
Abstract
A 46-year-old female was found to have a saccular superior mesenteric vein (SMV) aneurysm on computed tomography (CT) scan during workup for abdominal pain. It measured 3.5 cm in diameter. The SMV aneurysm was successfully resected, and the SMV was repaired with femoral vein patch angioplasty. She was placed on Coumadin for 3 months. At follow-up, the vein patch repair was patent and the patient was doing well with complete resolution of her abdominal pain.
Introduction
Visceral venous aneurysms are rare clinical entities. Most are located within the portal venous system, accounting for almost 90% of visceral venous aneurysms. 1 On the other hand, aneurysm of the superior mesenteric vein (SMV) accounts for approximately 9% of all visceral venous aneurysms. 1 They are usually found incidentally on radiographic studies. Complications are commonly associated with thrombosis or rupture. Surgical intervention is successful in selected patients; however, the treatment of portal venous aneurysms remains controversial.
Case Report
The patient is a 46-year-old female who initially presented to her primary care physician with intermittent right upper quadrant abdominal and pelvic pain for the past several years. In the 3 weeks leading up to her initial visit, the abdominal pain had worsened in intensity and frequency. She described the pain as intermittent and also complained of bloating. However, the symptoms were not associated with meals. She had no changes in bowel habits, weight loss, or melena. Her medical history included gastroesophageal reflux disease, vaginal hysterectomy, and bilateral salpingo-oophorectomy. She neither smokes tobacco nor drinks alcohol. Family history was negative for hypercoagulopathy and deep venous thrombosis. Physical examination was unremarkable, except for a periumbilical scar. The abdomen was soft and nontender without appreciable mass or bruits. Peripheral pulses were intact on bilateral upper and lower extremities.
During her workup, the initial computed tomography (CT) scan of the abdomen and pelvis revealed a 3.5 cm vascular mass in the right upper quadrant (Figure 1). There was no intraluminal thrombus. This mass originated from the SMV. Selective mesenteric arterial angiography with delayed portal venous imaging confirmed multiple significant venous collaterals entering this saccular SMV aneurysm (Figure 2) which precluded endovascular covered stent therapy.
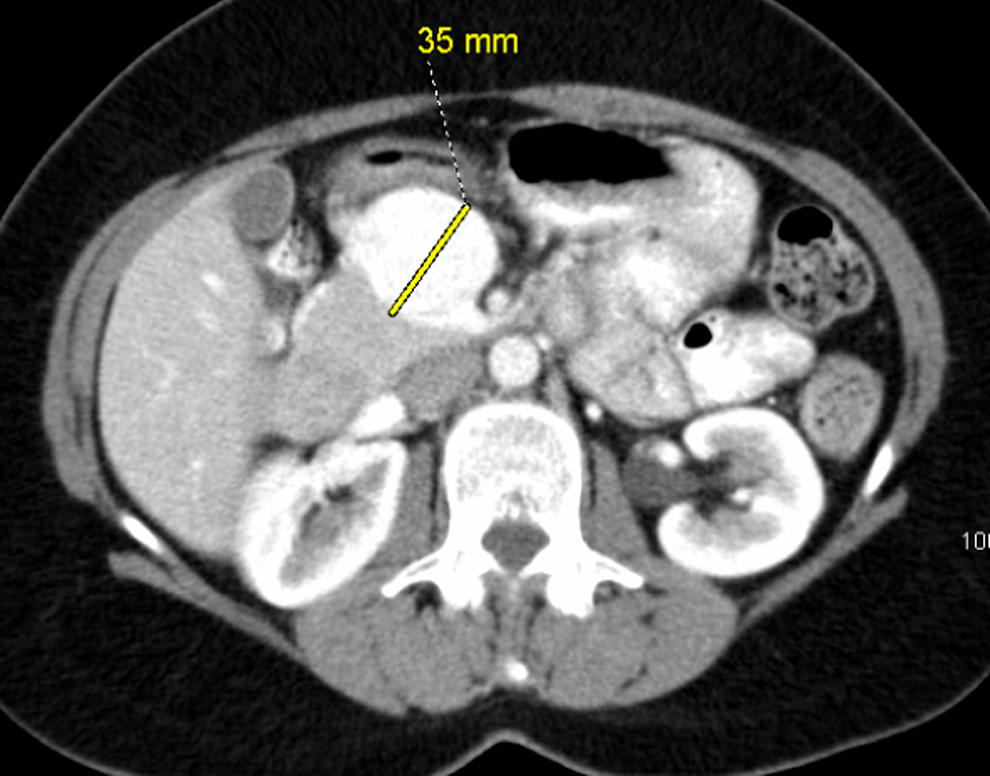
Computed tomography scan of the abdomen and pelvis revealing 3.5 cm SMV aneurysm. SMV indicates superior mesenteric vein.

Catheter angiography revealed multiple venous collaterals feeding into this SMV aneurysm. SMV indicates superior mesenteric vein.
Thus, she underwent exploratory laparotomy through a chevron incision. The SMV aneurysm was exposed initially through the root of the mesentery. The SMV was controlled distally, at the confluence with the splenic vein, through the lesser sac. This saccular aneurysm was resected and the SMV was repaired with a right femoral vein patch angioplasty (Figure 3). The postoperative course was uncomplicated and unremarkable. She was discharged on postoperative day 3. She was maintained on Coumadin therapy for the following 3 months. A follow-up CT scan demonstrated a patent SMV repair and complete resolution of the SMV aneurysm (Figure 4). Portal venous duplex scan at 1 year showed a patent SMV with normal waveforms (Figure 5).
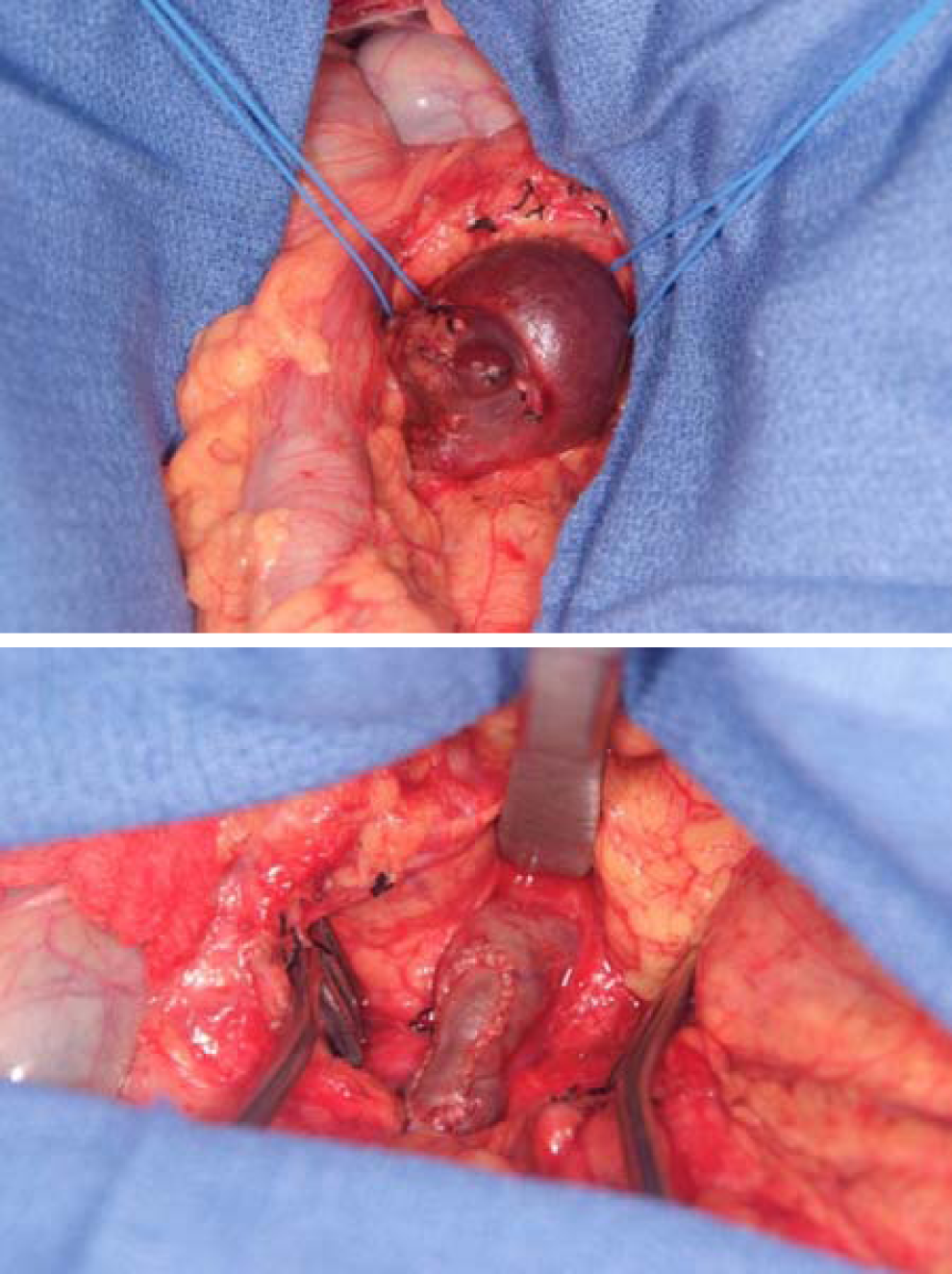
Intraoperative images of the SMV aneurysm, followed by repair with a femoral vein patch. SMV indicates superior mesenteric vein.

Contrast CT of the abdomen showing resolution of SMV aneurysm at 3 months. CT indicates computed tomography; SMV, superior mesenteric vein.
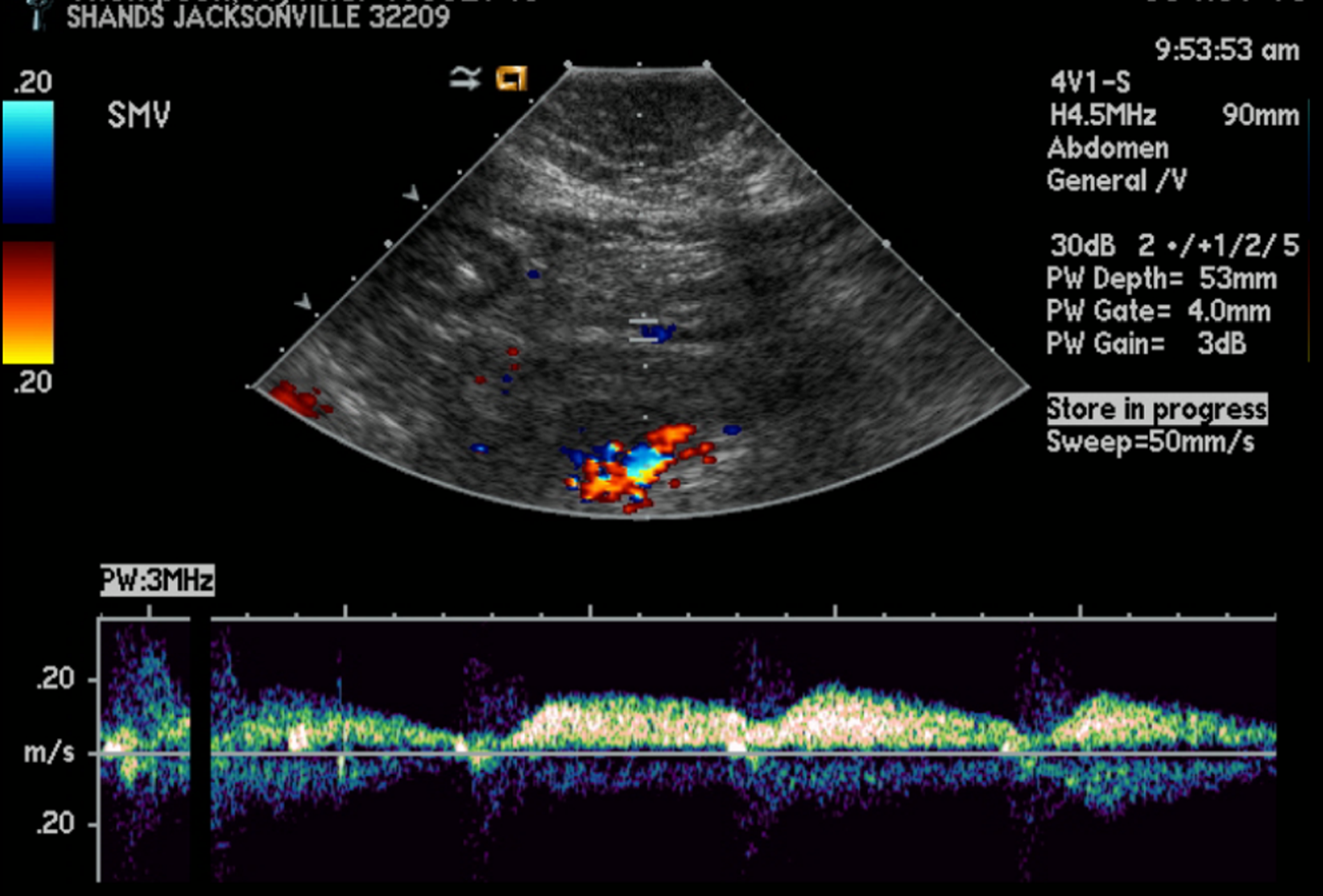
Portal venous duplex scan at 1 year showed a patent SMV with normal waveforms and no evidence of SMV aneurysm or thrombus. SMV indicates superior mesenteric vein.
Discussion
Portal venous aneurysms are uncommon entities, accounting for 3% of all venous aneurysms. 2 They are defined as a dilatation of more than 2 cm. Its incidence is difficult to define as most are found incidentally now that more abdominal radiographic examinations, such as ultrasound or CT scans, are being performed. The 2 most common locations are the main portal vein and the confluence of the SMV and the portal vein. Aneurysms of the SMV account for approximately 9% of visceral venous aneurysms. 1 Currently, there are 2 major theories for the development of portal venous aneurysms. They can be acquired or congenital. Some of these aneurysms are associated with underlying hepatic disease and portal hypertension.3–6 Pancreatitis can also lead to surrounding inflammatory response that could weaken adjacent vessel wall and give rise to venous dilatation. 6 However, others believe that it is also congenital as it had been found in patients of relatively young ages and in those without predisposing factors and diseases.1,7,8 In addition, portal venous aneurysms have been documented in utero. 9 Schild proposed that a small diverticulum may form during early embryonic development because of aberrant regression of the right vitelline vein. This incomplete regression may eventually lead to enlargement of the proximal SMV and form the aneurysm.7,10
Most patients with portal venous aneurysm are asymptomatic. However, those with symptoms are likely to present with vague abdominal pain that tends to recur and localize in the right upper quadrant. 10 Still, others report upper gastrointestinal bleeding 11 that occurs from rupture or less commonly, jaundice secondary to biliary compression and obstruction 8 from the mesenteric vein aneurysm.
Typically, an aneurysm will appear as an anechoic structure that lies in the expected location of the SMV on ultrasound. 3 Computed tomography angiography and magnetic resonance imaging (MRI) will reveal the size, shape, and extent of the aneurysm. Selective mesenteric/portal angiography can further evaluate the aneurysm for endoluminal therapy in selected patients.
Treatment of portal venous aneurysms remains controversial. They vary from close observation to endovascular therapy or open surgical intervention. Observation can be reserved for those who are medically at high risk of interventions and those who are reliable in case symptoms that develop over time. However, these patients will require at least annual follow-up to evaluate any change in size of the aneurysm. In 1 study, the aneurysm diameter remained stable and no complications occurred in 94% of patients who were followed with serial abdominal ultrasounds. 1 On rare instances, extrahepatic portal venous aneurysm had been found to regress spontaneously during yearly follow-up. 12
Reported complications of untreated aneurysms include thrombosis, rupture, and compression of adjacent structures. In most cases, interventions are the result of the presence of symptoms or the occurrence of these complications. Prophylactic intervention is also advocated for low-risk patients since there is no consensus as to what size these aneurysms may be observed. The type of procedure is based on aneurysmal size and location and medical and surgical comorbidities. Endoluminal therapy may be the best alternative modality for those with normal anatomy. In addition, patients with multiple comorbidities and with a significant-sized aneurysm may undergo endoluminal therapy. Open surgical repair may be reserved for relatively healthy individuals and those with tortuous anatomy and multiple feeding venous collaterals that are not amenable to endovascular repair. Surgical techniques include aneurysmorrhaphy with patch angioplasty or resection and interposition bypass graft.
Conclusion
Superior mesenteric vein aneurysms are rare and treatment remains controversial. For young and healthy patients, such as the patient presented in this case report, an open surgical approach is durable and associated with low morbidities.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.