
Abstract
We report our single-center experience in treating 101 type II endoleaks with ethylene-vinyl-alcohol copolymer (EVOH, Onyx). In all, 65 endoleaks were embolized transarterially, and 36 were treated through a translumbar approach. Since the first transarterial embolization, when we began attempts to treat all patients initially via common femoral access, 58 (65.9%) of 88 patients were successfully embolized transarterially. All endoleaks in the translumbar group were successfully treated. At a median follow-up length of 15 weeks, a decrease or stabilization in aneurysm size was observed in 39 (73.6%) of the 53 endoleaks that had adequate follow-up computed tomography imaging. The overall residual endoleak rate was 34.0%. There was no difference in efficacy when comparing transarterial and translumbar approaches. We demonstrate that in most cases, transarterial access of the endoleak nidus is feasible, and controlled embolization is possible using EVOH. Furthermore, EVOH appears effective in long-term stabilization of aneurysm size and in preventing residual endoleaks.
Introduction
The rising trend of endovascular repair of abdominal aortic aneurysms (EVAR) has produced a new dilemma of endoleak management. Defined as persistent blood flow into the aneurysmal sac, endoleaks are the most common complication associated with EVAR. 1,2 The most prevalent of the 5 types is a type II endoleak (having an incidence of 6%-17% up to 30 days post-EVAR 3 ), where there is persistent flow into the aneurysm sac from 1 or more collateral vessels, such as the inferior mesenteric artery (IMA) and lumbar artery. There is some controversy regarding the optimal management of type II endoleaks. Some physicians advocate definitive occlusion of all type II endoleaks because the leaks can allow transmission of systemic arterial pressure into the aneurysm and can therefore promote sac rupture. 4 However, others choose surveillance in the setting of a stable aneurysm sac size, relying on the fact that small type II endoleaks can seal spontaneously. 5 The understated secondary effect of type II endoleaks causing aneurysm sac enlargement is the development of delayed type I endoleaks, which further justifies the treatment of type II endoleaks.
A variety of techniques have been employed to treat type II endoleaks, including laparoscopic ligation of the IMA or lumbar arteries, 6 transarterial coil embolization of feeding vessels, 7 –9 translumbar coil embolization of the endoleak nidus, 10,11 and injection of liquid embolics or thrombin into the nidus. 12,13
In the present study, we report our single-center experience with using ethylene-vinyl-alcohol copolymer ([EVOH] Onyx, ev3 Inc, Plymouth, Minnesota) to treat both simple and complex type II endoleaks. Martin et al 14 previously reported successful translumbar embolization of 5 type II endoleaks using EVOH.
In the beginning of our experience using EVOH, we exclusively treated type II endoleaks using a translumbar approach. However, the transarterial route seemed technically feasible and since our first case, we have transitioned and always attempt treatment via a transarterial route. The other developing technique used more often at our institution is accessing the endoleak channel around the iliac stent graft, even without the presence of a type Ib endoleak.
Methods
A retrospective review of procedures conducted at our institution from August 1, 2006 to June 8, 2011 revealed that we repaired 101 type II endoleaks in 95 patients (6 patients had 2 separate type II endoleak repairs) using EVOH. Institutional approval was granted for this retrospective review. Study criteria included all patients with endoleak post-EVAR. Patients found to have type I or type III endoleaks were excluded. Treatment for the type II endoleak was deemed necessary because the patient’s abdominal aortic aneurysm (AAA) met one of the following criteria for treatment: aneurysm sac growth of 5 mm or more within a 6-month period, aneurysm sac greater than 6 cm in diameter, change in aneurysm sac morphology, or change in position or orientation of stent graft in the aneurysm sac. Among these patients, 89 (93.7%) were male and 6 (6.3%) were female. Mean patient age was 77.6 years (range = 63-93 years).
Prior to the endoleak repair, diagnostic angiography was performed to further characterize the endoleak and to determine the involved vessels. Abdominal aortogram followed by selective arteriogram of the superior mesenteric artery (SMA), common iliac, and hypogastric arteries were performed. Depending upon the degree of suspicion, selective middle colic and/or iliolumbar arteriograms were also performed.
If there was a feasible transarterial route via collateral pathways to the endoleak channel within the aneurysm sac, then a transarterial embolization was attempted. If there was incomplete apposition of the iliac limb of the stent graft to the iliac artery wall, then an attempt was made to track a hydrophilic wire and catheter directly into the aneurysm sac between the stent graft and iliac artery wall. Once the aneurysm sac was accessed, the endoleak channel was catheterized, followed by digital subtraction angiography (DSA) to assess the involved vessels. Once the microcatheter was within the endoleak channel in the aneurysm sac, embolization was performed with EVOH (see Figure 1).
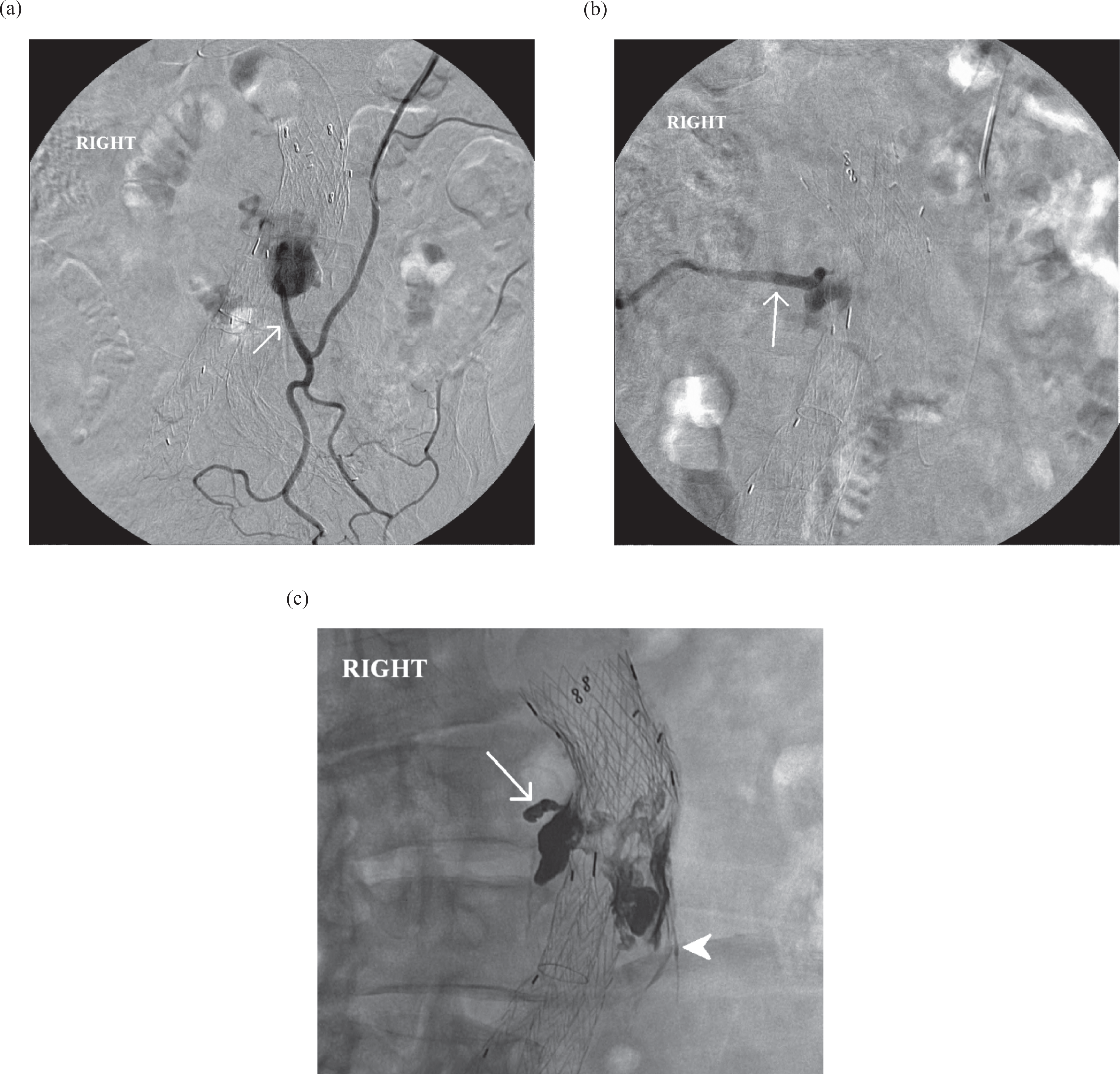
A, Digital subtraction angiography (DSA) showing selective left colic arteriogram via SMA/middle colic artery access. There is retrograde filling of the IMA (arrow) back to the aneurysm sac, opacifying the endoleak nidus. B, DSA directly into the endoleak nidus from the IMA reveals the presence of an outflow right L3 lumbar artery (arrow). C, Digital radiograph after EVOH embolization. EVOH fills the endoleak nidus and was intentionally extruded into the origins of both the IMA (arrowhead) and the right L3 lumbar artery (arrow). SMA indicates superior mesenteric artery; IMA, inferior mesentric artery; EVOH, ethylene-vinyl-alcohol copolymer.
The goal of embolization was to completely occlude the channel of flow and the involved vessels. Intentional extrusion of EVOH into the origins of the involved vessels was ideal. Coil embolization of the entry vessels was also performed if EVOH did not adequately extrude into the vessel used to enter the aneurysm sac.
If a direct route to the endoleak nidus was not achievable, a translumbar sac puncture and embolization was performed, usually on the next day.
Translumbar Approach
Patients were placed in the prone position and general endotracheal anesthesia was administered. General anesthesia was preferred because of the difficulty in lying prone for a prolonged period in our population due to their advanced age and comorbidities and airway protection. Computed tomography (CT) images for each patient were reviewed in order to determine the optimal entry point, angle, and depth for sac puncture. Using fluoroscopic guidance and anatomical landmarks, a 21-gauge styleted needle was used to directly access the aneurysm sac at or near the nidus of the endoleak, typically from a left paraspinal approach. If the endoleak nidus was not directly accessible, such as a predominately anterior or superior endoleak nidus, then remote access was obtained and the nidus was located with a coaxial system using anatomical landmarks. Upon pulsatile blood return, DSA was performed to localize the nidus and feeding vessels. After placement of a vascular sheath and 4F or 5F macrocatheter, embolization was then performed using EVOH through a DMSO-compatible microcatheter (Echelon or Rebar, ev3 Inc.) until the nidus was casted. If the IMA was involved in the endoleak and easily catheterized, protective coil embolization was performed prior to liquid embolization. Again, ideally EVOH would be intentionally extruded into the culprit vessel origins and not only in the channel of flow within the aneurysm sac (see Figure 2).
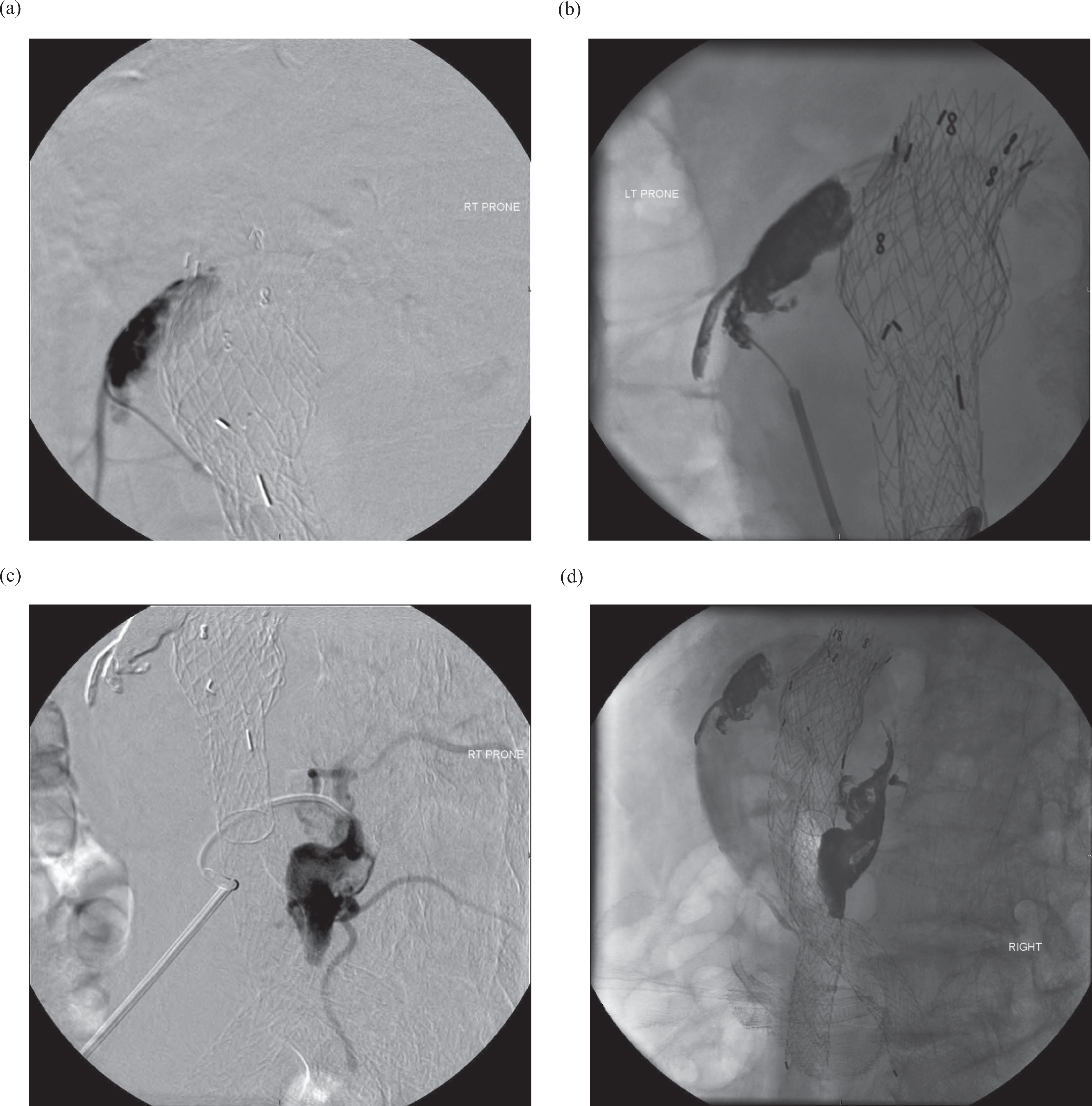
A, Direct translumbar puncture and DSA of the endoleak nidus demonstrates communication with the IMA but no flow to the suspected lumbar arteries. B, Digital radiograph after EVOH embolization to stasis and with intentional extrusion to the IMA. C, Second sac puncture into the inferior aspect of the endoleak nidus, with arteriogram showing L3 and L4 lumbar arteries communicating. D, Digital radiograph after EVOH embolization of both endoleaks shows a similar appearance to the DSA. DSA indicates digital subtraction angiography; EVOH, ethylene-vinyl-alcohol copolymer.
After embolization was completed and stasis was confirmed, an EVOH plug was formed in the sheath and deployed across the entry site in the aneurysm sac wall.
Results
Table 1 illustrates the arteries that contributed to the type II endoleaks in our study. The IMA, L3 lumbar artery, and L4 lumbar artery were the most likely culprits, respectively, contributing to 47.5%, 43.6%, and 52.5% of the 101 type II endoleaks. Table 2 demonstrates the transarterial course used to gain access to the endoleak channel; the SMA-middle colic-IMA and hypogastric–iliolumbar–lumbar collateral pathways were the most frequently used. In our later cases, we began to use the more direct access between the common iliac artery wall and iliac limb of the stent graft. Even without a demonstratable distal type Ib endoleak, this route was commonly possible. Even the smallest zone of incomplete apposition between the stent graft and iliac artery would allow the passage of a hydrophilic wire and catheter into the aneurysm sac. Patients with demonstrated type Ib endoleaks or inadequate distal seal length would go on to iliac stent graft extension.
Rate of Involvement of Various Aortic Branch Vessels in Feeding Type II Endoleaks
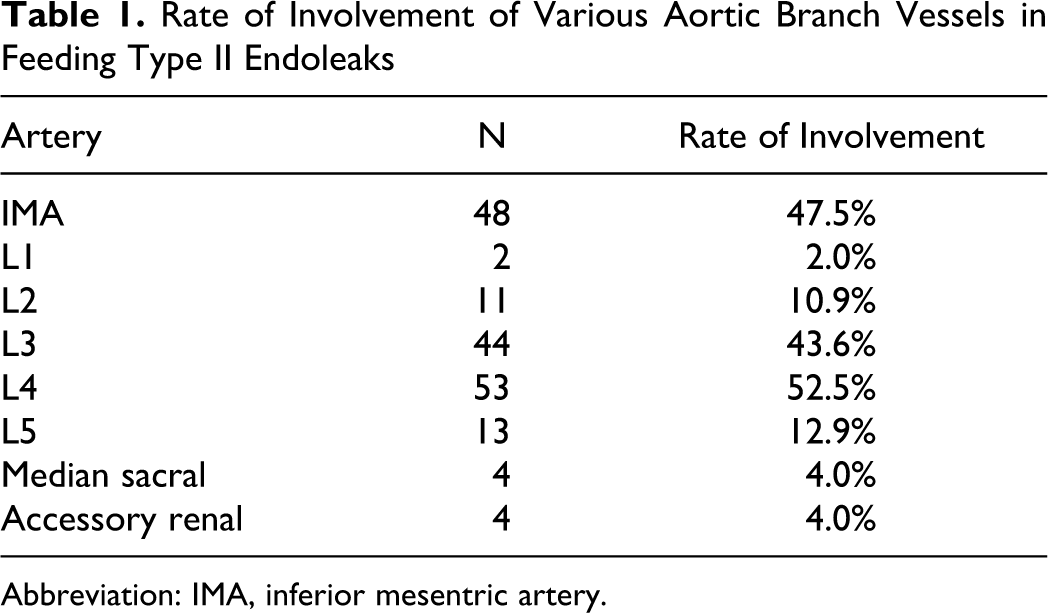
Abbreviation: IMA, inferior mesentric artery.
Transarterial Courses Utilized to Access Endoleak Channel
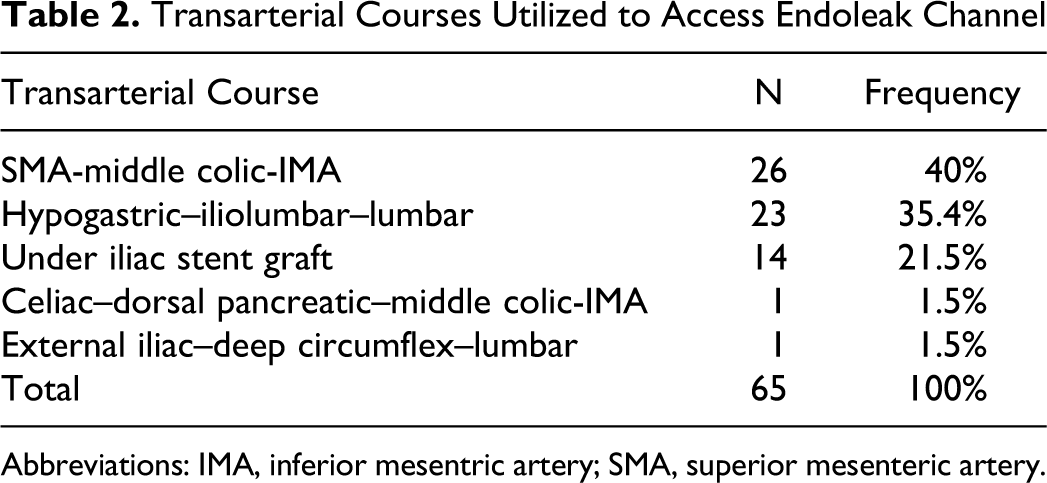
Abbreviations: IMA, inferior mesentric artery; SMA, superior mesenteric artery.
A total 65 (64.4%) of the endoleaks were embolized through a transarterial approach, and 36 (35.6%) were treated through a translumbar approach. Since the first transarterial embolization, when we began attempts to treat all patients initially via common femoral access, 58 (65.9%) of 88 patients were successfully treated via transarterial route. However, in our last 13 cases, 12 (92.3%) were successfully embolized transarterially. Technical success for both transarterial and translumbar embolization was defined as elimination of flow to the aneurysm sac. All of the endoleaks in the translumbar group were successfully accessed and complete embolization was achieved in all cases. No major complications were experienced in either group.
Out of the 101 type II endoleaks that were analyzed in this study, adequate pre- and post-embolization CT imaging was available for 53 (52.5%) of them. Median follow-up length was 15 weeks. Aneurysm size was assessed by measuring both the long and short axes of the aneurysm sac at the point of maximal dilatation and then calculating the corresponding elliptical area using these 2 values (area of an ellipse = лab, where a = semimajor axis and b =semiminor axis). A decrease or stabilization (≤1 cm2 increase) in aneurysm sac size was observed in 39 (73.6%) of the 53 endoleaks, while a >1 cm2 increase in sac size was seen in the remaining 14 (26.4%). The overall residual endoleak rate was 34.0% (see Table 3). For the endoleaks embolized transarterially, 21 (72.4%) out of 29 displayed a decrease or stabilization in sac size, and the residual endoleak rate was 41.4% (see Table 4). For those treated via a translumbar approach, 18 (75.0%) out of 24 displayed a decrease or stabilization in sac size, and the residual endoleak rate was 25.0% (see Table 5). There was no significant difference in efficacy in regard to either aneurysm sac behavior (t = 0.13, P = .90) or the residual endoleak rate (chi-square analysis, P = .21) when comparing transarterial and translumbar approaches.
Follow-Up Imaging Data for All Type II Endoleaks a
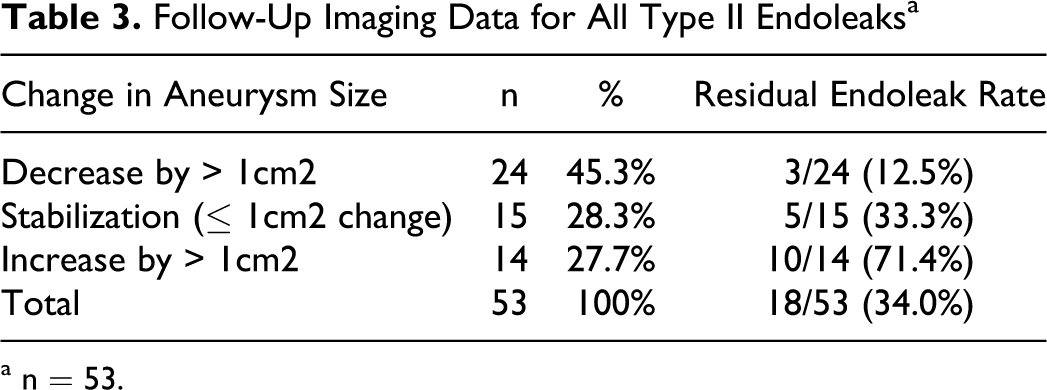
a n = 53.
Follow-Up Imaging Data for Transarterial Embolizations a
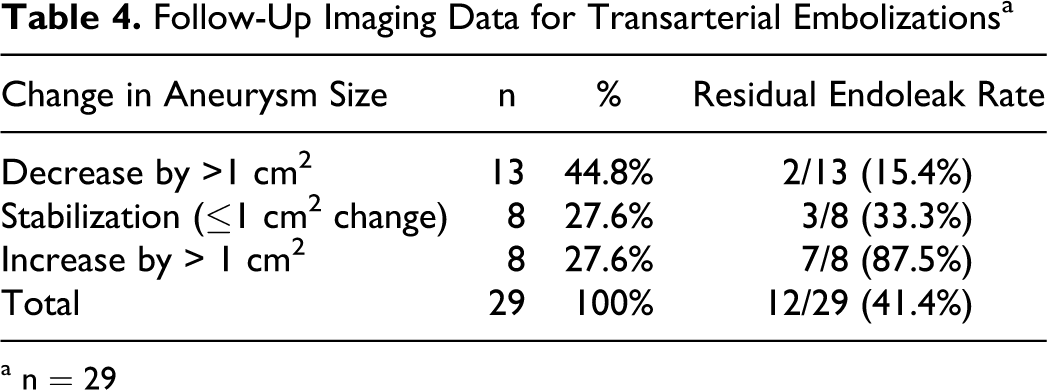
a n = 29
Follow-Up Imaging Data for Translumbar Embolizations a

a n = 24.
Discussion
One of the limitations of EVAR is the emerging issue of endoleak management, with the greatest incidence being the type II endoleak. There have been a number of reported cases of AAA rupture after EVAR with known type II endoleaks. 15 More significant, in the opinion of the authors, is the persistence of sac pressurization from type 2 endoleaks that can lead to enlargement of the AAA sac, degeneration of the aneurysm neck, and/or a change in position of the stent graft within the AAA sac. These occurrences may ultimately lead to a secondary type I endoleak which places the patient at higher risk for rupture. 16
Over the last 10 years, a number of different techniques have been utilized to treat type II endoleaks. One of the first approaches was transarterial coil embolization of the endoleak feeding vessels (usually the IMA or Iliolumbar artery). 7 –9 Although this method appeared successful at the time of embolization, Baum et al 11 found that 80% of type II endoleaks that were treated in this fashion ultimately recanalized over time. Later, type II endoleaks were thought to behave more like arteriovenous malformations, able to recruit multiple inflow and outflow vessels, with the portion of the endoleak within the aneurysm sac referred to as the “nidus.” Coil embolization of a single feeding vessel is largely ineffective due to the redistribution of blood flow through the other collateral vessels such as the lumbar arteries, thereby continuing to supply the nidus and pressurize the aneurysm sac.
Other practitioners have treated type II endoleaks with retroperitoneal endoscopic ligation of the involved vessels. 6 However, in order for this technique to be effective, virtually every aortic branch supplying the aneurysm sac must be ligated (eg, the IMA and all lumbar arteries) to avoid recruitment of additional collateral vessels by the endoleak. Thus, because of this dynamic redistribution of flow, laparoscopic ligation of individual vessels will exhibit the same ineffectiveness as transarterial coil embolization of these same vessels. In one study, Wisselink et al 6 laparoscopically ligated the IMA as well as 3 pairs of lumbar arteries that were feeding a type II endoleak, only to observe on a postoperative CT angiography that they had missed another pair of lumbar arteries that were feeding the endoleak.
After the ineffectiveness of the previous techniques had been demonstrated, direct translumbar embolization of the endoleak cavity itself began to be utilized. It was realized that embolization of the endoleak nidus was an absolute necessity in order to prevent recanalization. Initially, this was done entirely with coils, 10,11 but coil embolization of the endoleak nidus was also fraught with recannalization through the interstices of the coils. Also, embolization of the entire endoleak cavity with coils can be very time consuming. As a result, liquid embolic agents such as n-butyl 2-cyanoacrylate (NBCA) and thrombin began to be used to embolize the nidus. 12,13 The NBCA has the ability of forming a more complete cast of the endoleak nidus and usually causes less artifactual interference on follow-up imaging than coils. However, treating type II endoleaks with NBCA is difficult in that the glue must be injected rapidly in order to prevent catheter occlusion. This rapid speed of injection increases the risk of ischemic complications that can occur due to nontarget embolization of downstream vessels. After embolization with NBCA, often the catheter needs to be removed quickly in order not to be “glued” in place. If the embolization was then deemed incomplete, it may be extremely tedious or impossible to regain access to the endoleak nidus to complete the embolization. Thrombin proved to have limited use due to the poor long-term results secondary to recannalization. 17 EVOH, on the other hand, has the ability to be delivered through a DMSO-compatible microcatheter in a slower and more controlled manner, effectively decreasing the risk of nontarget embolization. The more controlled delivery method also allows the operator to intentionally “grow” EVOH into the involved inflow and outflow vessels in order to completely occlude all the vessels communicating with the endoleak nidus. In our experience, we have found that persistent type II endoleaks may result from incomplete embolization of not only the nidus but also the supplying branches.
Over the last 4 years, we have had extensive experience with management of type II endoleaks through both translumbar and transarterial approaches. Initially, we heavily favored the translumbar approach, from August 1, 2006 to October 8, 2007, 12 (80.0%) out of 15 type II endoleaks that we encountered were treated through direct translumbar sac puncture. After the initial success of accessing the endoleak nidus with the use of coaxial systems and flexible microcatheters, we demonstrate that the transarterial route to access and embolize the endoleak was feasible and successful in about 70% of cases. Technical failures were most often due to the length and tortuosity of collateral pathways or the small caliber of the collateral vessels. In cases where the transarterial route of accessing and treating the endoleak was unsuccessful, 100% of the cases were successfully accessed and treated via the translumbar route.
The advantages of the transarterial approach included the fact that there was no need for general anesthesia for airway control and the ability to perform both the diagnostic and therapeutic intervention in the same setting. Over the years, microcatheter/wire technology has significantly improved and advanced coaxial and triaxial catheter techniques were utilized to obtain direct transarterial access to the nidus. In our most recent experience, the retrograde perigraft access between the iliac artery wall and stent graft to the endoleak nidus became a favored approach having been performed in 63% of our last 15 cases.
Regarding the long-term clinical efficacy of EVOH, 39 (73.6%) of the 53 type II endoleaks that had adequate pre- and post-embolization CT scans showed a decrease or stabilization in aneurysm sac size at a median follow-up length of 15 weeks, with a residual endoleak rate of 34%. We chose to use area rather than maximal diameter when assessing aneurysm size because many aneurysms either grew or shrunk along their short axis. Furthermore, there was no significant difference in efficacy in regard to either aneurysm sac behavior or residual endoleak rate when comparing transarterial and translumbar approaches.
It is the opinion of the authors that the AVM model of endoleaks is inaccurate. The embolization of endoleaks requires the same approach as the treatment of a branched aneurysm. The endoleak nidus is not the impetus to flow, it is the involved vessels. The ideal goal of embolization should be to not only achieve total occlusion of the channel of flow within the aneurysm sac, but also the origins of all the involved vessels. The ideal agent would achieve this goal. This agent would be delivered in a controlled fashion with decreased risk of nontarget embolization. EVOH satisfied some of these elements but has significant limitations. EVOH is quite expensive, with limited availability, and creates an intense streak artifact that degrades the follow-up CT imaging.
Conclusion
EVOH is currently the best available liquid embolic agent for the treatment type II endoleaks. We have demonstrated that in our experience, the transarterial approach of embolization using small caliber flexible microcatheters is technically feasible with regard to accessing the endoleak nidus and controlled liquid embolization is possible with EVOH. Furthermore, EVOH appears to be effective in long-term stabilization of aneurysm sac size as well as in preventing residual endoleaks.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.