
Abstract
Aim: The aim of this study was to compare midterm mortality between anemic and nonanemic patients undergoing endovascular repair of abdominal aortic aneurysm and to assess a correlation with markers of inflammation. Methods: Anemia was defined as hemoglobin <13 (men) and <12 g/dL (women). The impact of anemia and inflammatory markers on mortality was assessed using Kaplan-Meier curves and Cox regression. Results: A total of 224 patients (12 females [5.36%]; age: 69.73 ± 8.72 years) were included; 102 (45.53%) were anemic. Median follow-up was 17 months (interquartile range: 7-25 months). Nine patients died (1.79%; 8 anemic vs 1 nonanemic). Survival was lower for patients with anemia (log-rank, P = .01). White blood cell count and C-reactive protein (CRP) differed significantly (P < .001 and P = .01). Anemia and CRP were associated with decreased survival (Cox regression, P = .01, hazard ratio [HR]: 0.35, 95% confidence interval: 0.14-0.84 and P = .002, HR: 1.18, 95% CI: 1.06-1.31). Conclusion: Patients with anemia had decreased survival over the midterm; inflammatory markers were higher among this group.
Introduction
Abdominal aortic aneurysm (AAA) constitutes a significant health problem in 5% to 10% of men above the age of 65 1 ; pathologically, it is associated with chronic aortic wall inflammation. 2,3 Endovascular repair of abdominal aortic aneurysm (EVAR) is associated with lower perioperative morbidity, less blood loss, and quicker recovery, as compared to open reconstruction; therefore, patients with greater comorbidity are increasingly being offered elective repair. 4 As a result, there is a significant need of predicting those at highest risk based on variables collected preoperatively in order to plan accordingly. Various authors have retrospectively investigated the value of preoperative factors in predicting the outcome of EVAR, including biochemical laboratory tests, 5,6 and scoring systems previously applied to open repair. 7
Anemia is commonly encountered in the setting of chronic inflammatory conditions, such as AAA. 8,9 A recent retrospective study suggested a link between preoperative anemia and mortality in patients undergoing EVAR 6 but failed to show a direct link between anemia and inflammatory markers. The aim of this study is to investigate the potential association of baseline anemia with midterm mortality following elective EVAR and to investigate a possible causative link by demonstrating whether patients with anemia have significantly increased inflammatory markers.
Methods
Study Design
Patients undergoing elective EVAR of an infrarenal AAA between January 2008 and April 2011 in a single tertiary referral center, who met the inclusion criteria and provided written informed consent, per institutional guidelines, were entered prospectively in a registry that aimed to assess the predictors of outcome in elective EVAR. Ethical approval was obtained by the institution’s review board committee.
Inclusion and Exclusion Criteria
The primary indication for EVAR was AAA transverse diameter >5 cm or a rapidly increasing sac of <5 cm; any symptomatic infrarenal AAA was also eligible. Ruptured, mycotic, and inflammatory aneurysms were excluded from this series. General contraindications for EVAR were age <18, allergy to contrast medium, coagulopathy, pregnancy or lactation, groin infection, life expectancy <1 year, and connective tissue disease. Patients with an aneurysm at another location and patients with end-stage renal failure requiring dialysis were excluded from the analysis.
Study Protocol
Recruitment
Demographics and comorbidities, including a full past medical and surgical history, full anesthetic assessment, and a full vascular examination were obtained at baseline (prior to EVAR). All patients underwent a computed tomographic angiography (CTA) with 2- or 3-dimensional (3D) reconstruction or magnetic resonance angiography (MRA) prior to repair. Nonsteroidal anti-inflammatory drugs (NSAIDs) and other nephrotoxic medication were stopped at least 1 week prior to EVAR due to the risk of contrast-induced nephropathy (CIN). Blood specimens were collected for a full blood count and routine biochemistry tests preoperatively, on the day of the admission for the elective operation. All specimens were analyzed at the institution’s laboratory on the same day. C-reactive protein (CRP) levels were measured using nephelometry (Immage 800 analyzer; Beckman Coulter, Brea, California). Full blood count was obtained using an automated hematology analyzer (CELL-DYN Sapphire analyzer; Abbott Laboratories, Abbott Park, Illinois). Data were entered in a database prior to EVAR once written informed consent had been obtained.
Follow-up
All patients were followed up according to our department’s standard EVAR protocol, which included plain abdominal radiography (anteroposterior and lateral views) and a contrast-enhanced CTA at 6 months, and annually thereafter. A full clinical examination was performed at every follow-up visit. Conventional angiography was reserved for investigation of suspected endoleak or graft occlusion. Data from follow-up visits, including results from blood tests, were entered in a database at the time of visit. Mortality and mode of death were assessed by contacting the patient’s next of kin and reviewing the patient’s case notes from our institution or the institution of their last admission prior to their death, if necessary.
Definitions
All complications and events during follow-up were classified and reported systematically, according to the reporting standards for endovascular aneurysm repair by Chaikof et al. 10 Anemia was defined as a hemoglobin level <13 g/dL for men and <12 g/dL for women, 11 according to the World Health Organization definition.
Procedures
The following endovascular devices were used: Anaconda (Vascutek, Inchinnan, Scotland, UK), Gore Excluder (Gore Medical, Flagstaff, Arizona), EndoFit tube graft (LeMaitre Vascular, Burlington, Massachusetts), EndoFit aortouniiliac device followed by a femorofemoral bypass (LeMaitre Vascular), Talent (Medtronic, Minneapolis, Minnesota), Endurant (Medtronic). Indications and specifications for the implantation of each device in this center have been described in detail elsewhere. 12 –14 Whenever a bifurcated endograft could be implanted, the aortouniiliac configuration was avoided as it involves an extra-anatomic bypass.
All procedures were performed in a fully equipped operating room with the patient under regional or general anesthesia and fluoroscopic control, by administering iopromide (Ultravist 300; Bayer Schering Pharma AG, Berlin, Germany), a nonionic contrast agent. All operations were performed by the same team of vascular surgeons and anesthetists with previous experience in EVAR using all the devices included in the analysis.
In accordance with our department's standard protocol for patients undergoing EVAR, 15 aspirin and clopidogrel were administered on the day of the procedure. Aspirin was discontinued on postoperative day 30, and clopidogrel was continued as a lifelong treatment. 15 During the perioperative period (<30 days), patients received a blood transfusion if their hemoglobin was <8 g/dL or if they were symptomatic and had a hemoglobin<10 g/dL. A plain abdominal radiograph was obtained on postoperative day 2 to assess graft integrity and position. The patient was usually ambulated on postoperative day 2 and was discharged on day 3.
Statistical Analysis
All analyses were performed using SPSS (Version 13.0; SPSS, Chicago, Illinois). Continuous parametric data are presented as mean value ± standard deviation or range, where appropriate; nonparametric data are presented as median and interquartile range. Categorical data are presented as absolute values and percentages. For univariable comparison of continuous data, the Student t test (parametric) or Mann-Whitney U test (nonparametric) was applied accordingly. Categorical data were compared using Fisher exact test. Survival and complication rates during follow-up were compared using the log-rank test. Kaplan-Meier curves were constructed for survival rates. Cox proportional hazard analysis, adjusted for baseline variables with a significant difference in univariate comparison, was applied to assess the effect of hemoglobin concentration on survival. P < .05 was considered statistically significant.
Results
A total of 224 patients (12 females [5.36%]; mean age: 69.73 ± 8.72 years) were included in the analysis. Mean aneurysm diameter was 6.07 ± 1.22 cm (Table 1). A total of 102 patients (45.53%) were found to be anemic prior to the operation. The only baseline variables that were significantly different between anemic and nonanemic patients were white blood cell (WBC) count and CRP. Baseline characteristics are summarized in Table 1. Anemic and nonanemic patients were compared in terms of history of cancer, age, sex, and all factors known to be associated with anemia 8 (Table 1).
Patient Demographics, Comorbidities at Admission, and Anatomical Characteristics
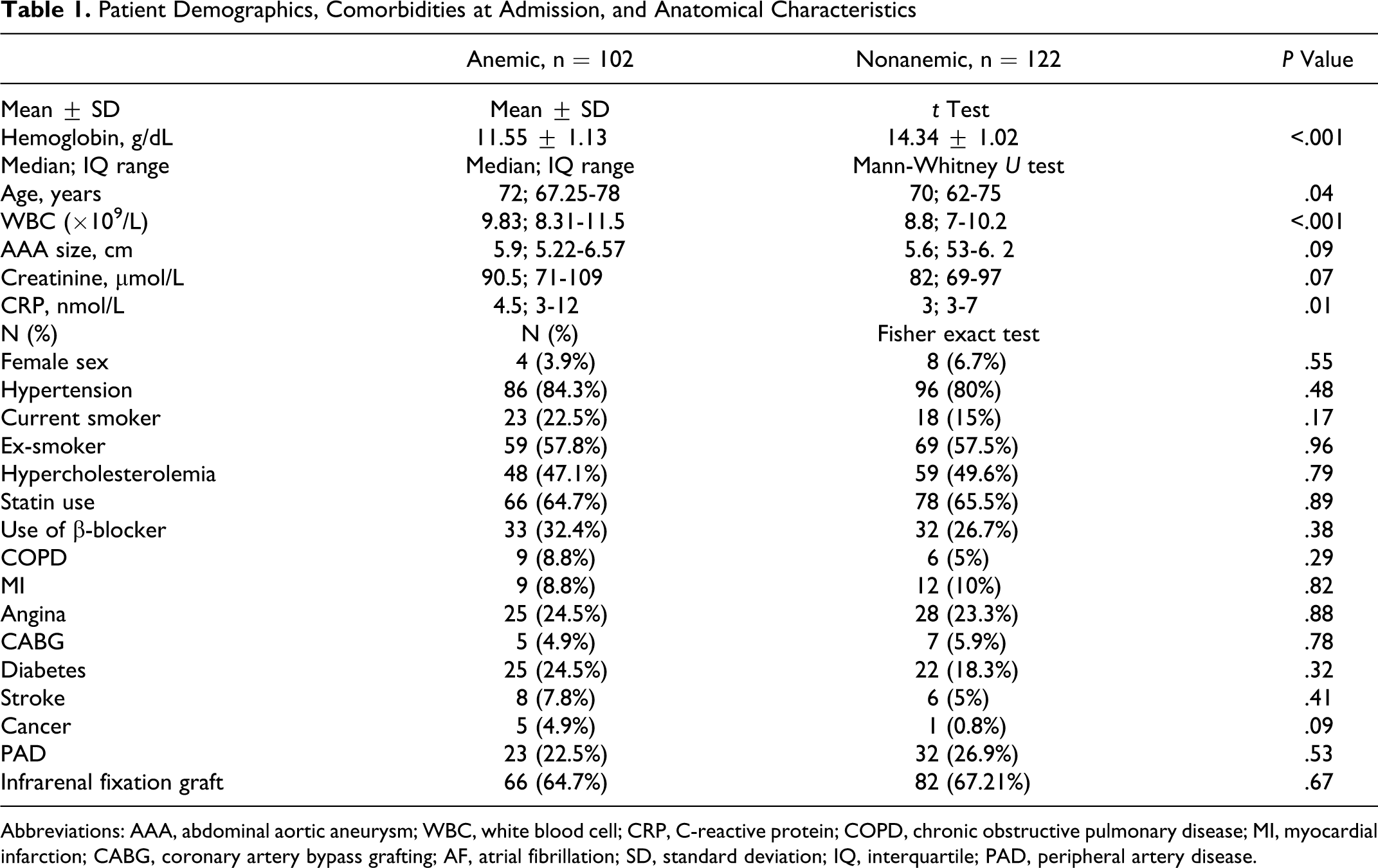
Abbreviations: AAA, abdominal aortic aneurysm; WBC, white blood cell; CRP, C-reactive protein; COPD, chronic obstructive pulmonary disease; MI, myocardial infarction; CABG, coronary artery bypass grafting; AF, atrial fibrillation; SD, standard deviation; IQ, interquartile; PAD, peripheral artery disease.
None of the patients in either group were taking immunosuppressive medications prior to EVAR. The NSAIDs were stopped at least 1 week prior to EVAR in all cases, to prevent CIN.
Median follow-up was 17 months (interquartile range: 7-25 months). No patient was lost to follow-up.
The mean operative time was 119 minutes (range, 59-162 minutes). The following devices were deployed: Anaconda—123 patients; EndoFit aortouniiliac and femorofemoral bypass—10; EndoFit tube graft—37; Endologix—11; Endurant—19; Gore Excluder—15; Talent—8; and AneuRX—1. An endograft with an infrarenal fixation mechanism (no suprarenal stents or other suprarenal fixation modality) was deployed in a total of 66 (66 of 102 [64.7%]) patients with anemia as compared to 82 (82 of 122 [67.21%]) nonanemic patients (P = .67).
Perioperative blood transfusion (within 30 days of the operation) was required in 17 patients (7.59%); none required more than 2 units of blood. All the patients that required a blood transfusion had undergone surgical exposure of at least 1 or one femoral artery to allow sheath and device introduction. There was no difference between anemic and nonanemic patients in terms of the need for perioperative blood transfusion (10 [9.8%] vs 7 [5.74%], P = .32).
There were no intraoperative deaths. One patient died perioperatively (1 of 224 [0.44%]). Overall, 9 patients died during follow-up (9 of 224 [1.79%], 8 anemic vs 1 nonanemic patient). The causes of death and other events are summarized in Tables 2 and 3. Survival was significantly lower in patients with anemia preoperatively (log-rank test, P = .01; Figure 1). Cox regression analysis adjusted for age, WBC at baseline, AAA diameter, serum creatinine concentration at baseline, history of cancer prior to EVAR, type 1 endoleak, and CRP at baseline revealed that hemoglobin concentration and CRP (both baseline) were associated with mortality (P = .01, hazard ratio [HR]: 0.35, 95% confidence interval [CI]: 0.14-0.84 and P = .002, HR: 1.18, 95% CI: 1.06-1.31, respectively; Table 4).
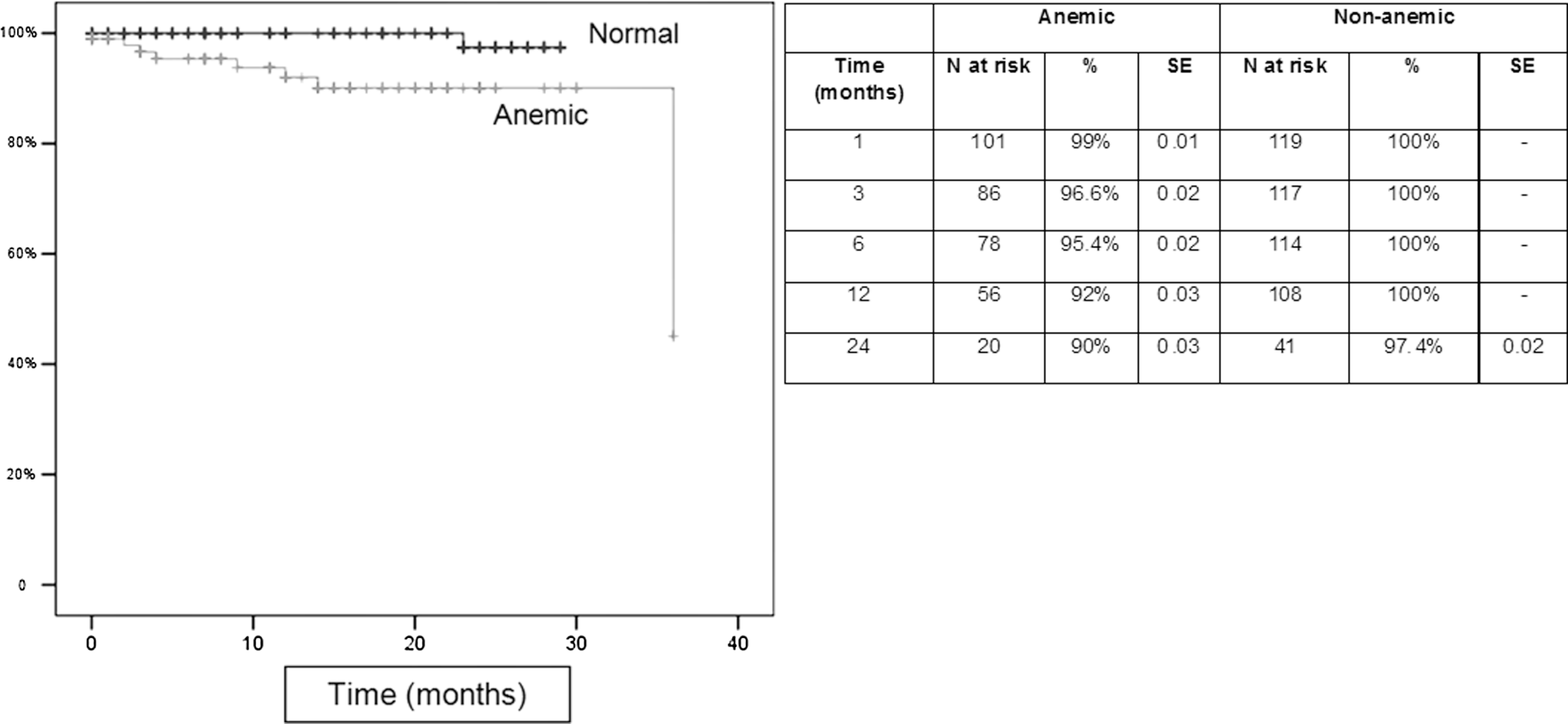
Kaplan-Meier curve comparing survival between anemic and nonanemic patients (24 months; log-rank test P = .01) and patients surviving and number of patients at risk at each time interval.
Cause of Death During Follow-Up
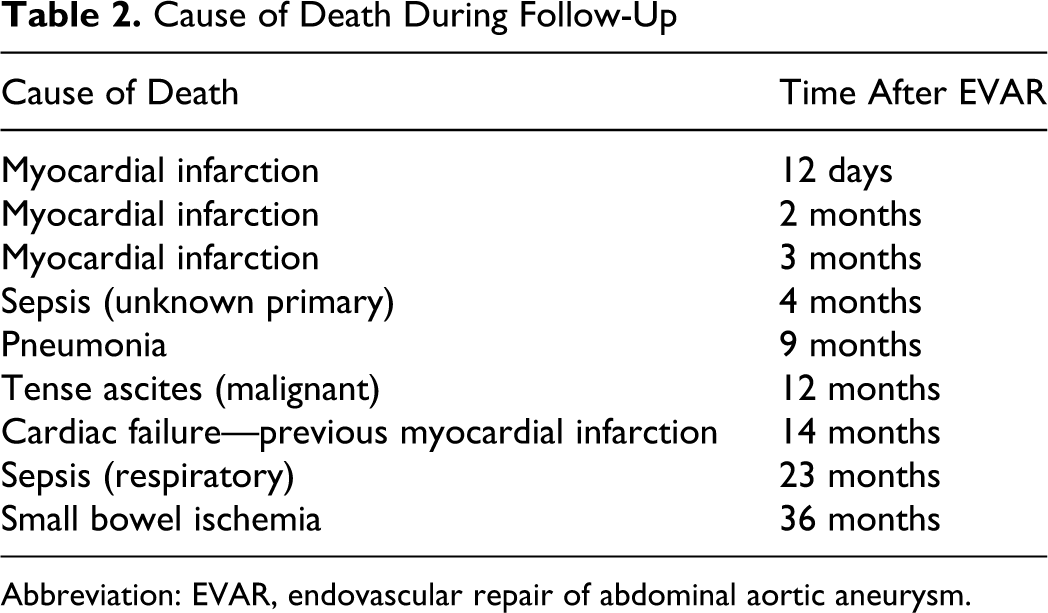
Abbreviation: EVAR, endovascular repair of abdominal aortic aneurysm.
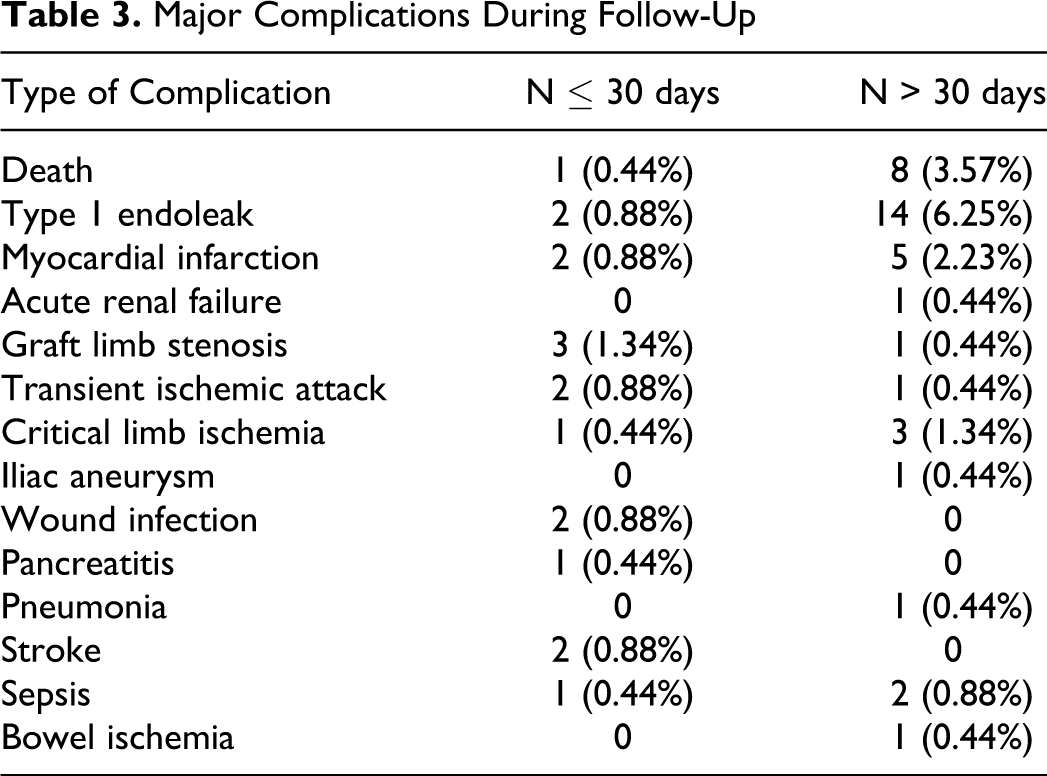
Major Complications During Follow-Up
Cox Regression Analysis for Mortality Over Midterm Follow-Up.
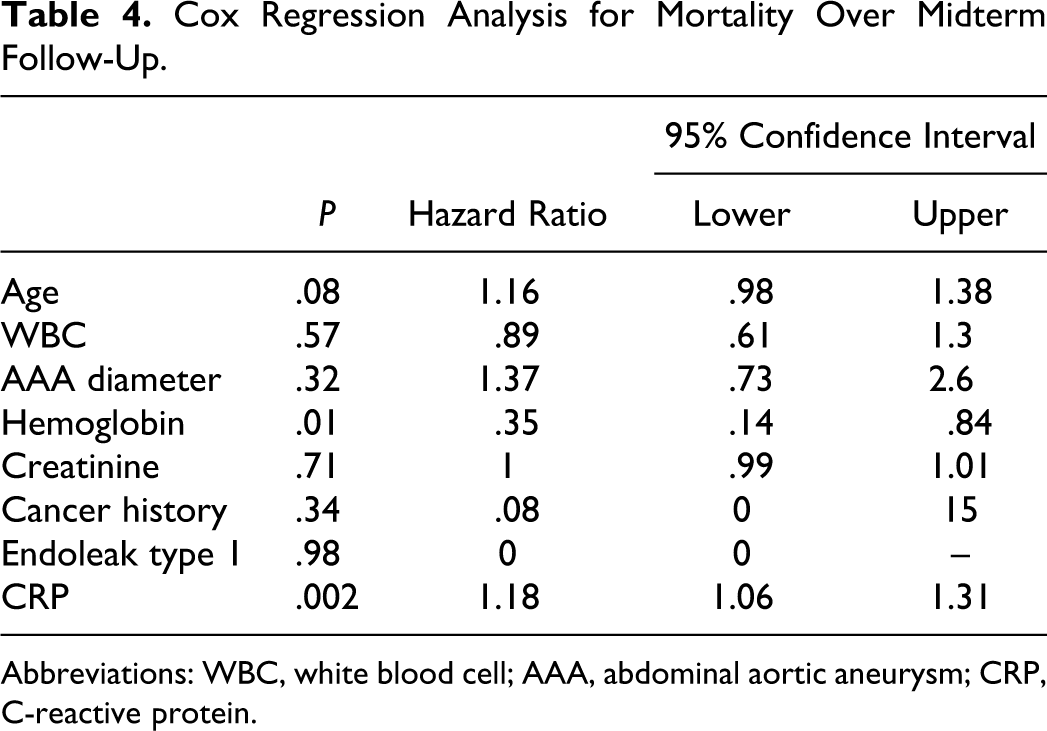
Abbreviations: WBC, white blood cell; AAA, abdominal aortic aneurysm; CRP, C-reactive protein.
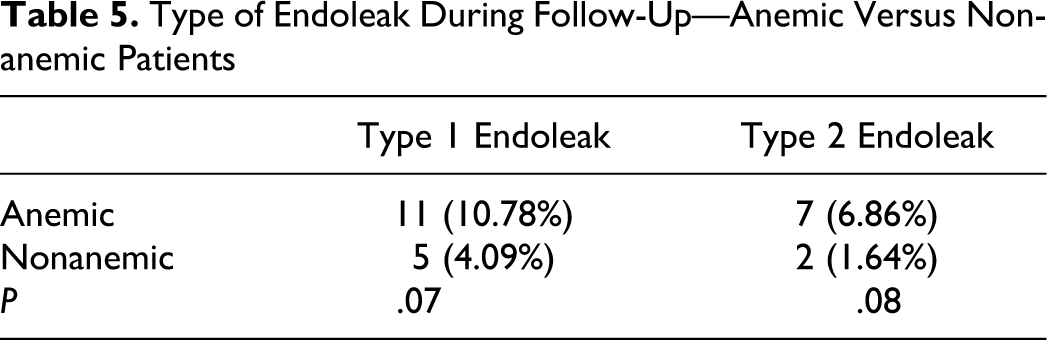
Regarding device-related complications, no perioperative graft migration or kinking was noted. Two (2 of 224 [0.88%]) type 1 endoleaks occurred perioperatively, treated successfully with the deployment of an endovascular cuff. Over the whole follow-up period, 16 patients (7.1%) developed type 1 endoleak (proximal or distal) and 9 (4%) developed type 2 endoleak; none of the patients with type 2 endoleak required further intervention. Four of the patients with type 1 endoleak were converted to open repair. The incidence of endoleak (both types 1 and 2) did not differ significantly between anemic and nonanemic patients (Table 5). One patient developed small bowel ischemia and died (36 months); abdominal computed tomography (CT) with contrast revealed no device migration, kinking, or aortic dissection prior to his death. One patient died due to tense malignant ascites at 12 months; no device-related complications were noted on an abdominal CT scan prior to his death. No further device-related complications were noted throughout follow-up.
Type of Endoleak During Follow-Up—Anemic Versus Nonanemic Patients
Discussion
This study suggests that anemia at baseline may be a negative predictive factor for patients undergoing EVAR, with regard to midterm mortality. Baseline WBC and CRP were found to differ significantly between anemic and nonanemic patients, and CRP was also associated with decreased survival. This suggests a higher inflammatory state among these individuals that may be related to outcome.
The advent of EVAR during the last 2 decades has meant that patients with greater comorbidity are now being offered elective repair because the technique requires significantly less operating time, and perioperative complications are decreased, compared with open reconstruction. 4 Obviously, this group of frailer patients are at increased risk of postoperative complications relating to underlying comorbidity. 4 Therefore, it is essential to identify those at highest risk prior to offering repair.
Anemia has traditionally been associated with chronic disease 9 and inflammatory states, where increased concentrations of hepcidin (an important regulator of iron homeostatis) cause iron sequestration in macrophages, resulting in anemia. 8,9,16 Additionally, the circulating inflammatory cytokines further induce hypoferremia and, therefore, anemia, as they promote iron metabolism and iron uptake from macrophages. 17,18
Anemia has also been identified as a predictor of morbidity and mortality in patients with ischemic heart disease, heart failure, and chronic renal dysfunction. 9,19,20 Additionally, it has recently been shown that anemia predicts mortality following surgery for colorectal cancer, endovascular intervention for peripheral arterial disease, open vascular reconstruction, and coronary artery bypass grafting. 21 –23 In fact, a recent study has suggested that the presence and severity of preoperative anemia in vascular patients are significant predictors of 30-day and 5-year cardiac events, regardless of underlying heart failure or renal disease. 24 The morbidity and mortality observed in this current series cannot be directly linked to technical issues associated with EVAR, as none of these patients had a proven migration, endoleak, or other significant device-related complication. This means that patients with anemia are at increased risk of developing severe postoperative complications not related to the procedure itself but probably secondary to their comorbidities and other factors, such as increased inflammation. This calls for a more scrutinizing medical assessment of this patient group at baseline to identify this comorbidity and correct it. In any case, we do not believe that these patients should not be offered repair but more attention is needed to avoid an unfavorable outcome.
Despite the fact that there is a clear causative relation between inflammation and anemia, most of the studies investigating hemoglobin concentration as a predictor of outcome following various surgical interventions did not demonstrate elevated inflammatory markers among the anemic individuals. A previous study by Diehm et al that documented a link between anemia and mortality after EVAR also failed to disclose significantly higher inflammatory markers among patients with anemia having AAA; however, hemoglobin was independently associated with aneurysmal diameter. 6 It is worth noting that AAA size has also been shown to independently correlate with circulating inflammatory markers, namely interleukin 6 and CRP. 25 In our series, patients with anemia did differ significantly in terms of markers of inflammation (CRP and WBC), and CRP was also associated with decreased survival on multivariate analysis, which supports the assumption that anemia is, indirectly, a marker of increased inflammation in aneurysmal disease of the abdominal aorta. Patients with aneurysmal disease in locations other than the aorta were not included in this analysis, as this could be a confounding factor when trying to correlate AAA and inflammatory markers. It is unclear whether Diehm et al 6 did exclude patients with aneurysms in other locations from their analysis.
Others markers of inflammation, such as erythrocyte sedimentation rate or circulating cytokines, were not analyzed in this series, as the aim of the study was to use laboratory tests performed in routine clinical practice.
Another important issue is the kind of morbidity that is associated with EVAR, which includes device-related complications such as endoleak and migration. Nordon et al 26 performed a meta-analysis of 17.987 EVAR cases and reported a crude annual secondary intervention rate of 6% per year for the EVAR trials and 3.7% per year (median) for the case series that have been published following the EVAR trials. This is different from the morbidity encountered following open reconstruction, where patients are more prone to complications related to increased blood loss and operating time. 27 In this series, a total of 2 type 1 endoleaks (2 of 224 [0.88%]) occurred perioperatively and over the whole follow-up, 16 patients (7.1%) developed a type 1 endoleak (proximal or distal). Despite that the deaths that have occurred were mostly related to comorbidity (Table 2) and not directly to technical issues, such as endoleak. Also, the incidence of endoleak did not differ significantly between anemic and nonanemic patients (Table 3). The anatomy of the proximal neck was comparable between the 2 groups, as reflected by the fact that the number of patients with a device with a suprarenal proximal fixation mechanism was deployed was equal among groups.
Limitations
The first limitation of the study is the fact that inflammatory markers could only be correlated with the aneurysmal diameter and not the sac clot content and volume, due to the design of the analysis (3D reconstruction data not collected prospectively at baseline for all patients). Additionally, it was not possible to correlate sac shrinkage with reversal of anemia over the follow-up, as this was not part of the initial protocol. Finally, the follow-up was limited to midterm (median: 17 months). Long-term data are not yet available.
However, the prospective nature of the study and the exclusion and adjustments for factors that could influence the incidence of anemia (age, sex, history of cancer, exclusion of patients with aneurysmal disease at other locations, and end-stage renal failure) are relative advantages of this analysis compared with previous studies.
This study suggests that anemia at baseline may be a negative predictive factor for patients undergoing EVAR. The CRP was also associated with decreased survival. Chronic inflammation is likely to be the explanation for the relation between anemia and worse outcome. Patients with anemia should undergo more thorough screening at baseline to identify the associated comorbidity that could lead to a negative outcome.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.