
Abstract
Blunt abdominal trauma with major vascular involvement is found to be rare. Although few series have been reported in the literature, the true incidence of blunt abdominal aortic injury is unknown. Different modalities of blunt trauma may occur among civilians with steering wheel and seat belt injury secondary to motor vehicle accident the most frequent. Mechanical forces produce variable patterns of injury; therefore, the onset of signs and symptoms can be different. Dissection and thrombosis of the abdominal aorta have been frequently described among seat-belted adult patients with major vascular involvement. The associated abdominal viscus and/or vertebral lesions must always be taken into account. Prompt diagnosis allows adequate surgical treatment. We present the case of a 66-year-old woman, restrained front passenger involved in a motor vehicle collision, who had small bowel transection, vertebral fractures, and aortic partial occlusion below inferior mesenteric artery with bilateral iliac artery involvement. Along with the case reported, the purpose of this study is to highlight and compare features and management of the previous cases described in the English literature.
Keywords
Introduction
Blunt abdominal trauma with major vascular involvement is found to be rare. Although few series have been reported in the literature, the true incidence of blunt abdominal aortic injury (BAAI) is unknown. Different modalities of blunt trauma may occur among civilians, with steering wheel and seat belt injury secondary to motor vehicle accident the most frequent. Mechanical forces produce variable patterns of injury; therefore, the onset of signs and symptoms can be different. Dissection and thrombosis of the abdominal aorta have been frequently described among seat-belted adult patients with major vascular involvement.
The associated abdominal viscus and/or vertebral lesions must always be taken into account. Prompt diagnosis allows adequate surgical treatment.
We present the case of a 66-year-old woman, restrained front passenger involved in a motor vehicle collision, who had small bowel transection, vertebral fractures, and aortic partial occlusion below inferior mesenteric artery with bilateral iliac artery involvement.
Along with the case reported, purpose of this study is to highlight and compare features and management of the previous cases described in the English literature.
Comparing to other abdominal viscus, abdominal aorta is rarely involved in the setting of nonpenetrating abdominal trauma.
The BAAI can occur isolated or associated with other lesions. Clinical presentation frequently allows early diagnosis of aortic involvement, but some patterns, such as intimal disruption without thrombosis, might be insidious. Detection of vascular involvement may be hampered by delayed onset of signs and symptoms and by elusive clinical evolution.
Suspicion of vascular lesion is mandatory when facing a blunt abdominal trauma with high impacting or decelerating forces, such as motor vehicle accidents, even more in the presence of intra-abdominal hollow viscus or solid organ lesions.
Thorough investigation about the mechanisms of trauma and careful collection of symptoms relating to acute arterial insufficiency are therefore mandatory. In presence of a seat belt sign, abdominal bruises or weakened peripheral pulses must always be actively checked during physical examination. Moreover, delayed onset of vascular symptoms should be carefully considered.
Methods
A review of the literature was performed in “PubMed” using the keywords “seat belt aorta,” “blunt abdominal aortic trauma,” and “blunt abdominal aortic injury.”
This search yielded 384 articles. The available reports on adult patients involved in car collision and wearing a seat belt with consequent abdominal aortic injury were reviewed. Our search was limited to full text articles in English language from core clinical journals.
We focused on those articles reporting the number of patients, age, sex, clinical presentation, patterns of vascular lesions and associated injury, diagnostic workup, treatment, and outcome. Only 28 articles, describing a total of 31 adult patients, exhaustively reported all the above-mentioned information and therefore were selected. We further report the case of a woman who had an aortic dissection and iliac occlusion secondary to a car accident.
Case Presentation
A 66-year-old Caucasian woman, front passenger wearing a 3-point seat belt, was involved in a head-on collision between 2 cars at approximately 70 km/h (44 mph). On arrival at the emergency department, she was conscious and hemodynamically stable (blood pressure 135/68 mmHg; heart rate 60 bpm; 100% O2 saturation; and Glasgow Coma Scale score 15).
She complained of thoracic, pelvic, and dorso-lumbar pain. Physical examination revealed sternal and abdominal ecchymotic abraded cutaneous bands, abdominal tenderness in the mid-upper quadrant elicited upon palpation, weakened left femoral pulse, and preserved lower extremities motor and sensory function.
Computed tomography (CT) scan showed sternal body fracture, infraction of T4-T5 posterior walls, and a parcellar T12 body fracture. Free air and fluid were detected in the peritoneal cavity, with a small amount of air localized also in the retroperitoneum. Enhanced CT scan showed partial occlusion of the infra-mesenteric aortic lumen due to left-sided eccentric thrombosis upon a calcification (Figure 1), partial thrombosis of the left common iliac artery, and dissection of the right common iliac with both external iliac arteries normally enhanced (Figure 2). The patient was immediately referred to the operating theater.
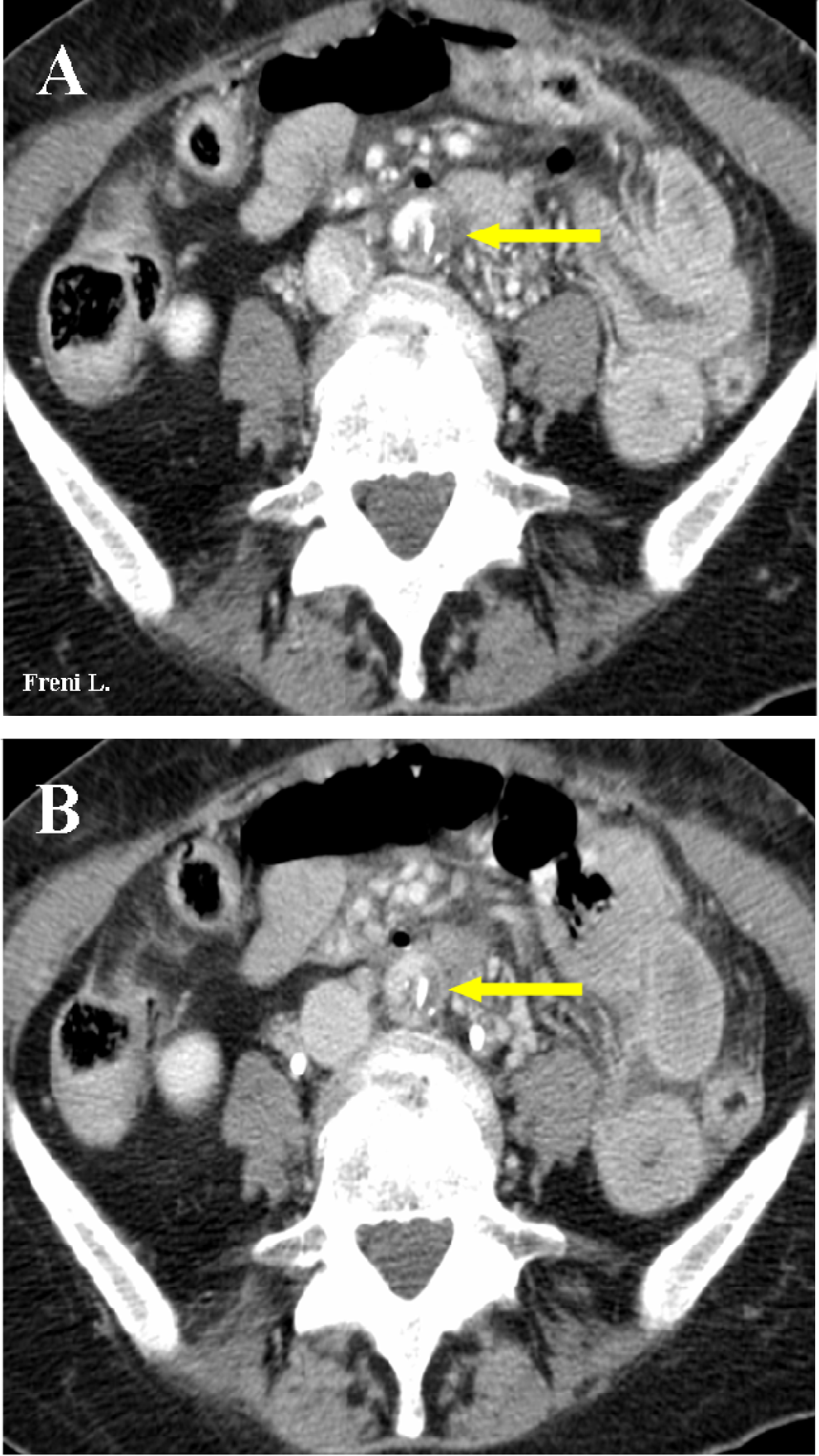
Enhanced computed tomography (CT) showing left-sided eccentric thrombosis (red arrow) upon calcification at the level of aortic bifurcation. A, arterial phase; B, venous phase.
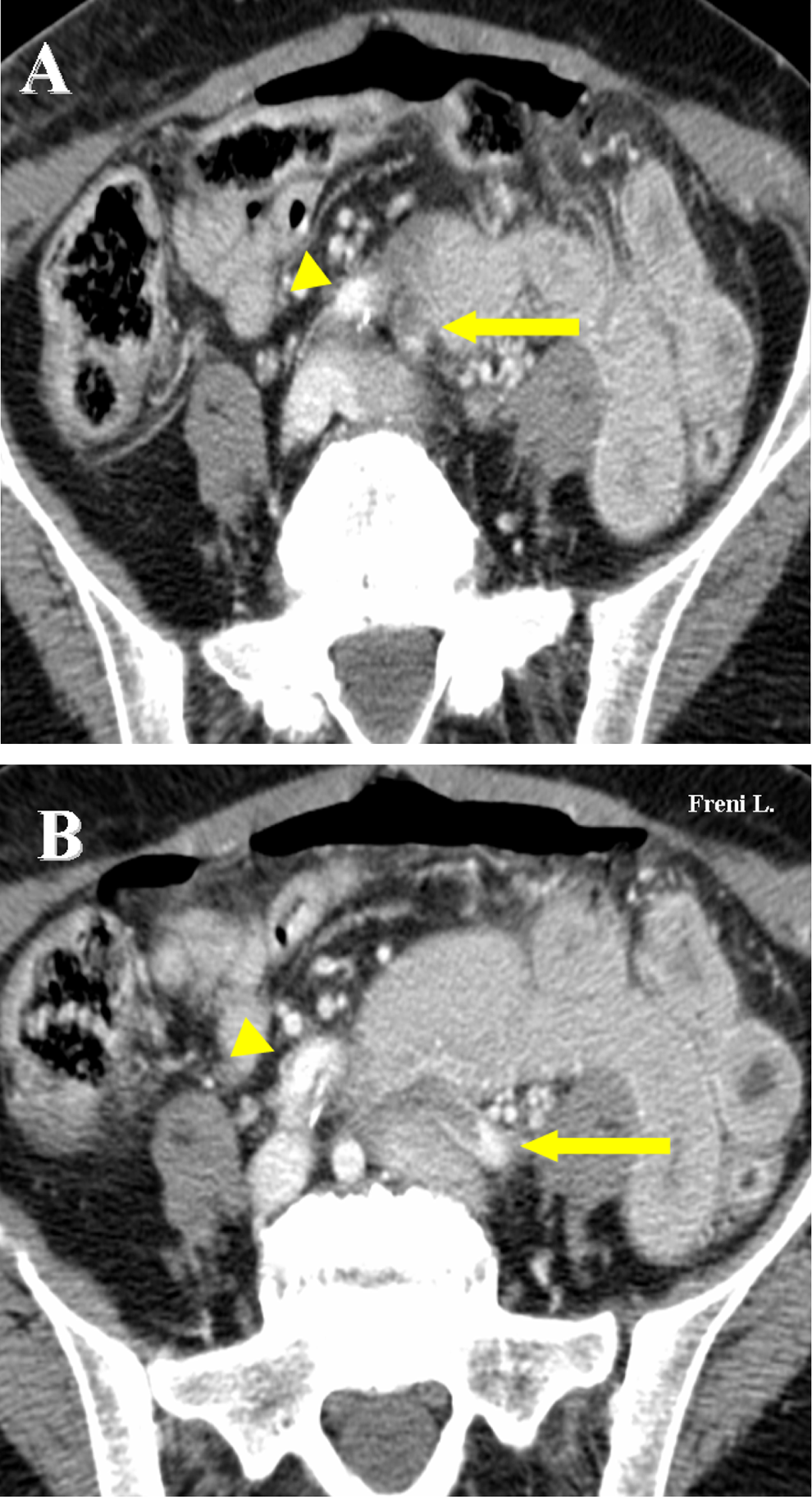
Enhanced computed tomography (CT) scan showing partial thrombosis of the proximal left common iliac artery (arrow) and dissection of the right common iliac artery (arrowhead).
Laparotomy revealed a small amount of blood (300 mL) in the peritoneal cavity and no evidence of solid organ injury. Transection of the second jejunal loop with partial laceration of its mesenterium was detected and repaired with side-to-side functional anastomoses, using a GIA linear stapler (Autosuture - MultiFire GIATM 60 – 2.5 Single Use Reloadable Stapler). Further exploration revealed hematoma of the retroperitoneum at the mesenterial root and behind the aortic bifurcation, with no evidence of active bleeding.
Due to the high risk of peritoneal contamination secondary to bowel transection and the absence of peripheral ischemic symptoms, we decided not to perform any vascular procedure at that time. Thus, a drainage was put into the Douglas cavity.
On the first postoperative day (POD), however, the patient complained of left foot numbness and increasing motor impairment. The left lower limb was hypothermic and mildly pale. A Doppler ultrasound (DUS) revealed left common iliac artery occlusion.
The patient was then rereferred to the operating theater. On exploration of the retroperitoneum, the aortic wall presented an ecchimotic area below the inferior mesenteric artery (Figure 3). A thrill was perceived on the right common iliac artery, which appeared slightly dilated, while the left common iliac artery was pulseless. A longitudinal arteriotomy was performed 3 cm above the aortic bifurcation, revealing a circumferential fracture of the intima and media with a folded flap occluding the left common iliac at its origin and partially the right common iliac artery, which was furthermore dissected (Figure 4). Residual aortic wall at the site of disruption was represented only by adventitia. Arteriotomy was elongated 1 cm toward the right common iliac.
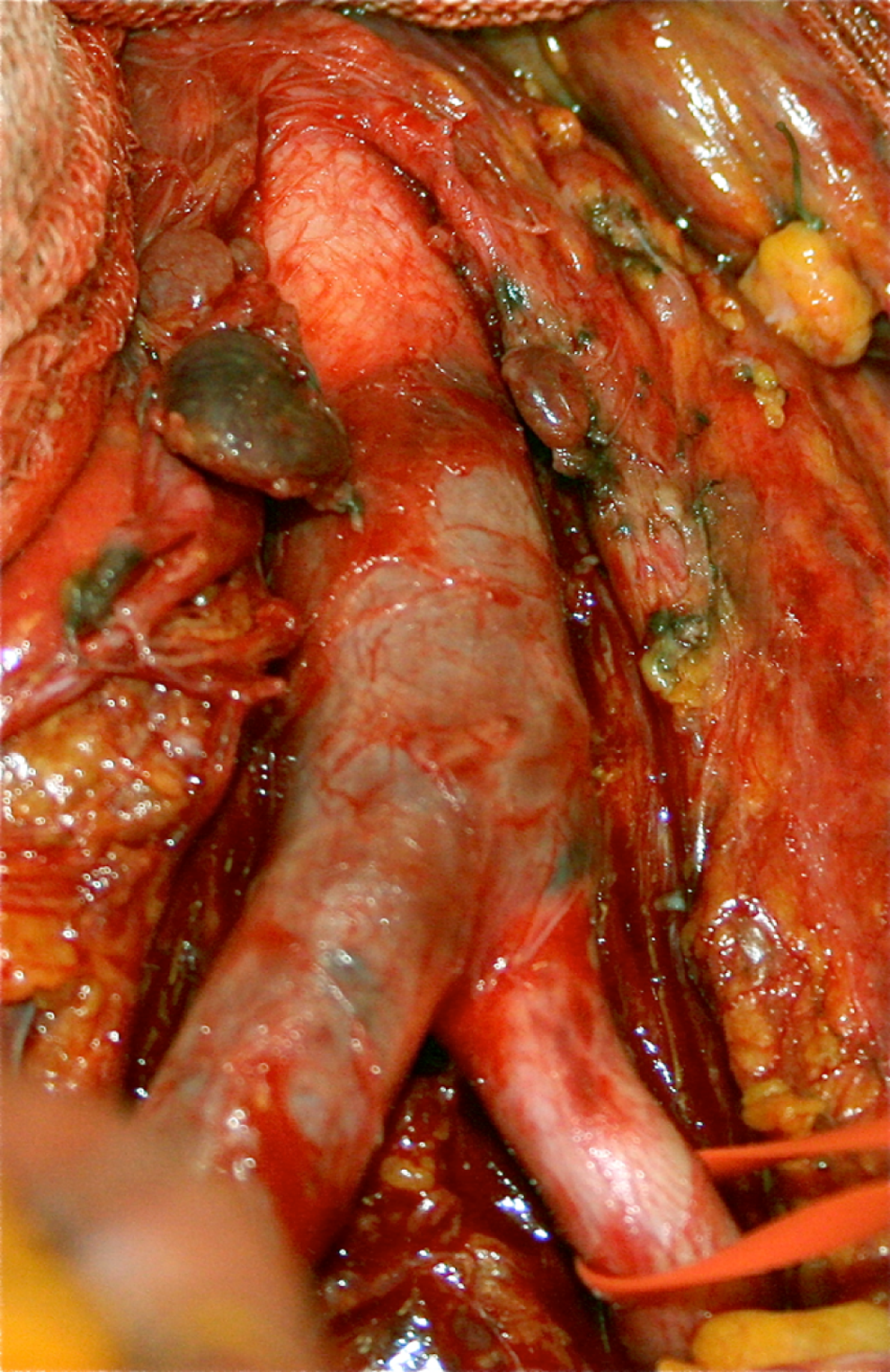
Ecchymotic appearance of the aortic wall below inferior mesenteric artery (IMA) level and of the right common iliac artery (intraoperative finding).
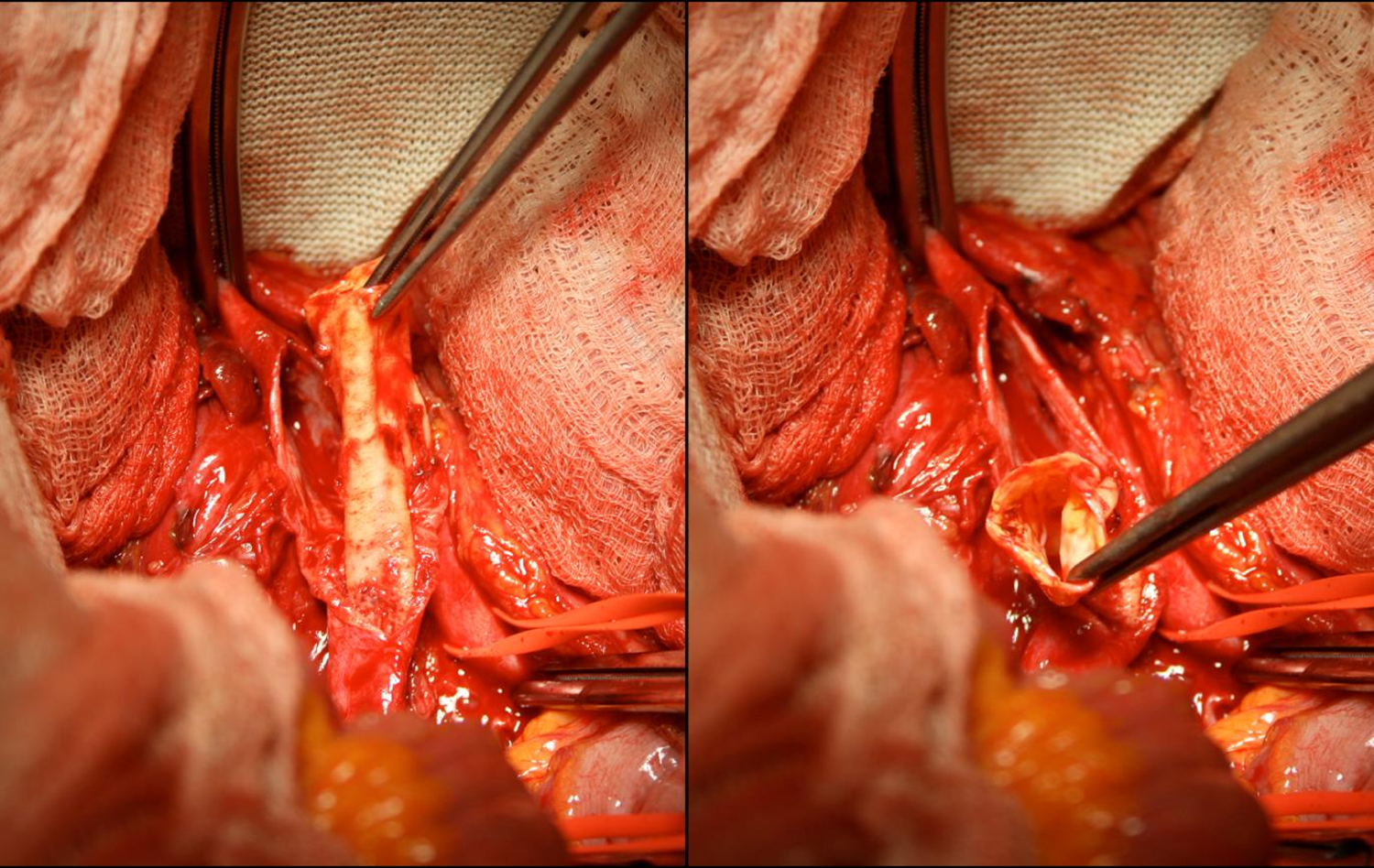
Intimal aortoiliac dissecting flap (intraoperative finding).
The aortic flap was lifted, regularized, and sutured to the adventitia, thus restoring blood flow to the left common iliac artery. The dissected intima-media in the right common iliac artery was repaired as well. Arteriotomy was sutured (Figure 5). Pulses were bilaterally perceptible in common, internal, and external iliac arteries.
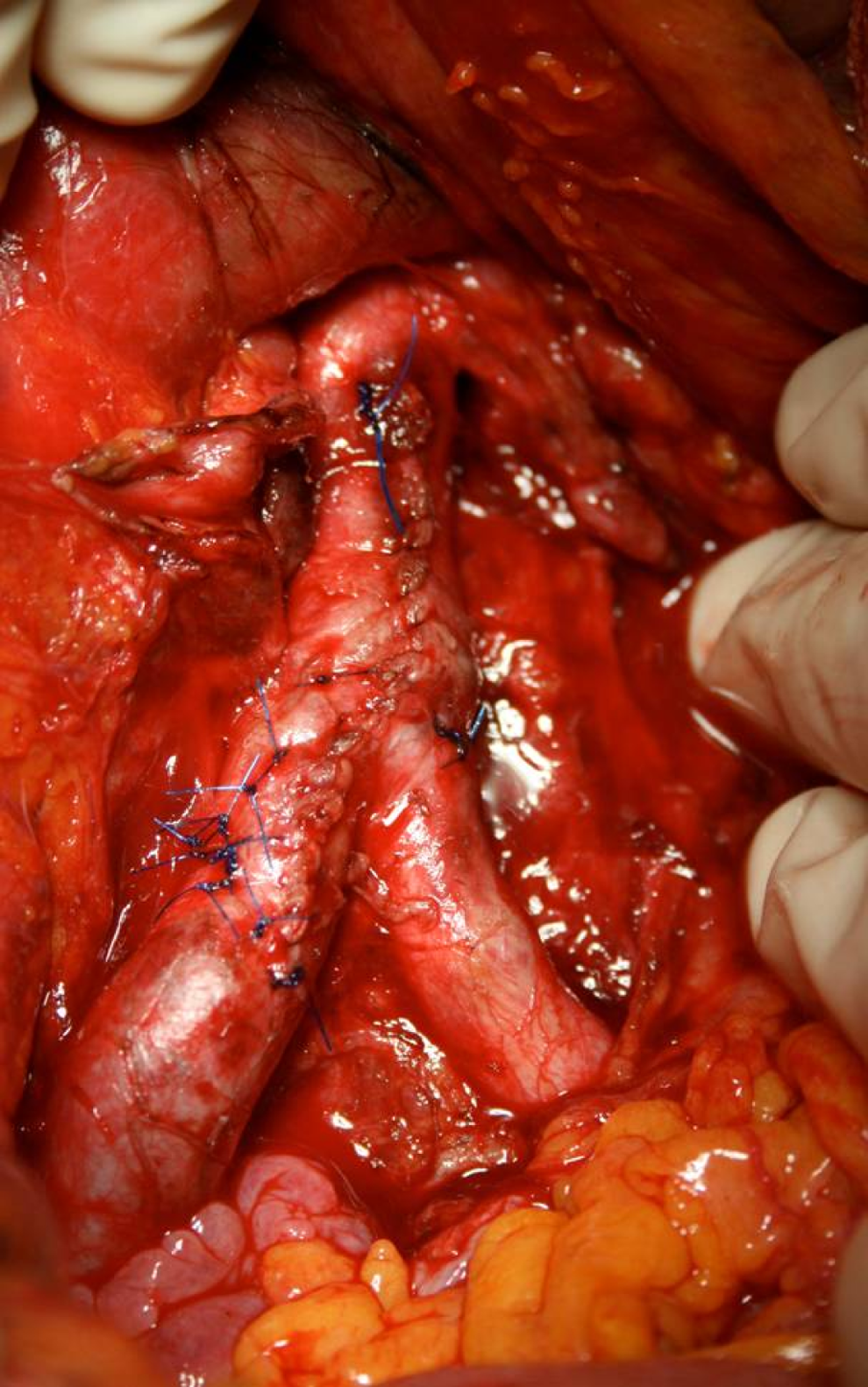
Aortic primary suture following intimal flap regularization and suture to the adventitia.
Intraoperative DUS showed direct flow in right popliteal artery, but occlusion in the left distal popliteal artery. A left popliteal thromboembolectomy with 3 F Fogarty balloon catheter was then performed through infra-articular access.
The patient had an uneventful postoperative course. On 11th POD, a DUS showed no stenosis at the site of aortic sutures, regular diameter of the iliac vessels, and direct peripheral flow to the lower limbs. The patient was then discharged on the 12th POD with corset for spine fractures. The DUS follow-up performed at 6, 12, and 24 months revealed no evidence of aortoiliac stenosis or dilation and proper bilateral lower limb perfusion.
Results and Discussion
Incidence
The first historical description of aortic injury, presumably due to blunt abdominal trauma, was made by Vesalius in 1557. The German anatomist Rindfleisch introduced the observation of a traumatic rupture of the aorta into modern scientific literature in 1893. 1
Approximately, 95% of the injuries to the aorta following blunt trauma are localized at the thoracic district, bearing a high mortality rate. 2,3
Nonpenetrating abdominal aortic trauma, on the other hand, is reported in the literature as a rare condition that is often associated with damage to other intra-abdominal organs. 4
In a study combining autoptic reports on 8710 blunt trauma fatalities, 16 (4.6%) of the 347 nonpenetrating aortic trauma involved the abdominal aorta. 2,5 Series from different trauma centers across the United States report an incidence of abdominal aortic injury between 0.01% and 0.07% secondary to blunt abdominal trauma. 4,6,7 In a recent literature review on BAAI from 1996 to 2012, motor vehicle crashes accounted for more than 60% of the reported causes. 7
Mechanisms of Injury
Since a restraint system was introduced in North America—the single belt in 1964 and the 3-point seat belt in 1973—its effectiveness in reducing fatal injuries, even at slow speed, has been emphasized. 8 Nevertheless, a “seat belt syndrome” was described and seat belt-related injuries have been widely reported. 9 –11
Different studies on dynamic models reproducing exerting forces in the setting of motor vehicle accident describe patterns of compression and deceleration force vectors acting on anatomic structures, either directly or indirectly, as the main mechanism of injury.
Direct forces are triggered by the impact with steering wheel or seat belt. They act exerting a compression on the abdominal contents and on the aorta against the vertebral column, forcing the hollow viscus into the pelvis upon impact and spinal flexion.
Indirect forces originate from the resolution of deceleration vector into a longitudinal and a transverse component, in relation to the vertebral spine.
The former acts upon the aortic blood column, driving it toward the aortic arch, already fulfilled by ventricular contraction. It results in an excessive stretch of the aortic wall at the aortic isthmus, thus favoring intimal disruption. 12-14
The latter results in a traction on the abdominal aorta and the iliac arteries, tractioned on the mesenteric vascular roots and pulled by the abdominal content into the pelvis. Different distribution of the decelerating forces between the abdominal aorta and the common iliac vessels cause a stress concentration at the bifurcation possibly leading to intimal fracture, as in the case herein reported.
Physiopathology and Clinical Presentation
Abdominal pain and acute abdomen is by far the most frequent pattern of presentation, especially when intra-abdominal viscus is injured.
A seat belt sign can be detected along the strap site, varying from mild bruising to soft tissue hematoma or tearing of the abdominal wall 9,11,15 (Table 1).
Review of Reported Cases of Seat Belt Abdominal Aortic Injury in Motor Vehicle Adult Passengers.
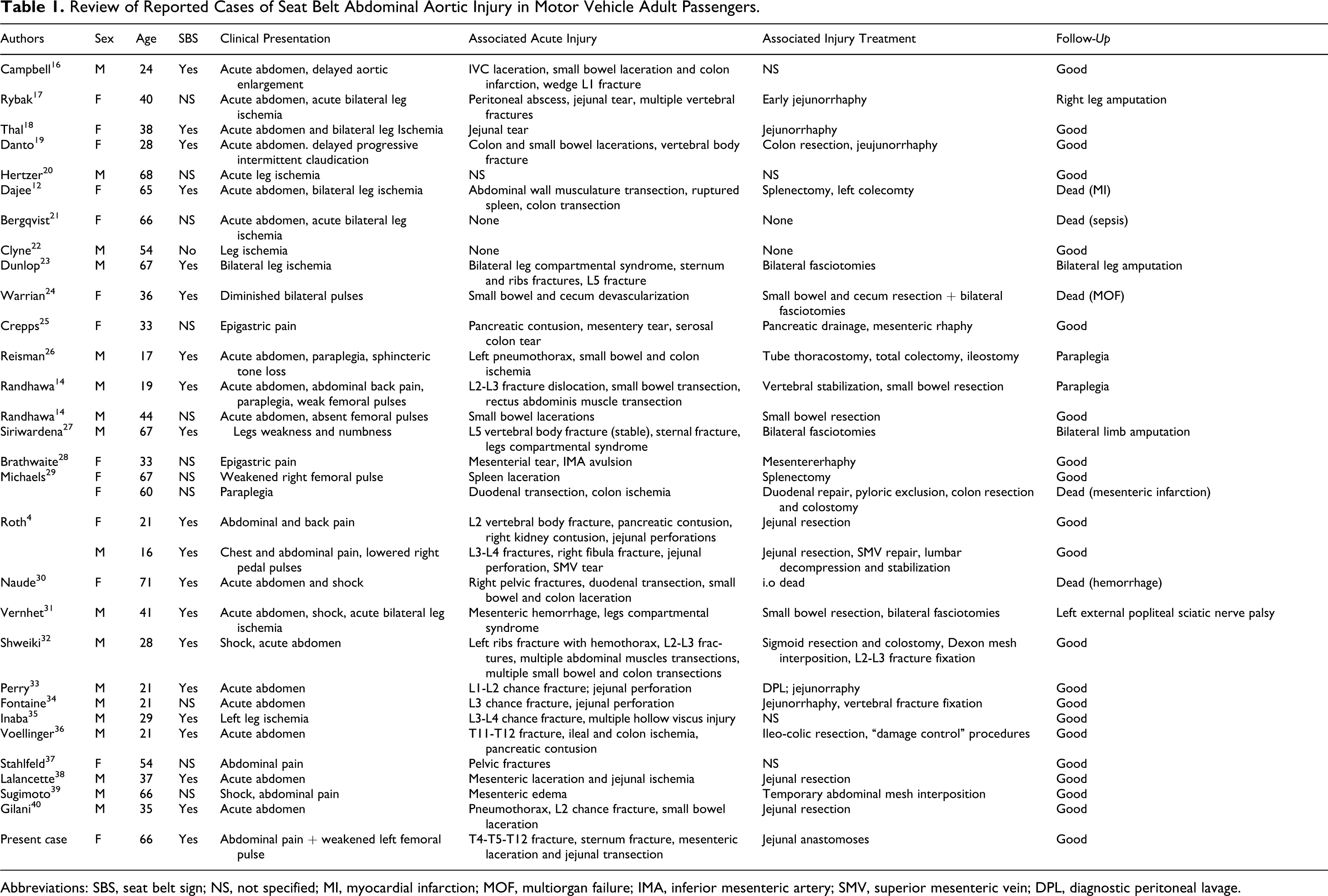
Abbreviations: SBS, seat belt sign; NS, not specified; MI, myocardial infarction; MOF, multiorgan failure; IMA, inferior mesenteric artery; SMV, superior mesenteric vein; DPL, diagnostic peritoneal lavage.
Frequently, abdominal pain and seat belt sign are associated with other findings such as back pain, skeletal fractures, hypovolemic shock, sphincteric tone loss, and lower limb symptoms.
In our review, 60% of the patients reported different patterns of lower limb symptoms at presentation, varying from mild discomfort and numbness to hypothermia, motor impairment, or even paraplegia. Acute vascular peripheral ischemia was by far the most frequent cause of these symptoms.
Overall, clinical presentation can be related to different patterns of aortic injury, which have been described on the base of the extent of vessel wall disruption.
Partial or circumferential aortic intimal tear below the renal arteries, with or without subsequent dissection, is the most common pathologic feature (74%, see Table 2).
Review of Reported Cases of Seat Belt Abdominal Aortic Injury in Motor Vehicle Adult Passengers: Vascular Injuries, Site, and Treatment.
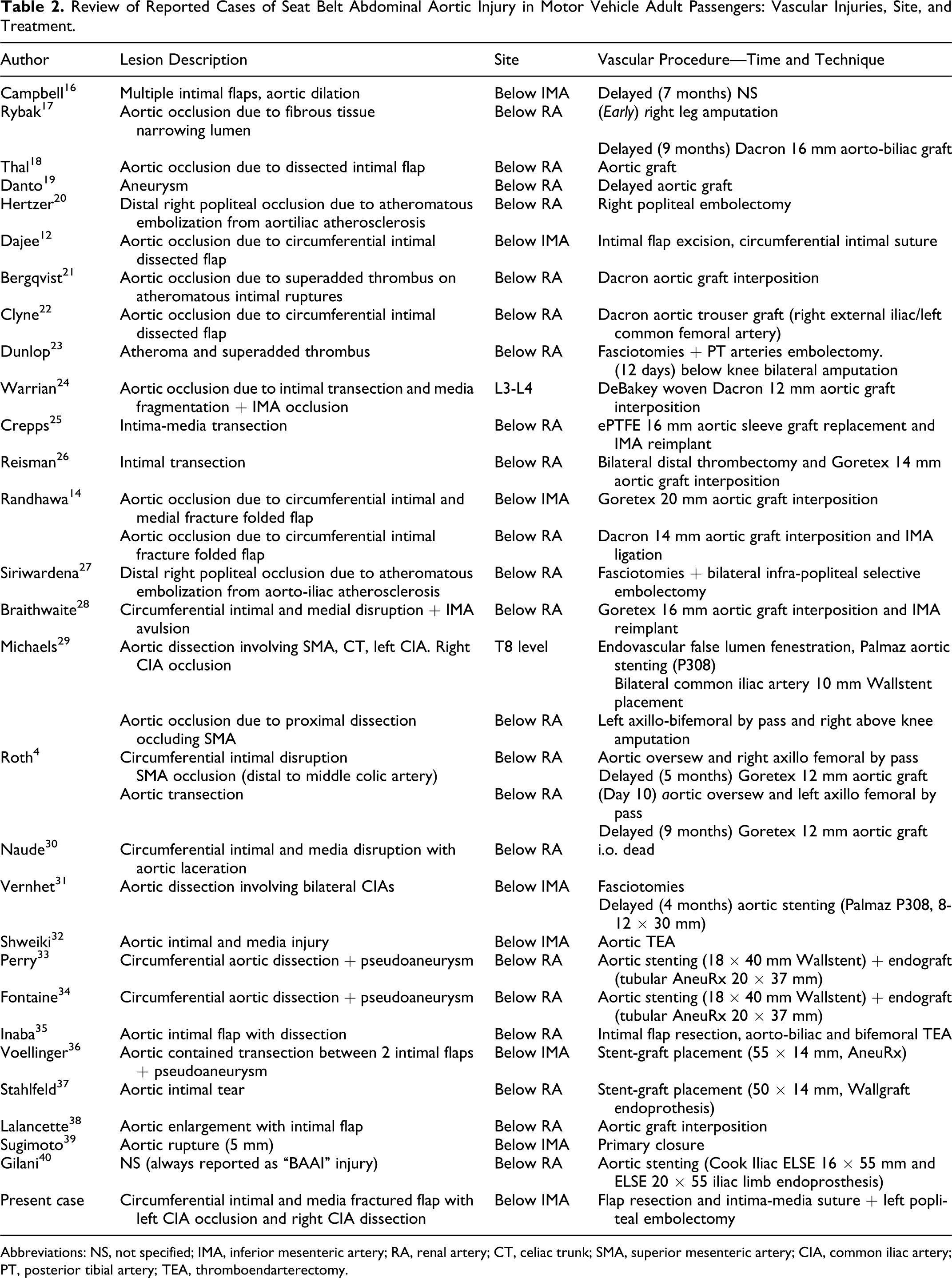
Abbreviations: NS, not specified; IMA, inferior mesenteric artery; RA, renal artery; CT, celiac trunk; SMA, superior mesenteric artery; CIA, common iliac artery; PT, posterior tibial artery; TEA, thromboendarterectomy.
Small intimal flaps, usually asymptomatic, tend to resolve spontaneously if adequate blood pressure control is achieved. Large intimal flaps might induce partial or complete aortic occlusion, with consequent spinal, peripheral, or mesenteric ischemia.
In the absence of direct mechanical spinal cord injury, the level of aortic occlusion accounts for the extension of neurological impairment. Sudden occlusion of the aorta between T5 and L1 is very likely to involve the arteria radiculomedullaris magna (Adamkiewicz artery), causing irreversible lower spinal cord ischemia: painless lower extremity paralisys, dissociated sensory loss, and loss of sphincterial tone, also called “anterior spinal artery syndrome.” 26
On the other side, aortic occlusion below the renal arteries induces acute lower limb ischemia, characterized by dysesthesias and/or painful paresthesias progressing over hours to combined sensory and motor deficits. This kind of symptoms begins distally, spreads centripetally, and tends to recover if the distal aortic reperfusion is promptly restored. 41,42
When aortic occlusion at this level involves mesenteric vessels, a bowel ischemia can occur either by direct occlusion or by thromboembolism.
Aortic intimal tear associated with disruption of the vasa vasorum can be asymptomatic. Progression to subintimal fibrosis and subsequent stenosis may lead to chronic limb ischemia.
Full-thickness disruption of the intima and media, with sparing of the adventitia, results in the development of a false aneurysm over hours to weeks. When no thrombosis or dissection of the aortic lumen is detected atheromatous plaque fracture with distal embolization is the most likely mechanism of peripheral limb ischemia, either acute or chronic. 20,23
Aortic rupture or visceral vessel avulsion with active hemorrhage has been reported too. 28,39
If an aortic damage is detected, then injuries to vertebral column or abdominal viscus are almost invariably present. In our review, associated injuries were present in all the patients except 3 who had isolated lower limb ischemia (94%, see Table 1).
A typical pattern of vertebral injury is a transverse fracture extending through the vertebral body and the pedicles of the spinous process, due to flexion-distraction injury (Chance-like) or pure distraction (Chance) on lumbar spine. 43
Incidence of visceral involvement in the case of BAAI is reported to be as high as 58%, 44 rising to 95% to 100% in the presence of a seat belt aortic lesion. 11,13 In our review, hollow viscus was more frequently injured than parenchimatous organs, with lesions varying from contusion or serosal tear, to transaction and avulsion of the vascular pedicles leading to necrotic ischemia (Table 1).
Extra-aortic vascular injuries, notably inferior vena cava laceration and superior mesenteric vein tear, were reported too. 4,16
Diagnosis
Diagnostic workup for BAAI depends on the patients’ presentation, unstable, stable with vascular symptoms, and stable without vascular symptoms.
Unstable patients mandate expedite abdominal surgery. Proper vascular diagnosis can therefore only be obtained intra- or postoperatively. To note, in this review, which includes patients treated since 1969, vascular injuries were often detected at laparotomy by accurate retroperitoneal examination.
Stable patients with vascular symptoms require further imaging to determine the origin of vascular impairment. Angiography was previously considered the gold standard technique to detect vessels injury and some authors suggested it should always be performed in stable patients with blunt abdominal trauma and suspicion of vascular involvement. 13
Nowadays, spiral CT scan or enhanced CT scan of the abdomen are effective in identifying most of the vascular lesions such as double channel, intraluminal flap, or dilation of the aortic lumen, and may also disclose complications such as dissection, thrombosis, pseudoaneurysm, and aortic rupture. Besides, CT scan allows detection of the associated lesions. Thus, aortography should be performed in the setting of a planned endovascular treatment (EVT) or in case of persistent diagnostic uncertainty.
Absence of vascular symptoms at presentation may hamper recognition of small evolving aortic lesions despite thorough diagnostic workup; therefore, delayed appearance of vascular involvement requires careful and accurate review of the imaging performed at the time of trauma.
Treatment
In our review, surgical repair of aortic injuries required different technical solutions according to the pattern of vascular damage (Table 2). The circumscribed lesions such as aortic wall tearing or short dissections are usually amenable of direct repair throughout endarterectomy and primary suture.
More often, the extent and complexity of aortic damage requires graft interposition, either anatomic or extra-anatomic.
Timing of graft interposition depends on the patients’ clinical conditions, pattern of vascular injury, and the presence of associated intra-abdominal lesions. Moreover, when vascular injuries are detected intraoperatively, treatment is mainly influenced by the presence of peritoneal contamination, which represents a high infective risk of synthetic aortic substitutes. In such cases, aortic injuries should be repaired avoiding the use of prosthetic graft whenever feasible. In the presence of active bleeding, occlusion, aortic transection or extensive dissection, and concomitant massive peritoneal contamination, some authors describe deferred graft placement after emergent proximal and distal aortic ligation and temporary extra-anatomic bypass. 4,13
Indeed, some authors report aortic synthetic graft placement along with repair of injured small bowel, without any incoming graft infection. 14,18
Aortic injury involving atheromatous plaques may cause distal embolization requiring thromboembolectomy. Regardless of the presence of limb ischemia or a good backflow from the iliac-femoral vessels, some authors suggest to systematically perform peripheral bilateral thromboembolectomy. 13
In the last decade, EVT was established as the treatment of choice for traumatic lesions of thoracic aorta. 45,46
Sporadic reports on successful EVT for the acute treatment of seat belt abdominal aortic injuries have been published since the end of the 1990s. 29,33,36,37,40 Emergent EVT represents a practical solution in case of abdominal contamination and may be particularly beneficial to patients requiring either “damage control surgery” or “nonoperative management” of associated lesions. Emergent EVT, however, can be performed in selected high-volume centers with rapid access to emergent intraoperative fluoroscopy and a wide choice of readily available consumables.
The EVT is also a widely accepted option for deferred treatment of posttraumatic dissections or pseudoaneurysm. 3,31
Long-term follow-up data need to be gathered to assess safety and efficacy of EVT and before recommending it as the standard of care.
The rate of mortality in our review was 15%, the causes of death being massive hemorrhage, sepsis, myocardial infarction, mesenteric infarction, and multiorgan failure.
Morbidity after treatment is often related to delayed diagnosis. Unrecognized limb ischemia can lead to ischemia/reperfusion damage and compartment syndrome or even to major amputations (9%). Spinal cord ischemia secondary to aortic thrombosis usually evolves into irreversible paraplegia (6%; Table 1).
Conclusion
Seat belt restrained passengers involved in car accidents had different injuries. Mechanical forces triggered at the time of impact may affect abdominal organs with variable severity at presentation. Abdominal aortic seat belt injury is uncommon but should always be considered regardless of the presence of a seat belt sign and of the speed of impact. Therefore, for investigation of the vascular involvement, peripheral signs of acute ischemia must be assessed.
Indeed vascular assessment should not be neglected in those cases where associated lesions or critical condition require emergent treatment.
Some of the patients with no clinical manifestation of vascular involvement at presentation may eventually develop claudication or silent vascular lesions such as false aneurysm.
In our opinion, careful integration of history of trauma, clinical observation, and diagnostic tools can lead to prompt diagnosis and adequate treatment, which at the state of the art is still represented by open surgical repair. Endovascular treatment can be an appealing solution in selected cases, but further data are needed to validate the technique.
Footnotes
Authors’ Note
Luca Freni was involved in concept and design, literature search, data collection, data analysis, writing the article, critical revision, and overall responsibility. Iacopo Barbetta was involved in writing the article, critical revision, and images editing. Daniela Mazzaccaro was involved in writing the article, critical revision, and drawing. Alberto Maria Settembrini was involved in literature search, data collection, and data analysis. Raffaello Dallatana was involved in concept and design, data analysis, and critical revision. Luca Tassinari was involved in data analysis. Piergiorgio Giuseppe Settembrini was involved in critical revision, final approval, and overall responsibility.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.