
Abstract
Central venous catheterization is a common procedure performed in the critically ill patient. The complication associated with this invasive procedure is well established. However, complication related to the guide wire is rare. We present a case of knotted and entrapped guide wire following central venous catheterization using the Seldinger method and technique to retrieve it nonoperatively.
Introduction
Most complications of central venous catheterization are well recognized but guide wire-specific complication and its management are rarely reported. We present a case of an entrapped guide wire that was retrieved using a minimally invasive technique.
Case Presentation
A 28-year-old lady was found unconscious after a fall down a flight of stairs with her neck flexed laterally against the floor. Computed tomography (CT) and magnetic resonance imaging revealed a fracture of her C5 vertebral body anteroinferiorly with posterior translation of the main bulk of C5 toward the spinal cord, resulting in cord contusion. Halo traction was subsequently applied and a central venous catheter was also needed while she was managed in the intensive care unit.
A right subclavian central venous catheter insertion was attempted by a trainee, using the Seldinger technique. The first attempt was performed under ultrasound guidance but was abandoned. A second attempt was performed using anatomical landmarks. The guide wire was inserted to approximately 25 cm, but at this point it became stuck and could neither be advanced further nor be retrieved. A plain chest x-ray showed the tip of the guide wire had formed several loops at the medial end of the right clavicle, resulting in a tight knot (Figure 1). A CT of the chest with reconstruction was performed in order to determine the relationship of the wire knot to the adjacent vessels. This study (Figure 2) showed that, while the guide wire was largely in the extravascular space, anterior to the brachiocephalic artery and ascending aorta, it was not possible to exclude the possibility that some of the knot could lie within the brachiocephalic vein.
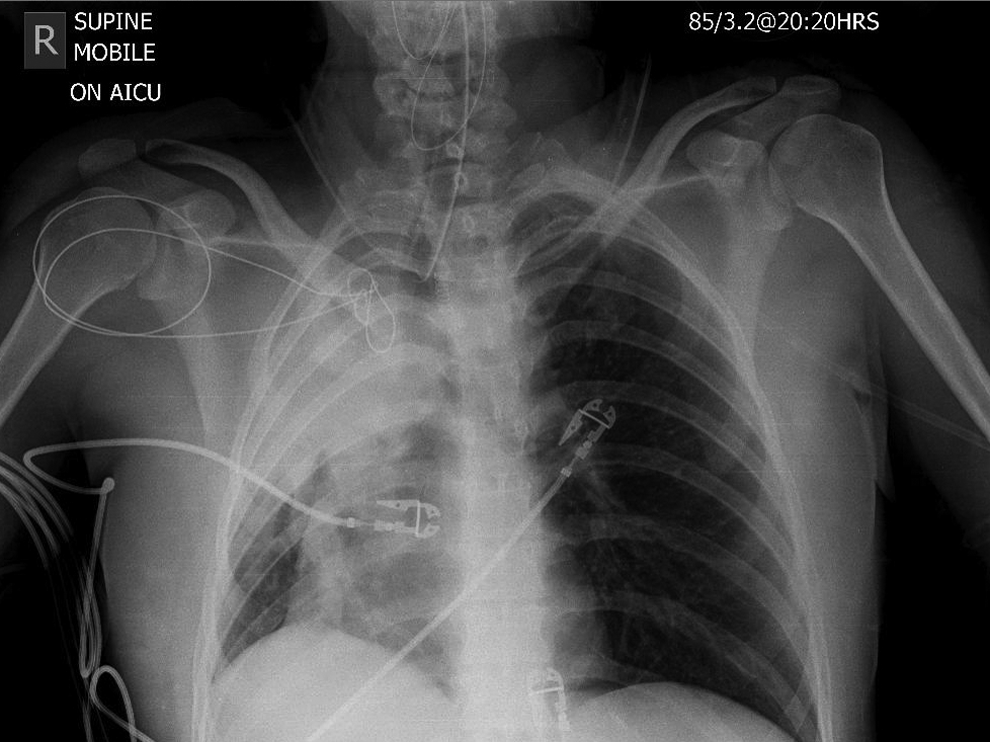
Chest x-ray showing the guide wide had formed a tight knot at the medial end of the right clavicle.
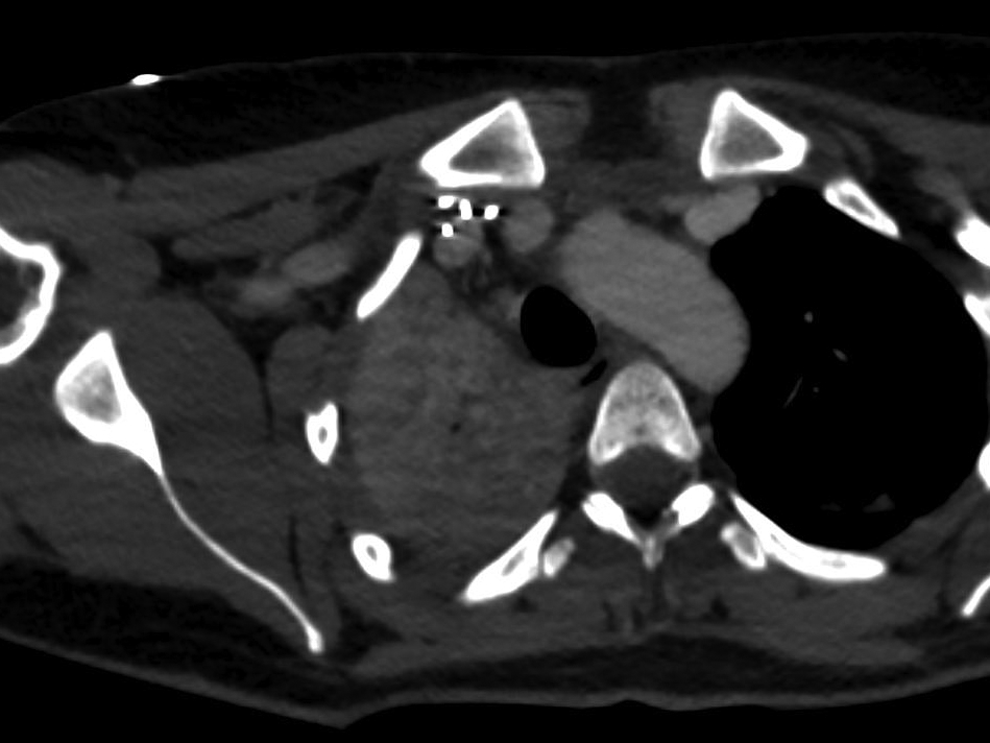
Axial computed tomography (CT) image showing the relationship between the entrapped guide wire and the vessels posterior to the medial end of the right clavicle.
The patient was taken to the operating theater for removal of the entrapped guide wire. As the patient was still ventilated at this stage, the procedure was performed under general anaesthesia with fluoroscopic guidance. A 5-F Van Schie seeking catheter (Cook Medical, Bloomington, Ind) was initially passed over the guide wire in an attempt to loosen the knot but this did not succeed. A 5-F sheath was then passed over the wire to the edge of the knot. The Van Schie catheter was then advanced through the sheath and the tip passed around the first loop of the knot, while maintaining gentle traction on the guide wire and holding the sheath still. This maneuver loosened and expanded the primary loop of the knot sufficiently to allow the Van Schie seeking catheter and the guide wire to be removed together through the sheath (Figures 3 and 4). The procedure lasted for approximately 20 minutes and a postoperative plain chest x-ray excluded a pneumothorax. The patient had a prolonged recovery from her spinal injury and was subsequently transferred to a rehabilitation unit.
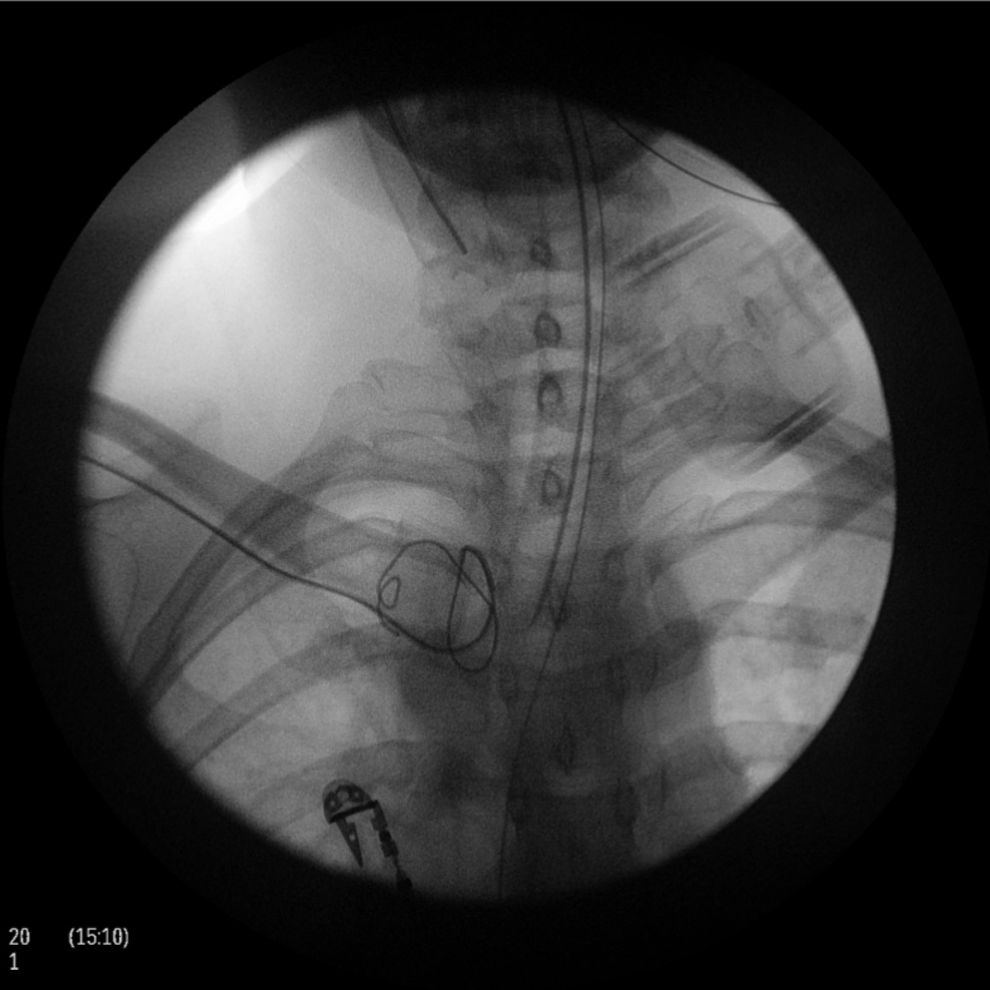
Fluoroscopic image showing the knot had loosened by a 5-F sheath and a Van Schie seeking catheter.

The guide wire was retrieved together with the Van Schie seeking cathether through a 5-F sheath.
Discussion
Central venous catheterization has complication rates of 5% to 19% including misplacement, arterial puncture, pneumothorax, and hematoma. 1,2 Complications related to the guide wire are rare and information about the appropriate management is scarce. 3 Entrapment of a guide wire in both intravascular 4 and extravascular 5 –7 spaces as well as perforation of the vessel wall have been described. 8 –10 Stiff dilators with forceful withdrawal or surgical exploration have been used. 8 –10 Surgical exploration can result in unnecessary morbidity, and using a stiff dilator can cause further kinking as its rigidity may diverge from the flexible path of the wire.
We described this technique to retrieve a knotted and entrapped guide wire without the need of surgical exploration or the use of stiff dilators with excessive force. A good understanding of the structure of the guide wire is required to manipulate and maintain control safely. A typical guide wire consists of 2 parts, an inner single filament wire core surrounded by an outer covering wire that coils its entire length and both parts are welded together at both ends. 11 The weld seam can only withstand a pull strength of approximately 17 N (1.73 kg force) whereas the entire guide wire is able to withstand stress of approximately 290 N (29.57 kg force). 11 Hence, the guide wire should not be pulled with force to prevent detachment of the inner wire from its outer coil.
We recommend 3-dimensional reconstruction of images to determine the position of the guide wire prior to the retrieval procedure and the use of fluoroscopic guidance throughout the procedure. If a guide wire becomes trapped, we recommend referral to an endovascular specialist. Pulling the guide wire alone is likely to tighten the knot, making it more difficult to retrieve and potentially resulting in vascular injury.
To avoid the problem of guide wire entrapment, ultrasound guidance should be considered for all guide wire insertions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.