
Abstract
Arteriovenous (AV) loop grafts are a type of vascular conduit that can be used to support free tissue transfer. Wounds of various etiologies may require free tissue transfer, and the AV loop graft is a useful adjunct when adjacent blood supply is inadequate. Here we present 2 cases and review the technique and published literature.
Keywords
Introduction
Complex wounds, such as those encountered in patients with diabetes, trauma, or radiation injury, may be difficult to heal. When primary closure of a large soft tissue defect is impossible and healing by secondary intention fails, coverage with free tissue transfers can be considered. Inadequate adjacent arterial supply and venous outflow, due either to the injury or to the preexisting vascular disease, may preclude free tissue transfer. In such cases, the use of the arteriovenous (AV) loop graft technique can be employed.
The AV loop graft is constructed using basic vein harvest and anastomotic techniques familiar to vascular surgeons. Venous conduit, typically greater saphenous vein, is used to create an AV fistula. The midpoint or apex of the fistula is placed as near the wound as possible to facilitate anastomosis to the vascular pedicle of the free flap. The fistula is subsequently divided at the midpoint and used as arterial inflow and venous outflow for the free flap. In this report, we discuss 2 cases of AV loop graft creation for successful free flap coverage of complex wounds and review the published literature on this technique.
Patients and Methods
Patient 1 is a 48-year-old man with a history of locally aggressive anorectal carcinoma and a large soft tissue defect of the perineum and sacrum. He had undergone multiple surgical resections, as well as chemo- and radiotherapy, resulting in a defect measuring 13 × 10 × 8 cm. He was evaluated by plastic surgery, and, after multiple debridements and applications of a vacuum-assisted closure (Wound VAC, KCI, San Antonio), was deemed to be a candidate for free flap reconstruction. Vascular surgical consultation was requested due to lack of suitable inflow and outflow vessels for the free flap.
Venous duplex vein mapping was performed, and the patient had suitable greater saphenous vein (diameter greater than 3 mm). At operation, the common femoral, femoral, and profunda femoris arteries were dissected and controlled. The greater saphenous vein was identified at its junction with the common femoral vein, dissected to the level of the midcalf with a series of jump incisions, and disconnected at its distal aspect. The proximal aspect was left in situ for venous drainage. A tunnel was fashioned over the lateral thigh so that the loop graft would reach approximately 2 cm away from the edge of the soft tissue wound. After tunneling, the vein was anastomosed to the common femoral artery (Figure 1).
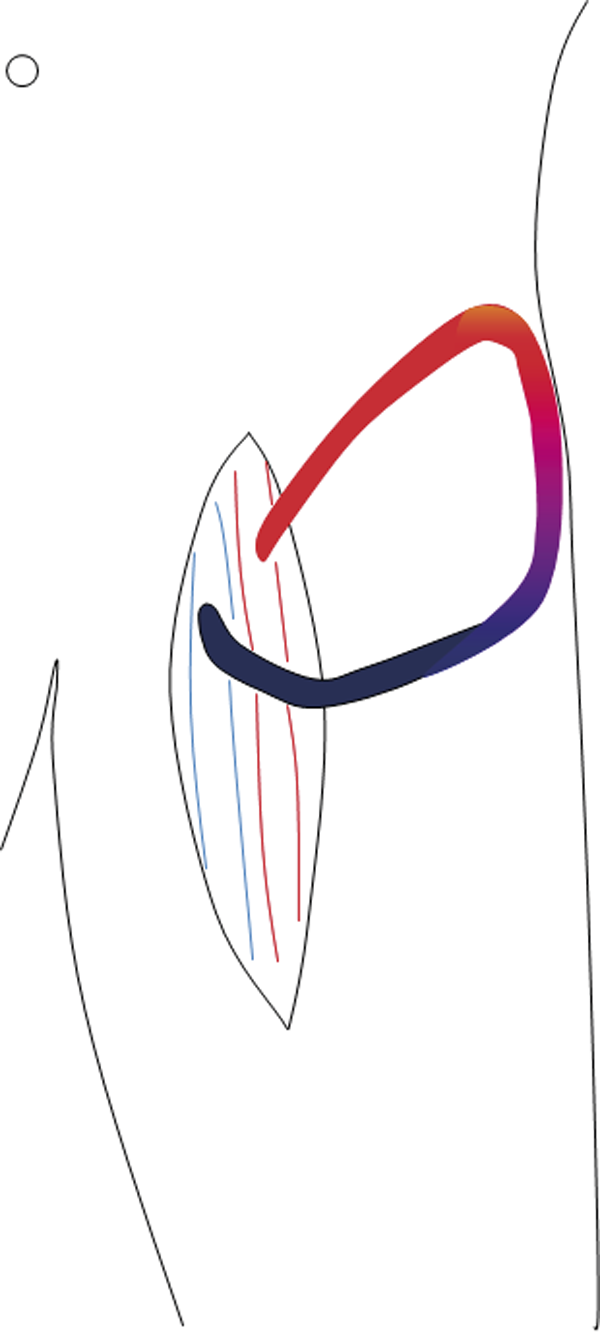
Configuration of femoral arteriovenous loop graft.
Four days later, the patient returned to the operating room with the plastic surgery team. A latissimus dorsi free flap was harvested. The AV loop graft was exposed and divided at its apex. The arterial and venous anastomoses were completed with 9-0 nonabsorbable monofilament suture. One week later, the patient returned to the operating room for final, minor debridement and refinement of the flap, and split-thickness skin grafting of the flap (Figures 2 and 3).

Wound prepared for grafting.
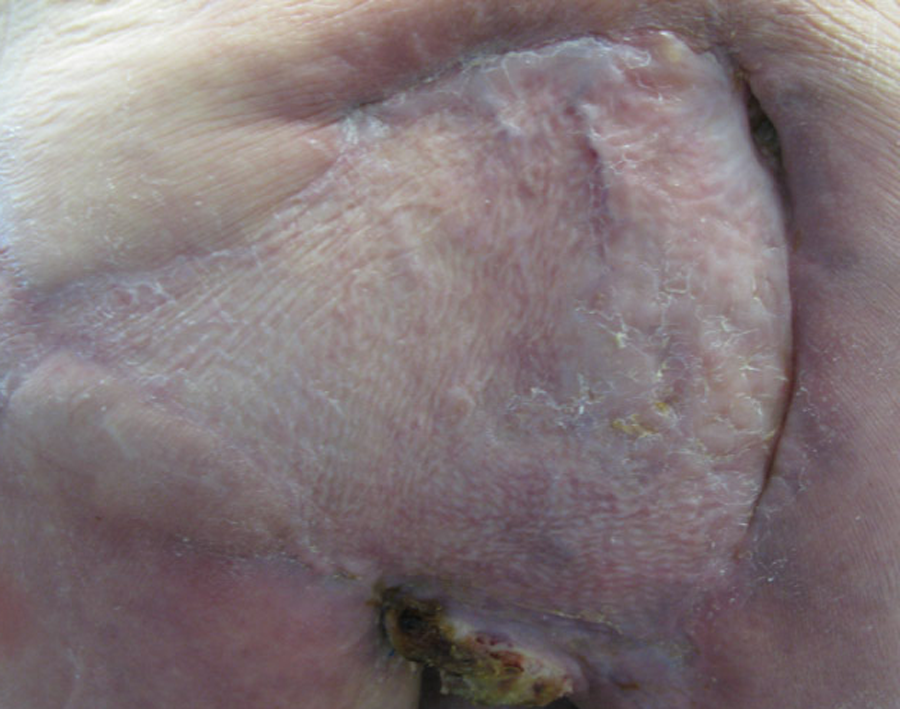
Wound closure after free flap and healed split-thickness skin grafting.
The patient expired from complications of his cancer 3 months later.
Patient 2 is a 31-year-old female with a history of a mixed glioma brain tumor. She had undergone multiple surgical resections as well as treatment with gamma knife radiation, chemotherapy, and local radiation. She developed a 10 by 15 cm open scalp wound with exposed cranium. A latissimus dorsi free flap based on the facial artery and vein was attempted but failed due to inadequate flow. Split thickness skin grafting also failed to close the wound.
Venous duplex vein mapping was performed, demonstrating the left greater saphenous vein to be 2.5 mm in the thigh. This was harvested at operation to be used for an AV loop graft. Through a cervical incision, the internal jugular vein and external carotid artery were controlled. A circumauricular tunnel was fashioned through which to tunnel the AV graft. After systemic heparinization, the arterial (external carotid) anastomosis was completed, the vein was brought through the tunnel, and the venous (internal jugular) anastomosis was completed (Figure 4).
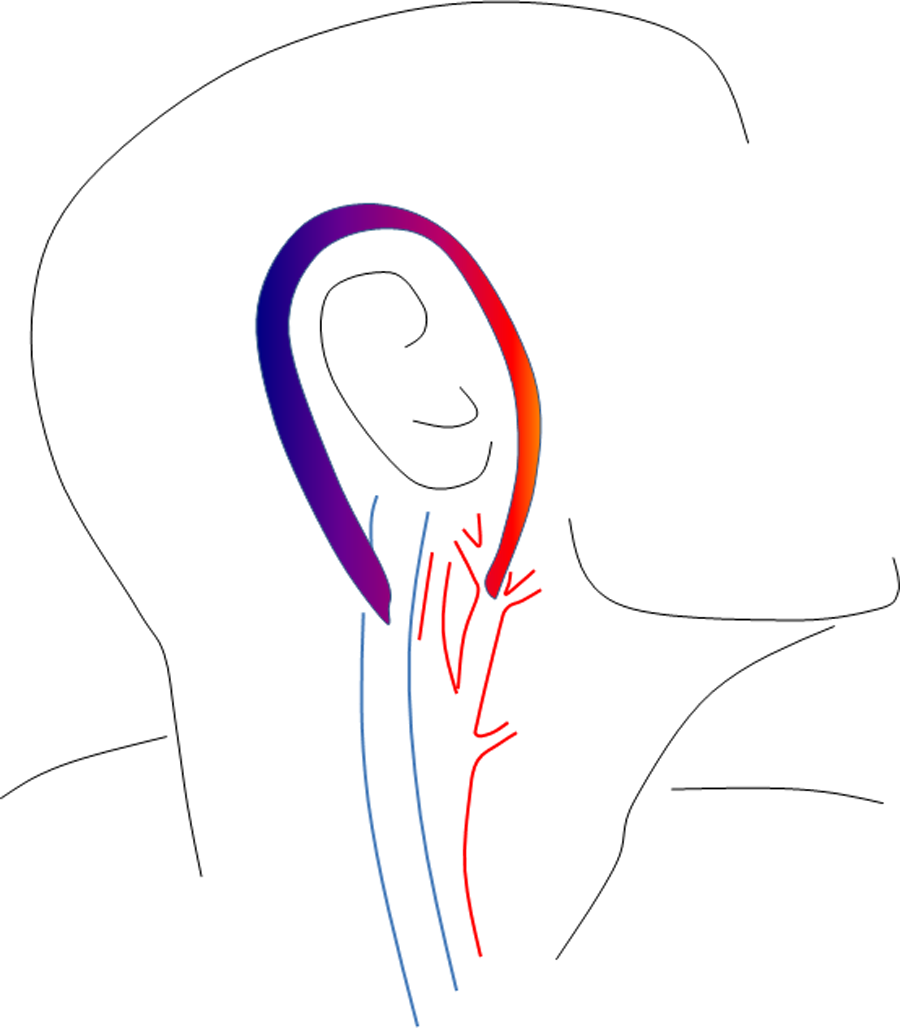
Configuration of carotid–jugular arteriovenous loop graft.
Four days later, the patient returned to the operating room with the plastic surgery team. The wound was debrided. A rectus abdominus flap was harvested, and the apex of the loop graft was exposed and divided. Arterial and venous anastomoses were completed in standard fashion. A few days later, the patient returned to the operating room for split thickness skin grafting of the flap.
Although she has had recurrence of her malignancy, the wound has remained closed 14 months later (Figures 5, 6, and 7).

Nonhealing scalp wound.

Wound with after free flap placement.

Wound following split-thickness skin grafting.
Discussion
Arteriovenous loop grafts can be constructed using methods familiar to practicing vascular surgeons. They are a useful adjunct to extend the vascular supply to areas in need of free flap coverage but with inadequate adjacent arterial inflow or venous outflow.
We have performed our operations as a 2-stage procedure, while others have advocated a 1-stage procedure. Oswald et al performed a series of 1-stage procedure with success, and after reviewing both 1- and 2-stage procedures, advocated this approach, based on a literature review that showed equal complication rates. 1 It is our opinion, however, that a 2-stage approach divides the case into 2 more manageable procedures. This ensures each respective surgical team adequate time to perform their portion of the procedure—these cases often require more dissection and meticulous operative technique than many vascular and reconstructive procedures. Furthermore, when the procedure is staged, the fistula can be observed for several days to be certain that it has adequate flow to support the free flap. If both procedures are done in a single setting, and the free flap loses flow, it may be difficult to tell whether the problem is with the graft or with the inflow or outflow conduit.
We perform the anastomoses from the free flap to the conduit in an end-to-end fashion with interrupted sutures. Although this technique may take longer than creating a running suture line, size discrepancy between the graft and the conduit can be resolved. This technique also eliminates “purse-stringing” which may occur with a running suture line.
Various configurations of the vascular graft can be employed depending on the location where soft tissue coverage is needed. Inflow and outflow vessels need not be adjacent to each other. The saphenous vein can be removed entirely and transposed to a different location or the venous drainage left intact and only an arterial anastomosis created, as was done in patient 1 and previously described in a similar case. 2
Arteriovenous loop grafts have application in a multiple scenarios in which vascular supply is compromised, including reconstruction for trauma and for diabetic tissue loss. When limb salvage cannot be accomplished because inadequate distal targets preclude traditional bypass, a loop graft can be used to support a free tissue transfer. Multiple authors have reported good success with this approach.
Atiyeh et al reported successful limb salvage in diabetics with nonhealing foot wounds. Of the 7 patients with diabetic foot ulcers 6 were successfully treated with free tissue transfer supported by AV loop graft.3,4 Sunar et al reported limb salvage in 11 of 13 treated extremities. 5
Cavadas reported a series of 56 procedures, 40 of which were for reconstruction after trauma and 6 of which were for treatment of diabetic foot wounds. A variety of free flaps were successfully transferred, including muscular, bone, osteocutaneous, and omental flaps. All 50 flaps performed survived. 6 Lin et al described a large series of AV loop grafts used in trauma patients and achieved a 91% limb salvage rate. 7
Conclusion
Coverage of complex soft tissue wounds can be difficult and may require a multispecialty approach. Basic vascular surgical techniques can be employed to create vascular conduits for support of free flaps when no adjacent vessels are available. These techniques have been shown to have successful application in the coverage of wounds of various etiologies including trauma, radiation, diabetes, and malignancy.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.