
Abstract
Traumatic nonanastomtic disruption of an axillofemoral bypass graft (AFBG) is a relatively rare entity. However, we are reporting on an 82-year-old female who presented with a pulsating mass on her left side, which was noticed about 2 weeks after she fell on her side. The patient had undergone an ABFG about 15 years earlier for limb revascularization, and she had an occluded aortobifemoral bypass graft. A diagnosis of localized rupture with pseudoaneurysm (PSA) was confirmed with arterial duplex ultrasound and computed tomograph (CT) angiogram scans. A 7-cm PSA with partial disruption of the polytetrafluoroethylene (PTFE) graft at the level of the fifth thoracic vertebrae was noted. An initial work-up to eliminate the possibility of sepsis and localized mycotic seeding was negative. The patient was taken to the hybrid angiogram room, and a percutaneous cut down of the AFBG was performed with local dissection below the site of rupture. A limited angiogram showed a focal PSA of the AFBG. An intravascular ultrasound (IVUS) was performed to calibrate the diameter of the AFBG, and a covered stent was deployed across the area of the disrupted graft. A completion angiogram showed complete exclusion of the PSA with good runoff throughout the graft. The authors will review the management of the traumatic PSA with an endovascular approach.
Introduction
The axillofemoral bypass graft (AFBG) was first pioneered by Blaisdell in 1963 and continues to be a viable option for lower extremity occlusive disease in selected patients. 1 Indications for an AFBG are a hostile abdomen, multiple previous abdominal surgeries, a prohibitive risk to general anesthesia, and severely sick patients. The configuration for an AFBG is either bifemoral or unifemoral, and the graft material to be used is either Dacron or polytetrafluoroethylene (PTFE). The 5-year patency rate for an AFBG is estimated to be 60% to 70%. 2 Spontaneous degeneration and aneurysm formation of these grafts of the extremity are extremely rare, however it is well-documented in case reports. 3,4 This case report describes a traumatic pseudoaneurysm (PSA) at the mid-shaft of the AFBG and outlines the feasibility of endovascular treatment in such scenarios.
A Case Report
An 82-year-old female presented to our institution as a transfer from another facility with a pulsating mass in the left torso 2 weeks after a fall on her left side. She had about a 5 cm pulsating mass along the side of the AFBG. She had undergone an AFBG about 10 years earlier for lower limb revascularization with an 8-mm, reinforced, thin-walled, fluorinated ethylene-propylene-ringed, expanded polytetrafluoroethylene (ePTFE) graft. On examination, there was a painful mildly tender mass at the mid-shaft level of the AFBG at the level of the nipple line. There were no symptoms of localized or diffuse sepsis. The patient denied any history of fever or infection. Her vital signs were within normal values, and her physical examination revealed a 5-cm pulsating mass along the course of the graft, with no localized or systemic signs of sepsis.
The patient’s past medical history was significant for coronary artery bypass graft surgery, hypertension, ejection fraction of 25%, and a failed aortobiiliac graft. An arterial duplex study showed a 5-cm PSA, and the diagnosis was confirmed by a computed tomography (CT) angiogram (Figure 1 A and B). A white blood cell scan and blood cultures were negative.
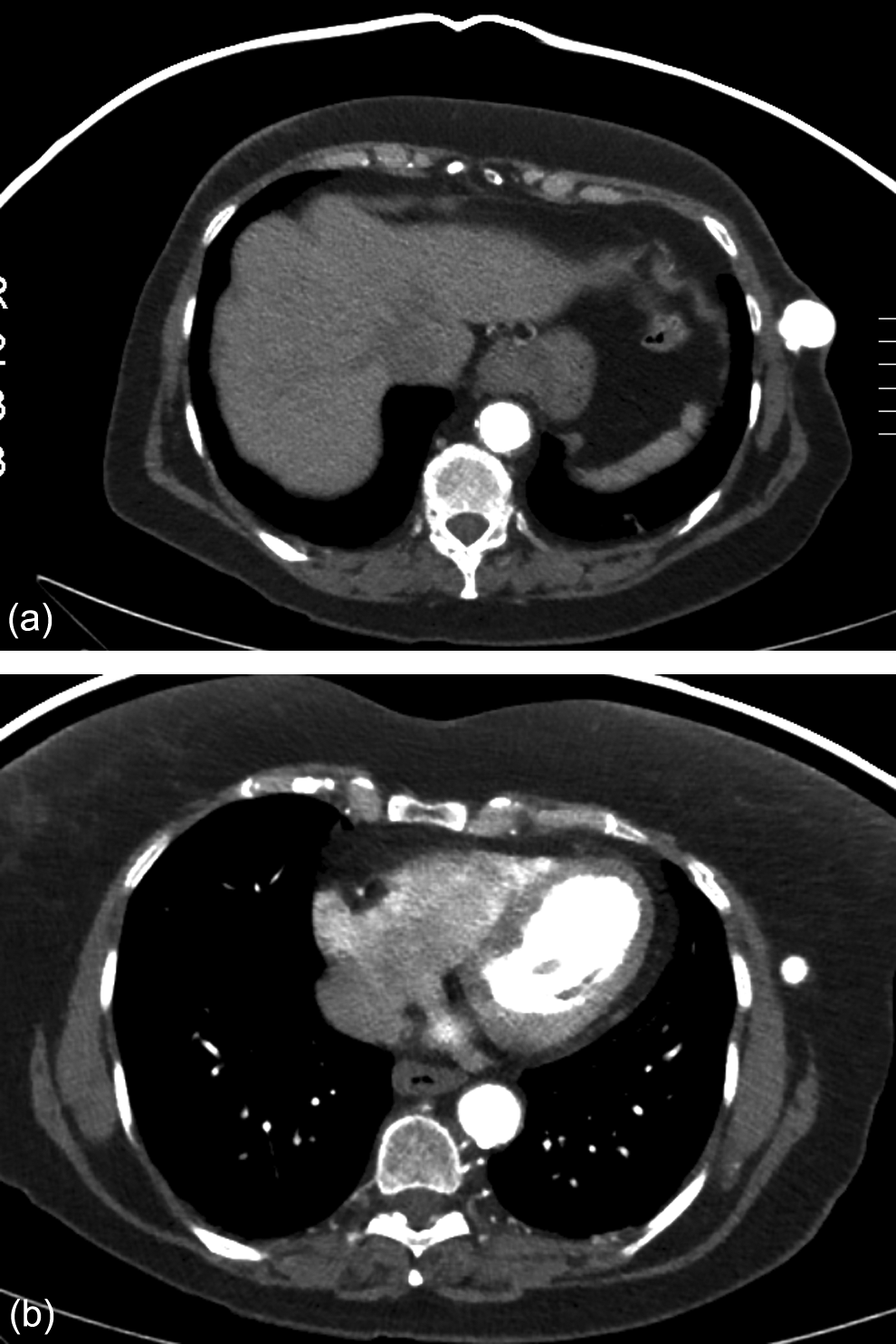
Computed tomograph (CT) angiogram of chest abdomen, and pelvis, axial views demonstraded axillofemoral bypass graft (AFBG) pseudoaneursym (A) and adjacent normal graft segment (A).
Due to the multiple prohibitive medical conditions, we opted to treat this patient with endovascular exclusion of the PSA. Preoperative antibiotics were given, then under local anesthesia with lidocaine and conscious sedation, a transverse incision of 2 cm and a cut down over the lower one-third of the AFBG was made at the level of the iliac crest. Proximal and distal control was achieved with vessel loops and then weight-based heparin was given for anticoagulation. A 9-F sheath was placed and an initial AFBG angiogram was preformed (Figure 2), and the area of the graft disruption was delineated. An intravascular ultrasound (IVUS) was used to precisely calibrate the size of the graft proximal and distal to the area of graft disruption (Figure 3 A and B). A 9 mm diameter and 100 mm length covered stent (VIABAHN, W. L. Gore & Associates, Inc, Flagstaff, Arizona) was deployed successfully over the area of disruption in the AFBG. A final completion angiogram demonstrated complete exclusion of the PSA with a brisk distal outflow (Figure 4). Postoperatively, the patient was placed on clopidogrel, 75 mg orally (PO) daily as well as her statin. The patient had an uneventful outcome, and she was discharged home on postoperative day 1. A 3-month follow-up arterial duplex demonstrated patent graft with no evidence to pseudoaneursm.
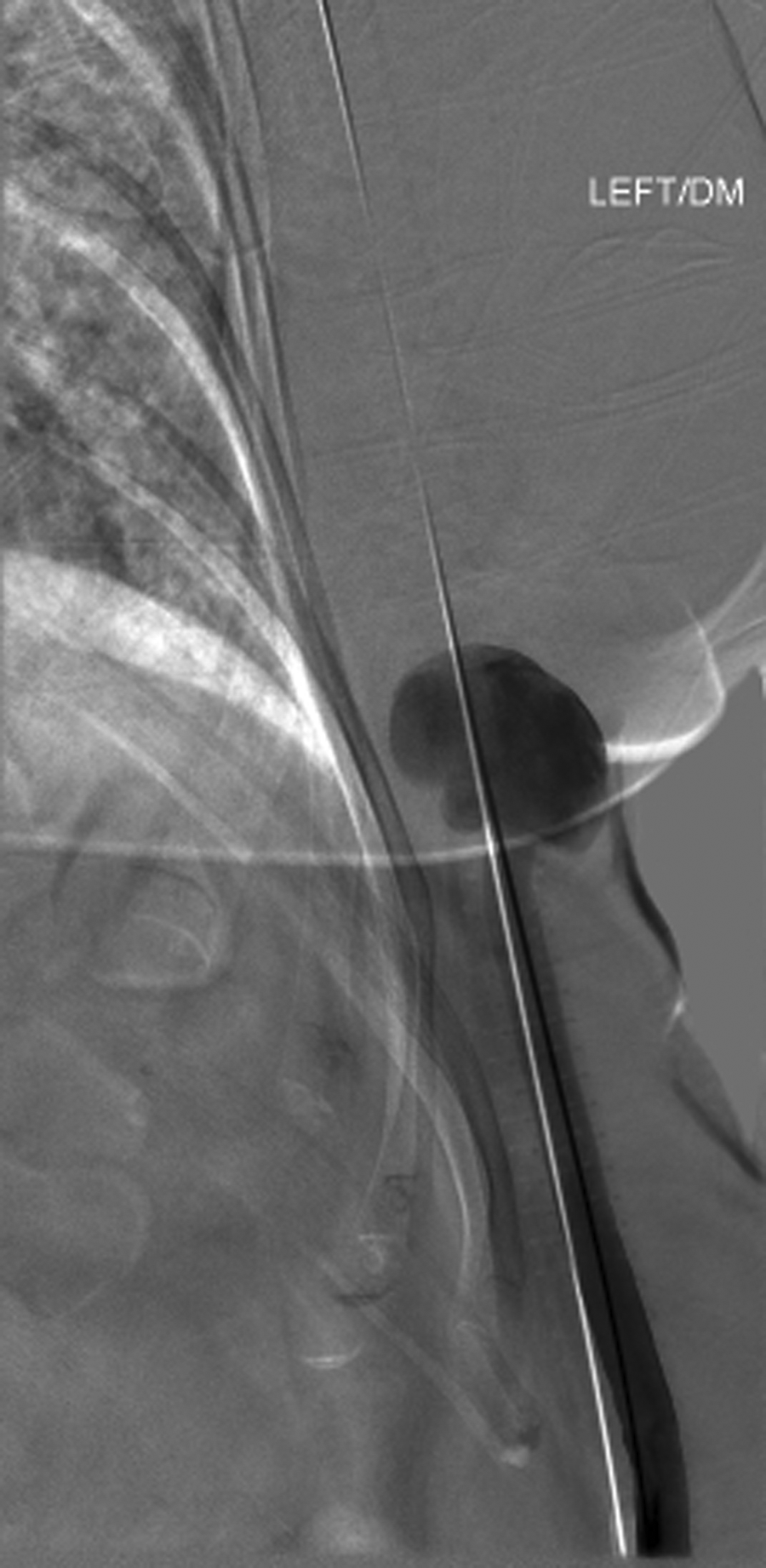
An angiogram demonstrating a pseudoaneurysm of the mid-shaft of the axillofemoral graft. Note a guide wire was placed across the area of the pseudoaneurysm.
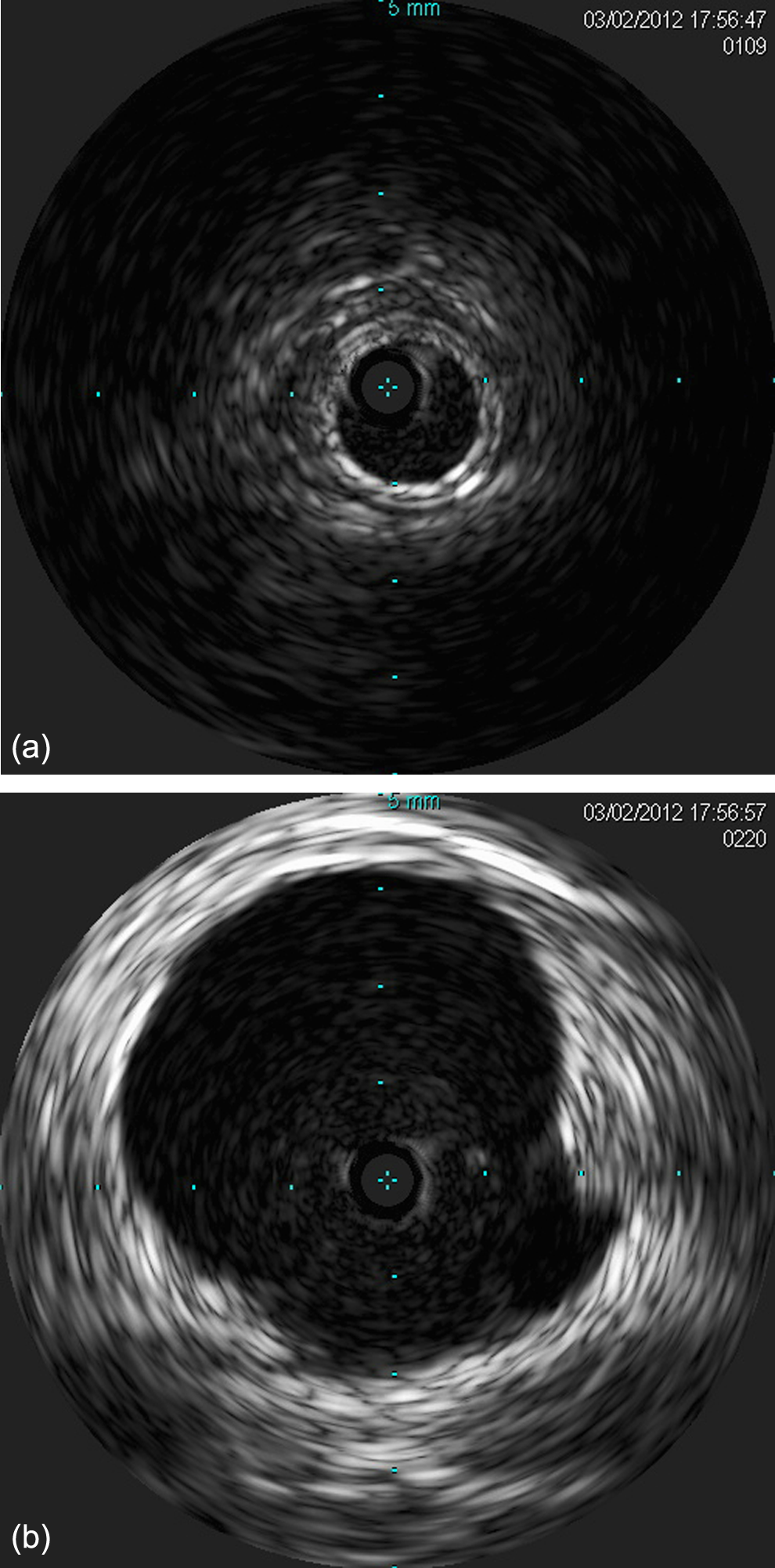
Intravascular ultrasound (IVUS) demonstating normal caliber graft area proximal to the pseudoaneurysm (A), prestenting IVUS image to demonstrate the area of outpouching of the pseudoaneurysm(B).
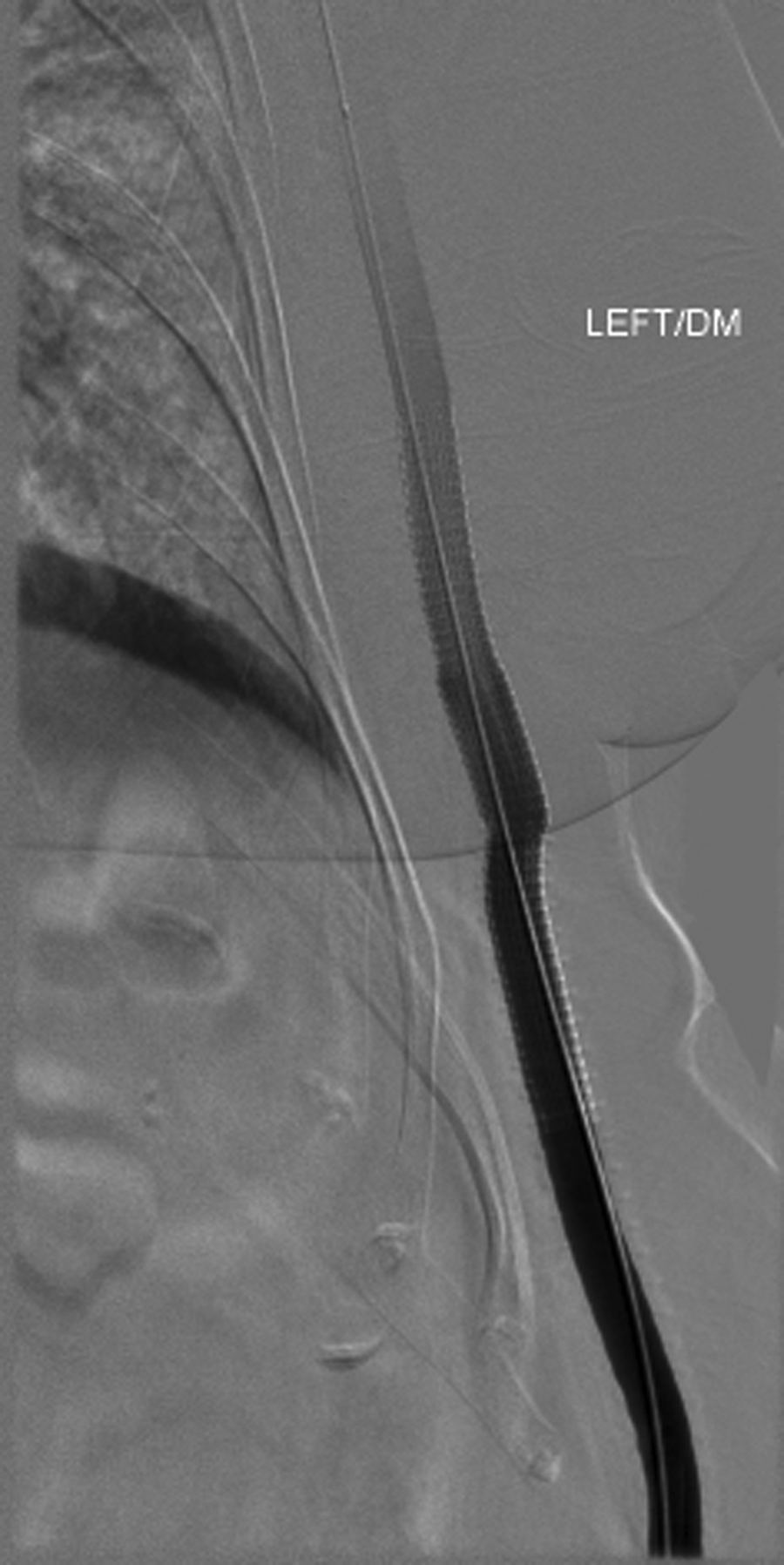
Completion angiogram showing complete exclusion of the pseudoaneurysm with good runoff to distal axillofemoral graft.
Discussion
There are only a few cases of nonanastomotic aneurysms related to AFBGs in the literature. 3 –8 An AFBG can be done alone or in conjunction with a femorofemoral bypass, and it is considered to be one of the most common extra-anatomical surgeries for lower limb revascularization. This technique has some important benefits, such as avoiding aortic clamping and the morbidity and mortality associated with traditional aortobifemoral graft surgery. An additional benefit is that the procedure can be performed under local anesthesia. All of these advantages make this operation more appealing in patients with significant cardiovascular comorbidities, who are in need of revascularization. The only trade off is a lower patency rate for ABFG, in comparison to 5-year patency rates for aortobifemoral bypass, which range from 35% to 71%. 9,10
Some reports have indicated that externally supported PTFE grafts are associated with an improved patency rate with less kinking/compression, secondary to the external support of the rings. 10,11 Although it is extremely rare, the most likely cause of nonanastomotic aneurysms of an AFBG is trauma. An early report was credited to Buche who described a posttraumatic false aneurysm of an AFBG that was treated successfully with an open interposition graft. 5 Shortly thereafter, Piazza et al described a case of a nonanastomotic nontraumatic PSA that occurred 12 months after placement of the graft; and they described the repair of the disrupted segment, which was accomplished with an interposition 8 mm ePTFE graft. 3 Another report on a nonanastomotic PSA of an AFBG was caused by seat belt trauma. 6 Oz et al described a nonanastomotic PSA that occurred 29 months after insertion of an ePTFE that was repaired successfully with open repair. 4 Grochow et al described of a nonanastomotic PSA secondary to chronic abrasion in a paraplegic patient that was treated with a minimally invasive technique. 7 Recently, an additional report on an iatrogenic rupture was described in an 81-year-old patient. The rupture in the mid-shaft of the AFBG/ePTFE occurred 6 years after insertion, there were no signs of infection or internal defect of the graft, and this was treated successfully with an interposition graft. 8
Among the above 4 publications, only one true aneurysm was described 4 and the rest were PSAs. 3,5 –8 The majority of reports described trauma as the primary cause of these PSAs, and that was outlined in our report as well. 5 –7 However, iatrogenic disruption, and even rupture of these grafts, has also been described. 3,4,8 The common material used for the AFBGs described in these reports is the ePTFE.
Most authors recommend routine follow-up on these grafts after placement. The most commonly described repair in the literature is open repair with an interposition graft, to achieve tension-free anastomosis. The only case report utilizing endovascular repair was by Grochow and colleagues. 7
An arterial duplex is a reliable tool for determining an accurate diagnosis, however a more sensitive and specific tool is the CT angiogram, which may also assist in evaluating for localized collection and signs of inflammation or abscess. A complete sepsis work-up is crucial in such cases, including a white blood cell (WBC) scan and blood cultures. The utility of IVUS in these cases cannot be underestimated, and it is also useful in many aspects of intervention, such as proper vessel sizing and estimation of the severity of pathology. IVUS can also be helpful in certain aspects after intervention, such as accurate estimation for cross-sectional area gain, characterization of stent placement, and evaluation of stent expansion and in-stent restenosis.
Conclusion
Pseudoaneurysms of AFBGs can occur with trauma, such as a fall, and can be successfully managed by percutaneous placement of a covered stent.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.