
Abstract
This report describes the hybrid endovascular treatment of an aortic root dilatation and a thoracoabdominal aneurysm in a high-risk patient with Marfan syndrome. A 50-year-old male, in hemodialysis for polycystic kidney and polycystic liver, was referred to our department for aortic root dilatation of 5 cm and a 6.3-cm thoracoabdominal aneurysm . He already underwent surgical repair of abdominal aortic aneurysm 10 years ago, complicated by pseudoaneurysm of the proximal anastomosis that had been treated in another center, with an endoprosthesis. The patient underwent aortic root replacement, aortic valve sparing operation, and rerouting of the superior mesenteric artery and celiac trunk to the ascending aorta. The thoracoabdominal aneurysm was excluded with an endoprosthesis few days after the surgical step. The 12-month computed tomography scan confirmed the complete exclusion of the thoracoabdominal aneurysm.
Introduction
Aortic root and thoracoabdominal aneurysm are common manifestations of Marfan syndrome and the most important determinant of prognosis. Many patients die from complications such as aortic rupture and aortic dissection, without surgical intervention. 1 Management of these lesions represents a major challenge for surgeons, as the gold standard treatment for patients with Marfan syndrome is total replacement of the aneurysmatic aorta through open approach. This technique however is burdened by high mortality and complication rates, even in high volume centers. 2
Hybrid treatment (surgical and endovascular) has been recently proposed as an alternative for the treatment of the aneurysmatic disease, especially in prohibitive high-risk patients.
Case Report
A 50-year-old male patient with Marfan syndrome, in hemodialysis for polycystic kidney since 7 years and affected by polycystic liver and chronic heart ischemia with 35% ejection fraction, was referred to our department for aortic root dilatation of 5 cm, with moderate aortic insufficiency and a 6.3 × 5.6 cm2 thoracoabdominal aneurysm. Ten years before, he had undergone surgical repair of an abdominal aortic aneurysm. Eight years after the operation, a pseudoaneurysm of the proximal anastomosis developed. A tubular endograft was then placed in another hospital to correct the lesion (Figure 1). Since the patient was already in hemodialysis, the pseudoaneurysm was excluded covering both renal arteries with the graft (Zenith; Cook, Bloomington, Indiana). Probably, due to the high strength of that endoprosthesis, associated with an intrinsic disorder of the aorta, the endograft had expanded into a new aneurysm, which involved the origins of both the superior mesenteric artery (SMA) and the celiac trunk (CTR). After discussion with the patient, family consent was given, and the patient underwent aortic root replacement, aortic valve sparing operation, and rerouting of the SMA and the CTR to the ascending aorta. After sternotomy, the skin incision was prolonged to the mid part of the abdomen, and the SMA and CTR were isolated. Cardiopulmonary bypass was instituted from ascending aorta and right atrium; after cardioplegic cardiac arrest, the aortic root was replaced sparing the aortic valve, with a 30-mm Dacron graft, and the coronary ostia were reimplanted (David type I operation). After the aorta was declamped and the heart restarted, a 10-mm Dacron prosthesis was anastomosed to the anterolateral part of the neoascending aorta and tunnelized through the diaphragm into the abdomen. The CTR and SMA were separated from the aorta and connected together with a 8-mm Dacron prosthesis; finally, the prosthesis coming from the ascending aorta was anastomosed to the prosthesis connected to the SMA and CTR. Immediate postoperative examination was fine, and the patient was discharged from intensive care unit after 24 hours. Three days later, the patient underwent endovascular exclusion of the thoracoabdominal aneurysm in the interventional cardiology suite, under general anesthesia. Cerebrospinal fluid (CSF) drainage was used to prevent paraplegia. Two Gore C-TAG stent graft 26-26-10 and 28-28-15 (W.L. Gore & Assoc, Flagstaff, Arizona) were placed through surgical exposure of the right common femoral artery, from midthoracic aorta to midabdominal aorta. The Gore C-TAG 26-26-10 endoprosthesis was first implanted using the mid thoracic aorta free from thrombus or dilatation as proximal landing zone; then, the Gore C-TAG 28-28-15 was placed, with 5 cm of overlapping over the first endoprosthesis and using the surgical Dacron abdominal prosthesis as a safe and unexpandable distal landing zone. Immediate angiographic control was good, and a compliant stent graft balloon was inflated to mold the devices only in the overlapping zone and in the distal landing zone. We decided not to dilate the proximal landing zone due to the fragility of the Marfan aorta. The CSF drainage was removed 3 days later according to the hospital protocol. The recovery was uneventful, and predischarge computed tomography (CT) scan showed the complete exclusion of the aneurysm without any sign of endoleak. Echocardiographic control showed a perfect continent aortic valve.
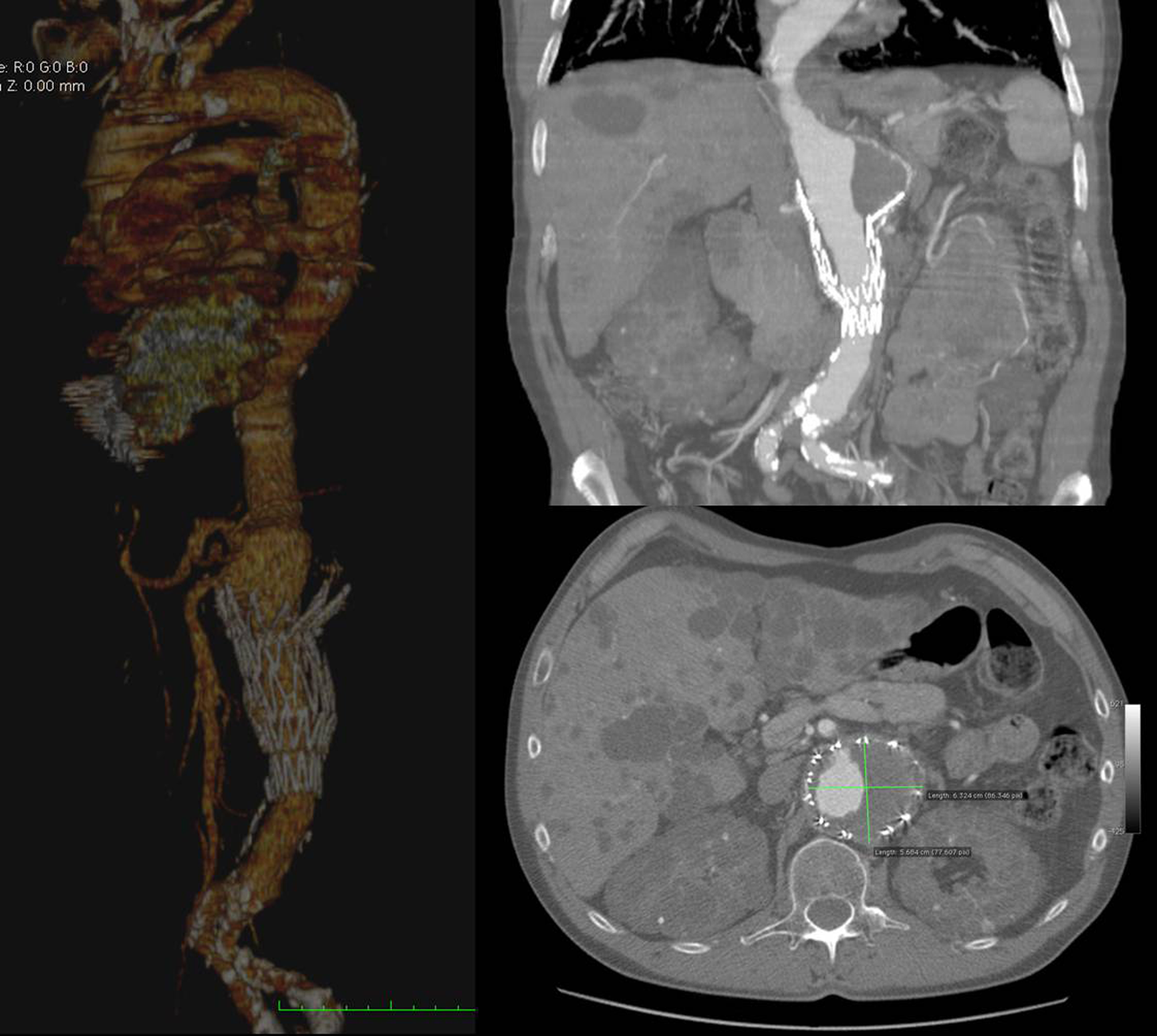
Preoperative computed tomography (CT) scan showing aortic root dilatation and thoracoabdominal aneurysm.
The patient was then transferred to the renal unit three days later in good physical conditions.
The 12-month CT scan confirmed the complete exclusion of the thoracoabdominal aneurysm (Figure 2), and the patient is still in good conditions.
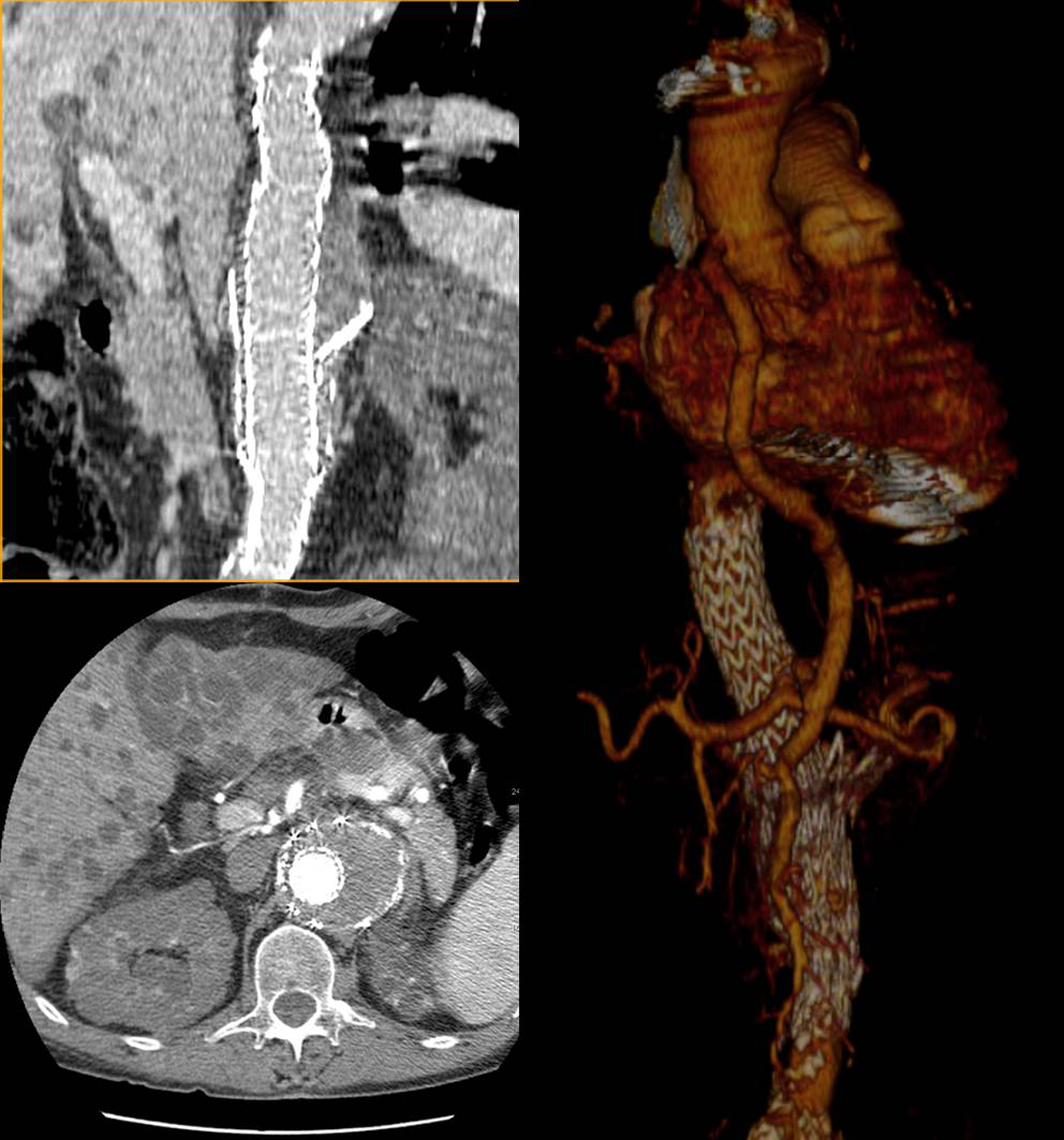
Twelve-month computed tomography (CT) scan control showing exclusion of the aneurysm and the rerouting of the visceral arteries to the ascending aorta.
Discussion
The patients with Marfan syndrome are challenging, particularly when more than one district of the aorta is involved. In our case, the 5 cm aortic root dilatation was of primary importance for high risk of rupture or dissection. Our goal was to replace the aortic root and ascending aorta preserving the aortic valve, thus avoiding complications derived from the mechanical prosthesis and long-term anticoagulation. 3
Regarding the correction of the thoracoabdominal aneurysm, use of endoprosthesis in patients with Marfan syndrome is a matter of debate 4 ; particularly, free flow and high radial force endoprosthesis are discouraged due to the induced dilatation of the native aorta. 5 In our report, the thoracoabdominal aneurysm had been enhanced probably by the stress of the previous implanted endoprosthesis on a genetically diseased aorta. We implanted Gore C-TAG grafts in order to use an endoprosthesis with a reported radial force lower than any other available device. We decided to oversize the endoprosthesis to only 5% and not to use a free flow endograft in the proximal landing zone, to avoid overstress on a diseased aorta which was predisposed to dilate.
The ideal treatment for the thoracoabdominal aneurysm in our patient would have been the surgical removal of the endograft and the replacement of the diseased aorta with direct reimplantation of the visceral arteries. 5 However, due to the comorbidities, we believed that the patient was too fragile to afford 2 major cardiovascular surgery in a short period. Moreover, both due to the prior abdominal surgery and the presence of the endograft, a total open approach would have been challenging. Therefore, we decided upon a 2-step hybrid endovascular treatment to reduce the invasiveness of the thoraco-abdominal aneurysm treatment. Since surgical therapy was the only solution for aortic root dilatation, we used the new ascending aorta for the rerouting of the visceral arteries allowing a good proximal landing zone in the thoracic aorta and a preexisting perfect unexpandable distal landing zone in the abdominal aorta. The endovascular step was delayed 3 days after surgery step to allow complete recovery of the patient from the cardiac surgery.
In the literature, experiences with hybrid treatment of thoracoabdominal aneurysms involving visceral debranching in high-risk patients are limited to small series. 6 Similar experiences in patients with Marfan syndrome are in the form of rare case reports. 7 To our knowledge, the present case is the first report of a hybrid endovascular correction of a thoracoabdominal aneurysm following endovascular aortic repair in a patient with Marfan syndrome.
Concerns may raise about the risk of spinal cord ischemia 8 in a patient who had already undergone abdominal aortic repla-cement. During or immediately after cardiopulmonary bypass, the ability to maintain supranormal mean arterial pressures to augment spinal cord perfusion may be limited by bleeding. Moreover, many authorities may contraindicate the use of CSF drainage because of the presence of coagulopathy and the subsequent risk of central nervous system complications. The use of CSF as a tool to prevent spinal chord ischemia is still a matter of debate, 9 but in our experience, the presence of an abdominal surgical prosthesis and the extension of the endoprosthesis in the thoracic aorta are mandatory for CSF. In our report, hybrid endovascular treatment of aortic root and thoracoabdominal aneurysm has proven to be an appealing and feasible alternative to total open repair in this high-risk patient with Marfan syndrome. However, our experience is limited, and further studies and reports are needed to assess this technique.
Conclusion
Hybrid endovascular treatment of an aortic root dilatation and a thorachoabdominal aneurysm in a high-risk patient with Marfan syndrome could be a valid alternative to 2 major cardiovascular surgery, especially in prohibitive high-risk patients. Early results are encouraging, but only long-term follow-up will elucidate the role of the endoprosthesis in patients with Marfan syndrome.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.