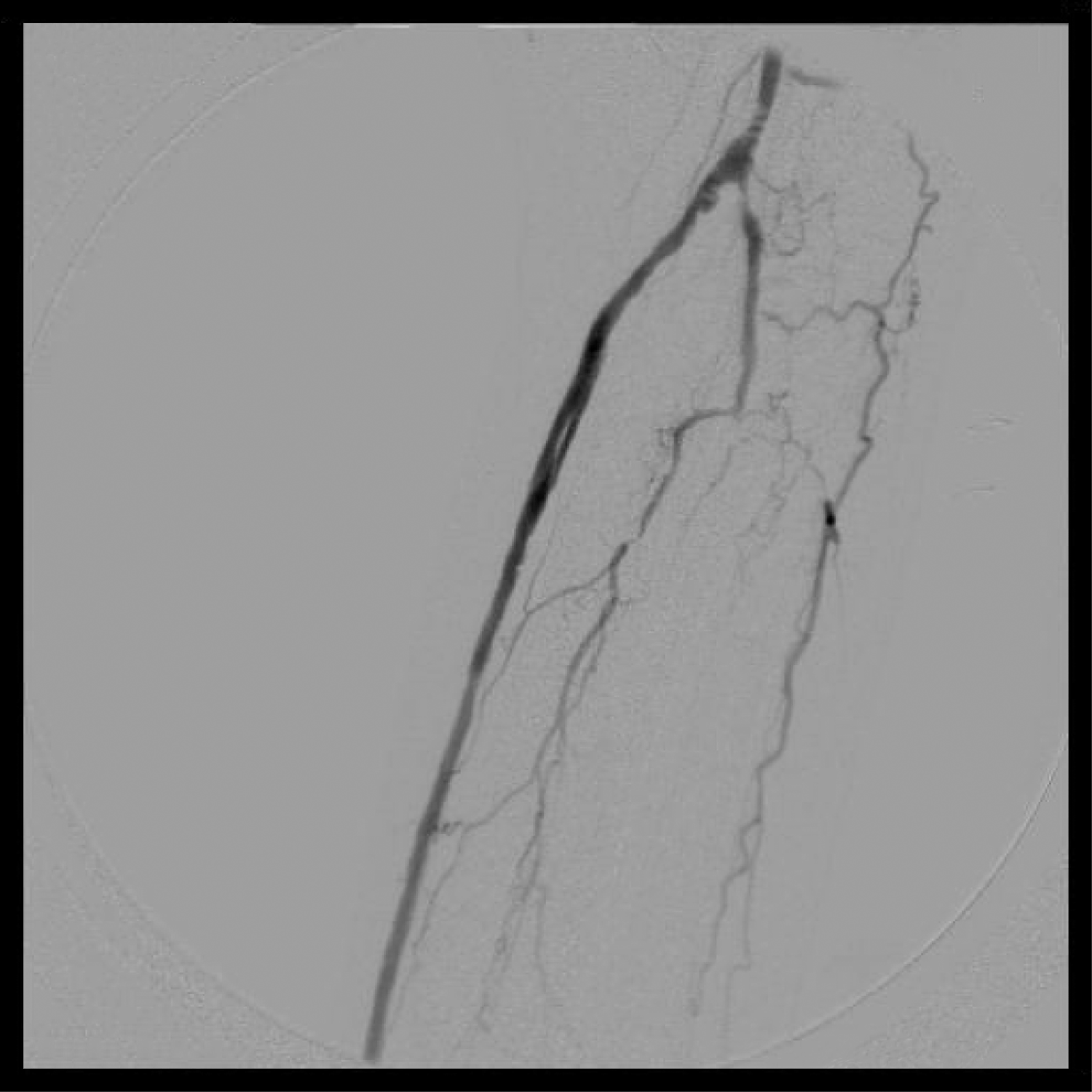
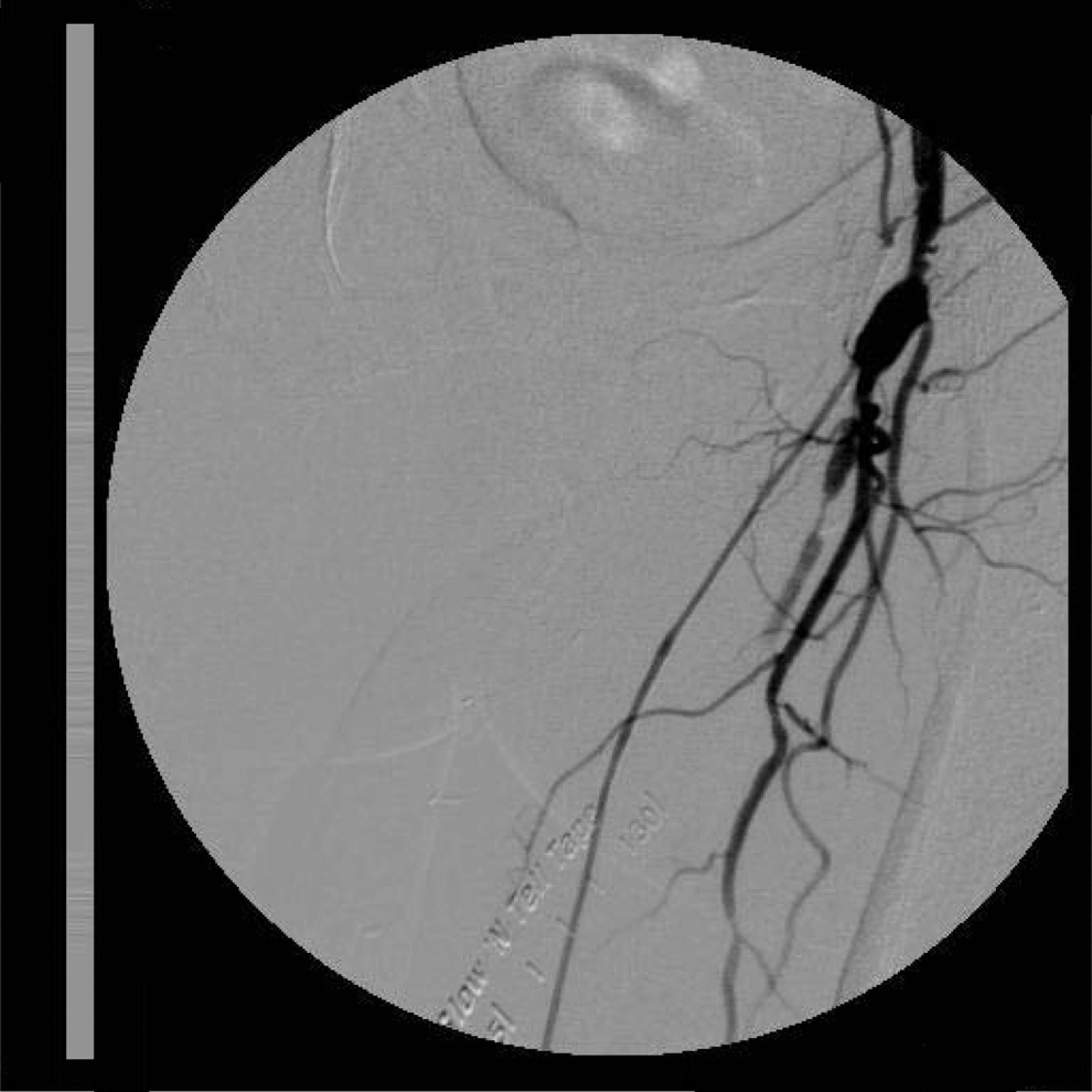
A 66-year-old male presented to our office with a 3-week history of right foot, rest pain as well as a nonhealing, third toe ulcer. Past medical history was significant for extensive peripheral vascular disease, end-stage renal disease on hemodialysis, myocardial infarction, triple coronary artery bypass graft, right popliteal-anterior tibial artery bypass with autogenous saphenous vein graft, and revision of distal anastomosis with interposition vein jump graft. Duplex scan of the right leg revealed that the bypass graft was occluded with diminished waveforms at the ankle. The patient underwent a right lower extremity angiogram, which revealed occlusion of the bypass graft (Figure 3 ). Using a 0.35-inch’ guidewire and 0.035-inch × 135 cm QuickCross support catheter (Spectranetics Corporation, Colorado Springs, Colorado), we crossed the occluded portion of the vessel then attempted a balloon angioplasty of the graft (using 3 × 100 mm balloon) with no technical success. We subsequently performed LA using a 0.9-mm Turbo Elite laser catheter resulting in recanalization of the bypass graft with a residual lumen diameter of 1 to 1.5 mm, approximately 30 cm in length. A second pass was made with a 2.0-mm Turbo Elite laser catheter, increasing the lumen diameter from 2 to 2.5 mm (Figure 4 ). We then performed balloon angioplasty of the vein with a 3 × 100 mm balloon resulting in a patent bypass graft with no evidence of residual stenosis. Postoperatively, arterial duplex revealed a patent right lower extremity bypass graft; dorsalis pedis pulse was now palpable and the patient’s rest pain had resolved. He was started on heparin 6 hours postoperatively then switched to coumadin. The patient was followed at a series of outpatient visits over 12 months during which time he remained asymptomatic and the third toe ulceration was completely healed; follow-up duplex at 12 months demonstrated patent venous bypass graft.

Occluded right proximal popliteal-anterior tibial artery bypass marked by the arrow.
Patent right proximal popliteal-anterior tibial artery bypass marked by the arrow.
Case 3
A 77-year-old male with a history of left popliteal to plantar artery bypass admitted to the hospital with nonhealing left fifth toe amputation site. Past medical history was significant for extensive peripheral vascular disease, myocardial infarction, left popliteal-plantar artery bypass with autogenous saphenous vein graft. Duplex scan of the left leg revealed that the bypass graft was occluded. The patient underwent a left lower extremity angiogram, which revealed occlusion of the bypass graft (Figure 5 ). Using a 0.35 inch guidewire and 0.035 inch × 135 cm QuickCross support catheter (Spectranetics Corporation), we crossed the occluded bypass graft. We subsequently performed LA using a 0.9 and 1.4 mm Turbo Elite laser catheter resulting in recanalization of the bypass graft with a residual lumen diameter of 1 to 1.5 mm, approximately 30 cm in length. We then performed balloon angioplasty of the vein with a 3 × 100 mm balloon resulting in a patent bypass graft with no evidence of residual stenosis. Postoperatively, arterial duplex revealed a patent right lower extremity bypass graft; posterior tibial pulse was now palpable (Figure 6 ). He was started on heparin 6 hours postoperatively then switched to coumadin. The patient was discharged home on therapeutic coumadin.
Selective angiogram of left leg showing occluded bypass.
Selective angiogram of left leg showing patent bypass after laser-assisted angioplasty.
Case 4
A 82-year-old female was admitted to the hospital with nonhealing left fifth toe amputation site. Past medical history was significant for extensive peripheral vascular disease, myocardial infarction, and left femoral to tibio peroneal artery bypass with autogenous saphenous vein graft. Duplex scan of the left leg revealed that the bypass graft had multiple segments of severe stenosis with near total occlusion of the proximal graft. The patient underwent a left lower extremity angiogram, which revealed the bypass graft with stenosis of the proximal anastomosis with areas of severe stenosis all throughout the graft (Figure 7 ). Using a 0.18 inch gold tip wire and 0.018 inch × 135 cm QuickCross support catheter (Spectranetics Corporation), we crossed the stenosed bypass graft. We subsequently performed LA using a 1.7 mm Turbo Elite laser catheter resulting in recanalization of the bypass graft with a residual lumen diameter of 1 to 1.5 mm, approximately 30 cm in length. We then performed balloon angioplasty of the vein with a 2.5 × 100 mm balloon resulting in a patent bypass graft with no evidence of residual stenosis (Figure 8 ). Postoperatively, arterial duplex revealed a patent right lower extremity bypass graft. She was started on heparin 6 hours postoperatively then switched to coumadin. The patient was discharged home on therapeutic coumadin.

Selective angiogram of left leg showing near total occlusion of proximal left fem-tibial-peroneal trunk bypass with Reversed saphenous vein graft
Selective angiogram after laser-assisted angioplasty of left leg bypass
Discussion
The standard management of occluded autogenous vein grafts includes patch angioplasty, interposition vein grafts, vein graft extensions, and occasionally, balloon angioplasty. Surgical revision 4 of stenosed autogenous vein grafts have shown patency rates of 99% at 1 year and 96% at 3 years, with a morbidity rate of 13.6% and a mortality rate of 1%. In the population we serve, endovascular repair is favored since patients are at higher anesthetic risk and most of them lack adequate veins for surgical revision. Excimer LA has been shown to be an important armament among the arsenal of percutaneous therapies. We present the first case series where LA was used to repair vein bypass in patients who have significant comorbidities with long-term follow-up.
There are multiple endovascular options to achieve percutaneous revascularization of lower extremity occlusions and stenoses. Techniques that employ plaque displacement as the primary method of recanalization include balloon angioplasty, microtome assistance (cutting balloon) angioplasty, cryoplasty, and stent deployment. These devices have initially demonstrated excellent outcomes with technical success and limb salvage; however, they are plagued with poor long-term results due to neointimal hyperplasia.
Several have investigated the success rate and efficacy of treatment in patients with stenosed autogenous vein bypass grafts who underwent balloon angioplasty. Tong et al reviewed 90 balloon angioplasties performed on patients with threatened vein bypass grafts. In all, 60% were infragenicular bypass conduits with reported stenosis-free patency rates of 55.8% at 6 months, 54% at 1 year, and 45% at 3 years cumulatively. These investigators noted a statistically significant difference in restenosis rates of below knee bypass grafts (53%) as compared to those above knee (16.4%). 5 Katz and Alexander 6 treated graft stenoses ranging from 0.5 to 3.0 cm using balloon angioplasties with a 31% failure rate at 6 months, 55% at 1 year, and 62% at 2 years; their complication rate was 8%.
The excimer laser (Spectranetics Corporation), approved for peripheral use in 2004 by the US Food and Drug Administration, removes plaque via photoablation. This ultraviolet laser generates a 308 nm wavelength, stimulates plaque composed of lipids, calcifications, or fibrotic tissue (including hyperplastic neointima), leading to disruption of the molecular bonds of the lesion which then disintegrates into particles smaller then 10 μm. The 50 μm laser tip delivers energy in short bursts of 125 billionths of a second causing an increase in molecular vibration within the plaque, resulting in the heating of intracellular water which vaporizes and ruptures the cells. The end product is tissue plaque reduced to <10 μm in size which is absorbed by the bloodstream. 7
Wissgott et al treated 452 superficial femoral artery (SFA) lesions with an average length of 25.5 cm by laser angioplasty. Complications included initial failure of recanalization (14.5%), 142 stent deployment for treatment of dissection (22.1%), perforation (3.9%), and distal embolization (3.3%). Including intent-to-treat failures, the primary patency rates at 1 and 4 years were 50.2% and 26%, respectively. 8
Laird and colleagues analyzed a prospective registry of 145 patients with 155 critically ischemic limbs treated by LA in individuals who were poor candidates American Society of Anesthesiologists (ASA class IV) for surgical revascularization. Vessel occlusions were present in 92% of limbs and the median treated lesion was 11 cm. In this study, stenting was performed in 45% of limbs and procedural success was observed in 86% of limbs. At 6-month follow-up, limb salvage was achieved in 110 (92%) of 119 surviving patients or 118 (93%) of 127 limbs. 9
Scheinert et al were able to treat long, chronic occlusions of the SFA with LA; 411 lesions were treated by excimer LA with successful recanalization in 90.5%. Stent placements were required in 7.3%. Complications included perforation (2.2%) and distal embolization/thrombosis (3.9%). The reported 10 primary and secondary patency at 1 year was 65.1% and 75.9%, respectively, with a technical success rate of 90.5%.
Conclusion
We have presented a case series where endovascular laser-assisted angioplasty has been demonstrated to be an alternative treatment to surgery for autogenous vein bypass occlusions of infrainguinal and infragencular. Of the occluded vein bypasses failed angioplasty and were successfully atherectomized with LA measuring lengths of 35 cm for patient 1 and 30 cm for patient 2, 30 cm for patient 3, and 30 cm for patient 4, respectively. All the patients have been followed up for more than a year with resolution of presenting symptoms. Although there are a limited number of situations in which this treatment may be useful, careful patient selection and early clinical suspicion are 2 factors that may contribute to the success of this procedure. We propose that further large-scale studies assessing the efficacy of LA for autogenous bypass occlusions are warranted to better identify appropriate selection parameters for this therapeutic modality in a challenging patient population. To the best of our knowledge, this is the first reported case series of laser-assisted recanalization of autogenous vein bypass grafts in the literature.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.