
Abstract
Introduction
Endovascular treatment has been increasingly utilized to treat patients with chronic mesenteric ischemia (CMI).1,2 Open revascularization is a durable procedure with excellent patency rates and low chance of recurrence but carries substantial morbidity and mortality, particularly in the elderly or high-risk patients, or in those with cachexia and multiple comorbidities.3,4
The goal of endovascular revascularization is to restore antegrade flow into at least 1 of the 3 mesenteric arteries, preferentially the superior mesenteric artery (SMA). The ideal lesion to treat with stent placement is a focal stenosis without significant calcification or thrombus. Flush occlusions pose a special challenge. The lack of an arterial stump renders visualization, selective catheterization, and recanalization difficult or impossible. In addition, recanalization procedures may be associated with higher risk of intraprocedural complications such as distal embolization, rupture, and dissection. 5 We report 2 challenging cases of recanalization of flush long-segment SMA occlusions in high-risk patients with emphasis on technical tips.
Patients
Case 1
An 80-year-old female presented with 9-month history of progressive postprandial abdominal pain, 50-pound weight loss, cachexia, and recent onset of vomiting and watery diarrhea. Her medical history was notable for hypertension, hyperlipidemia, severe bilateral carotid stenosis, prior transient ischemic attack, coronary artery disease, and peripheral arterial disease. On physical examination, she was cachectic, had limited mobility, scaphoid abdomen with midabdominal bruit, normal upper extremity pulses, diminished femoral and popliteal pulses, and nonpalpable pedal pulses. A dobutamine stress echocardiogram showed inferior and lateral myocardial ischemia. Subsequent coronary angiography confirmed a 4-vessel coronary artery disease which was not suitable for revascularization.
Duplex mesenteric artery ultrasound (DUS) and computed tomography angiography (CTA) confirmed flush occlusion of the celiac axis and SMA, and high-grade stenosis of the inferior mesenteric artery ([IMA] Figure 1A, B). The abdominal aorta had diffuse calcifications, severe stenosis above the IMA origin, and bilateral iliac artery calcification.
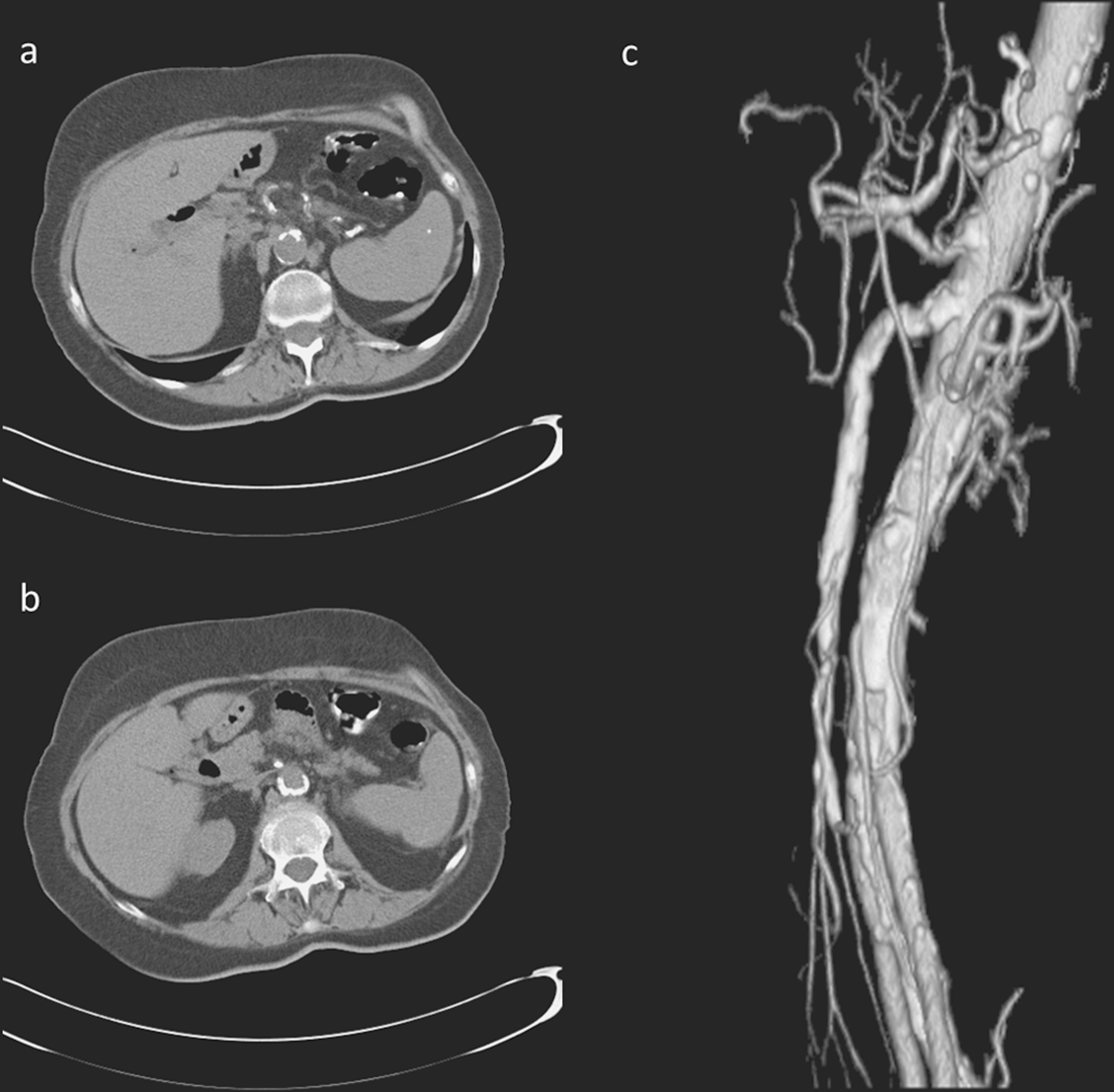
Computed tomography (CT) scan of an 80-year-old female with postprandial pain and weight loss (patient 1). A, Flush celiac trunk occlusion. B, Flush superior mesenteric artery (SMA) occlusion. C, Computed tomography angiogram of patient 2 showing highly calcified infrarenal aortic segment with both flush SMA and celiac artery (CA) occlusion.
Case 2
A 77-year-old female presented with a 7-month history of postprandial abdominal pain and weight loss. Her past medical history was notable for hypertension, hyperlipidemia, Barret esophagus, hypothyroidism, and prior right iliac artery angioplasty for intermittent claudication. On physical examination, she was malnourished and had no bruits or masses but diminished lower extremity pulses. A dobutamine echocardiogram stress test was positive for ischemia. Computed tomography angiography revealed calcified abdominal aorta, severe calcification, and high-grade stenosis at the origin of the celiac axis and flush SMA occlusion (Figure 1C).
Technique
Recanalization of flush SMA occlusion was performed in both patients using left retrograde brachial artery approach. The left brachial artery was accessed using ultrasound guidance and a 0.018-inch micropuncture set. This was exchanged into a 0.035-inch system and a 7F 90-cm Rabee sheath (Cook Medical Inc, Bloomington, Indiana) was advanced to the supra-celiac aorta. A 7F 100-cm MPA guide (Cook Medical Inc) and 5F 125-cm MPA catheter (Cook Medical Inc) combination was used to provide support for selective catheterization of the SMA. Because lateral aortography did not allow visualization of the SMA stump, we used concomitant IMA catheterization and selective IMA angiography via the femoral approach. This yielded optimal identification of the site of reconstitution of the SMA in both cases (Figure 2A). Once the SMA origin was engaged using the MPA guide and catheter, a 0.018-inch V-18 wire (Boston Scientific, Natick, Massachusetts) was used to cross the area of occlusion, followed by a 0.018-inch Quickcross catheter (Spectra medics, Colorado Springs, Columbia). Alternatively, we have used a 0.035-inch soft or stiff glidewire and Quickcross catheter. Predilatation was performed using a 3 mm × 2 cm angioplasty balloon. Stenting was performed using iCAST stent grafts (Atrium Medical, Hudson, New Hampshire). In the first case, this was performed using a 0.035-inch wire and on the second case using a 0.014-inch Spider RX 320-cm filter-wire (ev3 Inc, Plymouth, Minnesota), which was positioned within the main trunk of the SMA distal to the end point of recanalization. In both cases the proximal aspect of the stent was flared using an 8 mm × 2 cm angioplasty balloon. We found that stent flaring facilitates reintubation of the stent in the event of restenosis. A schematic sequence of recanalization, predilation, angioplasty, and stenting as described above is shown in Figure 2B-E.
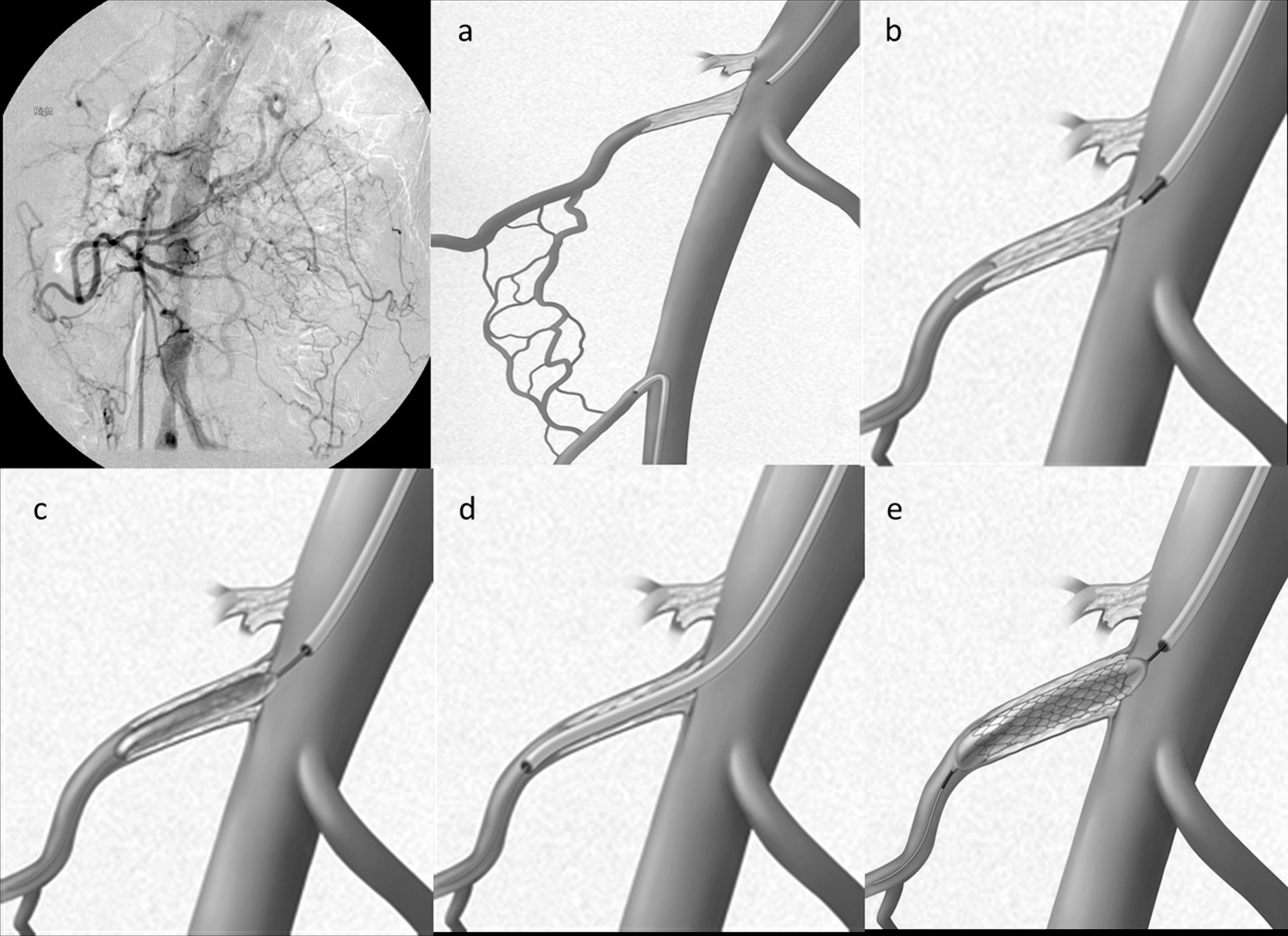
Schematic sequence depicting the endovascular instruction to cross a long-segment superior mesenteric artery (SMA) occlusion. A, Catheter-based angiogram (left) and drawing (right) showing reconstitution of the SMA via inferior mesenteric artery (IMA) obtained through femoral approach. B, Engagement of SMA with a combination of the MPA guide and catheter with subsequent recanalization of SMA. C, Predilation with a 3 mm × 20 mm angioplasty balloon. D and E, Guiding catheter advanced with angioplasty and stenting of the SMA.
The first case was complicated by intraprocedural embolization detected during completion angiography. This was treated using local injection of tissue plasminogen activator (tPA) and an Export XT aspiration catheter (Medtronic, Minneapolis, Minnesota), with complete removal of the distal thrombus and a persistent nonflow limiting dissection flap (Figure 3A, B). Completion angiography in case 2 showed no evidence of complications, residual stenosis, or dissection. Both patients reported immediate symptom relief and were discharged home on postoperative days 3 and 1, respectively. Follow-up at 6- and 12-month revealed no evidence of recurrent symptoms, weight gain of 11 and 12.5 kg, and widely patent SMA stents, respectively.
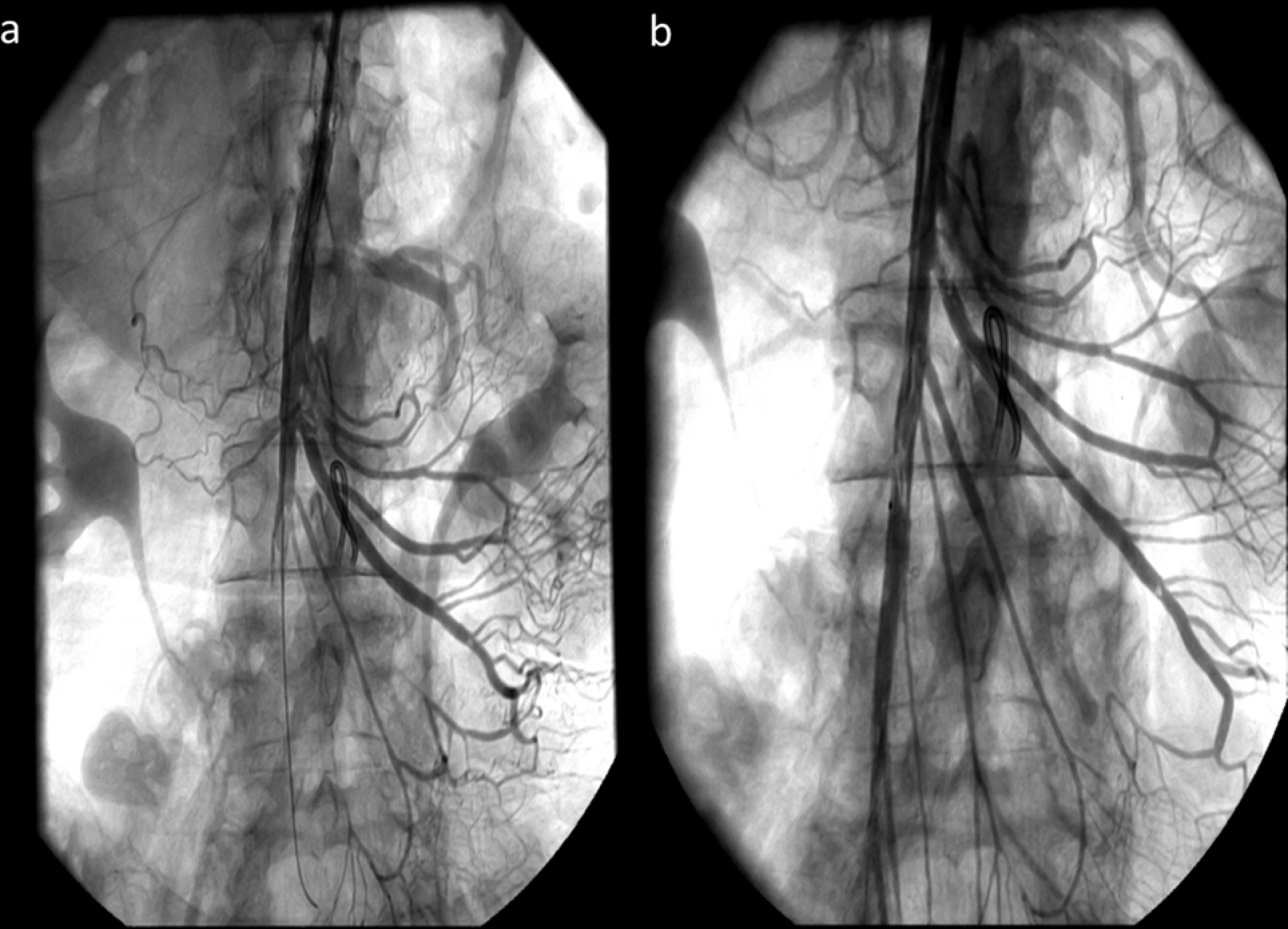
A, Poststenting superior mesenteric artery (SMA) angiogram. SMA occlusion due to distal embolization that was successfully treated with intraoperative pharmacomechanical thrombectomy/thrombolysis. B, Completion angiogram demonstrating a nonflow-limiting dissection flap.
Discussion
Chronic mesenteric ischemia is an uncommon condition typically caused by ostial atherosclerotic lesions affecting at least 2 of the 3 mesenteric arteries. The disease preferentially affects female patients in their sixth or seventh decades of life. Several patients have significant comorbidities and diffuse atherosclerosis of other vascular territories including cardiac, cerebral, renal, and peripheral vascular disease. The natural history of CMI is one of progressive cachexia or progression to acute ischemia leading to bowel necrosis, perforation, peritonitis, and death. Revascularization is indicated in all patients with symptomatic lesions but is not recommended as prophylaxis in patients who remain asymptomatic.
Controversy continues on the ideal method of revascularization (open or endovascular) and whether single- versus multiple-vessel or antegrade versus retrograde revascularization is preferable. Endovascular treatment with angioplasty and/or stenting is associated with less morbidity and mortality, likely higher recurrence rates, and need for more reinterventions.6,7 Alternatively, open surgical revascularization is a durable procedure, but mortality and morbidity are significantly higher in several retrospective series.8,9 The ideal treatment should be individualized taking into consideration the clinical and anatomic factors such as length of the lesion and presence of excessive calcification or thrombus.
Patients who present with cachexia or have severe cardiac and pulmonary diseases are not ideal candidates for open surgical revascularization and should be preferentially treated with a percutaneous approach. When the lesion is not favorable for an endovascular intervention, other alternatives are ilio-SMA, retrograde SMA bypass, or a hybrid retrograde SMA recanalization, avoiding aortic cross-clamping. 10 Although these operations may carry less cardiac risk, the need for open laparotomy is potentially associated with wound healing and pulmonary complications.
Results of mesenteric endovascular revascularizations for CMI show excellent early results. The main concern has been durability. The 1-year primary patency rates and freedom from recurrent symptoms ranges from 33% to 68% and 25% to 75%, respectively.11–14 However, most patients with symptomatic recurrent stenoses are successfully treated with a second endovascular intervention and 1-year secondary patency rates often exceed 95%. A few reports have analyzed stenoses and occlusions separately. Resch and associates reported on 17 patients treated with mesenteric recanalizations and found 96% primary success and 82% freedom from symptoms at 1 year. 13 The Cleveland Clinic group recently reported a larger cohort of patients. 14 There was no difference in results when stenoses were compared with occlusions. 14
The goal of endovascular revascularization is to restore flow into at least 1 of the 3 mesenteric arteries. We generally target the SMA first and consider celiac stenting only if the SMA is not feasible or if we obtained a suboptimal result (dissection or residual stenosis). One percutaneous alternative in patients with unfavorable SMA and celiac lesions is IMA angioplasty and stenting. In our experience, we found higher rates of complications such as rupture at the origin, distal embolization, and dissection. 15 This may be due to the small size of the vessel, angulation, and frequent occurrence of severe calcification at the origin. However, other groups have performed IMA interventions with good results. Sarac and associates found no differences in patency rates for celiac, SMA, and IMA revascularizations. 14 We currently avoid IMA interventions whenever possible.
The ideal lesion for endovascular treatment is a short-segment stenosis without significant calcification or thrombus. Occlusions, longer lesions, or those associated with eccentric or concentric plaque or thrombus are more challenging. One particular scenario associated with great difficulty is flush occlusions, such as the 2 cases presented. The lack of a stump renders visualization of the vessel origin difficult or impossible, unless there are calcifications. In addition, it is difficult to engage the arterial origin or use a stiffer system to cross the lesion. Whereas stenosis and some occlusions can be treated via femoral approach, recanalization of flush SMA occlusions is nearly impossible via the femoral approach.
Use of a stiffer system is of paramount importance to succeed. We recommend using the combination of a sheath, guide catheter, and catheter to provide support. Finally, aortogram requires multiple 20- to 30-mL boluses of contrast for localization of the SMA origin. We found that simultaneous injection of the IMA or one of the internal iliac arteries often allows identification of the distal SMA end point and probable SMA origin for probing with the wire.
In both cases we have used a balloon-expandable stent grafts as opposed to the standard uncovered stents. The rationale for this was possibly less risk of rupture or distal embolization. However, this benefit has not yet been confirmed for mesenteric stenting in patients with CMI.
Conclusion
High-risk patients with CMI who are not ideally suited for open mesenteric revascularization should be treated with mesenteric angioplasty and stenting. Flush SMA occlusions are challenging lesions but may be recanalized with good results. Technical aspects that facilitate recanalization include use of a brachial approach, stiffer system, and concomitant IMA angiography to minimize the use of contrast.
Footnotes
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Gustavo S. Oderich is a consultant for Medtronic.
The author(s) received no financial support for the research and/or authorship of this article.