
Abstract
Thoracic aortic endografting has been successfully implemented to treat aneurysmal disease of the distal aortic arch and descending thoracic aorta. Although there are reports of ascending aortic endovascular interventions, the total endovascular repair of a ruptured ascending aorta secondary to a Type A dissection has not been described. We report the case of a 77-year-old patient who presented with a ruptured ascending aortic aneurysm secondary to degeneration of a Stanford type A aortic dissection. His surgical history was significant for orthotropic heart transplant 19 years prior. The dissection, aneurysm, and rupture occurred in the native aorta distal to the ascending aortic suture line. At presentation, he was hemodynamically unstable with a right hemothorax. We placed 3 Medtronic Talent Thoracic Stent Graft devices (Medtronic Inc, Minneapolis, MN) across the suture line in the ascending aorta, excluding the rupture. The patient survived and has been followed to 25 months.
Introduction
Thoracic aortic dissection results from a disruption of the aortic intima leading to a dissection plane and a false lumen within the aortic media. The annual incidence of aortic dissection is 3 to 4 per 1 00 000 patients, and it represents the most common aortic emergency. 1 Dissections may be classified by their anatomy (eg, De Bakey, Stanford) or by the time to presentation (eg, acute, subacute). 1 Dissections of the ascending aorta carry an especially high morbidity and mortality as the dissection can propagate to the coronary arteries and aortic valve, compromising cardiac function. Given these risks, open surgical correction of the ascending aortic dissection has been the rule. Recently, hybrid open and endovascular therapies have been described for treating pathology of the ascending aorta. To date, no report has described the emergent total endovascular repair of an acute ascending aortic rupture.
Case Report
We present the case of a 77-year-old male with a history of ischemic cardiomyopathy and orthotropic heart transplant 19 years previously. He had a known Stanford type A aortic dissection of the native aorta. The dissection flap originated at the suture line between the transplanted and the native ascending aorta and terminated proximal to the innominate artery. As the suture line appeared to limit proximal extension of the dissection toward the heart, it was managed medically. Open repair of the dissection was considered but not undertaken due to a history of sternotomy on 4 previous occasions, diffuse and circumferential aortic calcification, and multiple medical comorbidities. He presented to the emergency department of our hospital after an episode of syncope and right-sided chest pain. Computed tomography (CT) angiogram of the chest revealed aneurysmal degeneration and rupture of the dissection resulting in a substantial right hemothorax (Figure 1).
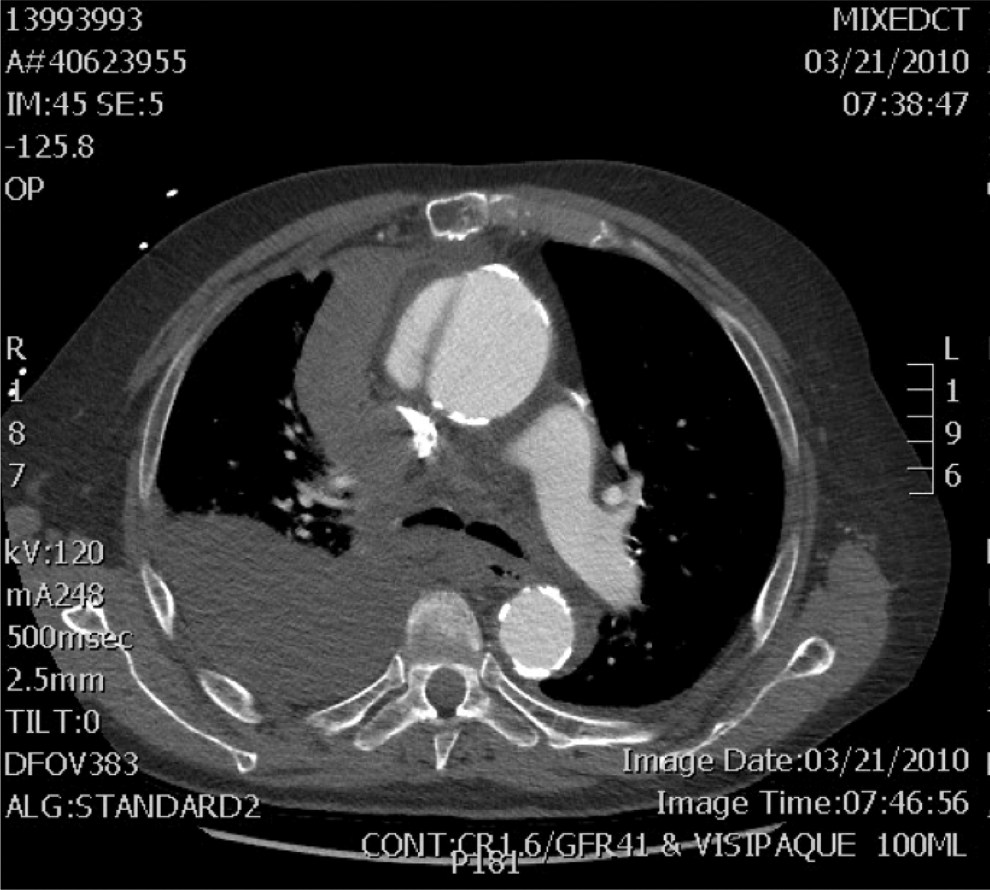
Preoperative computed tomography (CT) scan revealing dissection flap in the ascending aorta, contrast extravasation, and right hemothorax.
The morbidity and mortality of an open rupture repair were felt to be prohibitive; therefore, the patient was evaluated for endovascular repair. After careful review of the CT scan using 3-dimensional reconstruction, we noted that due to the transplant, his ascending aorta, proximal to the innominate artery, was greater than 20 cm in length. We were able to identify both a proximal and a distal landing zone, and based on this, we decided to attempt an endovascular repair of the ruptured ascending arch aneurysm. He was taken to the operating room emergently.
Open bilateral femoral arterial access was obtained. Wire access was obtained to the level of the left ventricle, and angiography confirmed a long ascending aorta, 20 to 25 cm in length, with proximal and distal diameters of 33 mm and 42 mm, respectively (Figure 2).
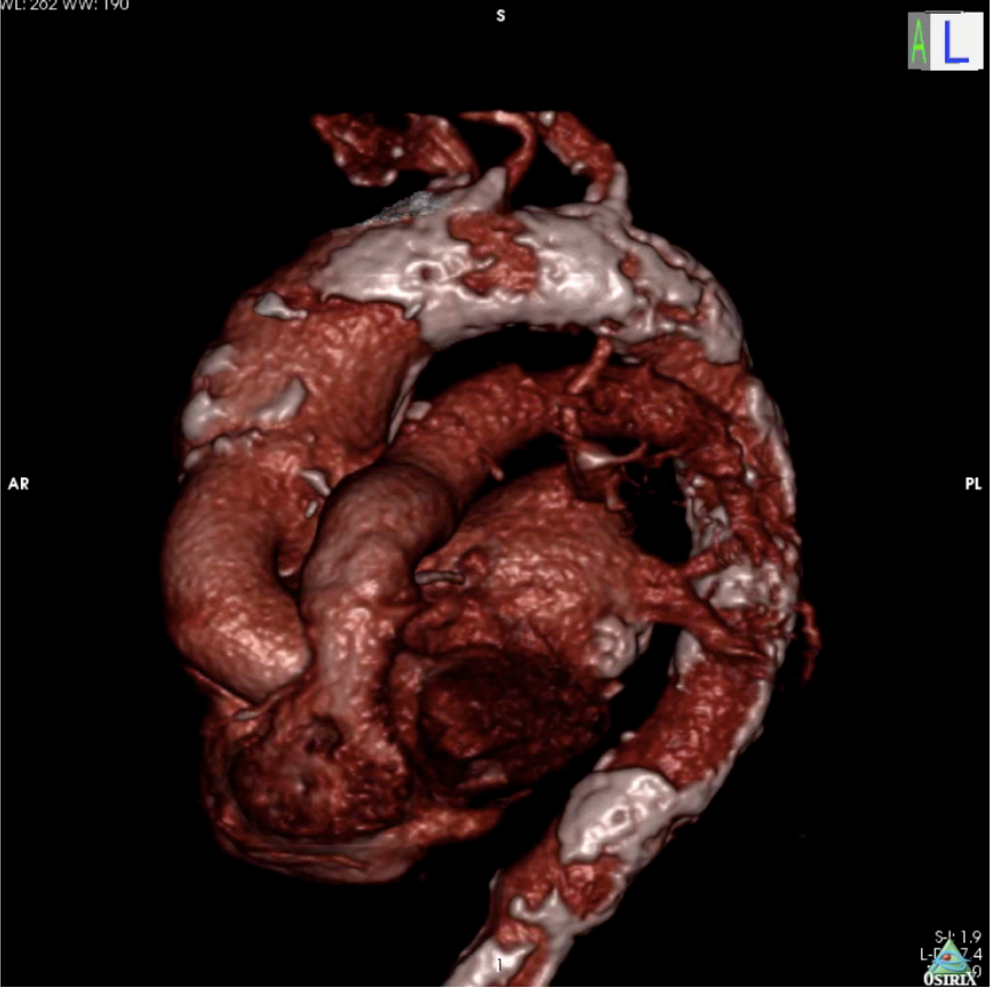
Three-dimensional (3-D) reconstruction of preoperative computed tomography (CT)-angiogram revealing long ascending aorta, aortic diameter difference between transplanted and native ascending aorta, and diffuse aortic calcifications.
The Medtronic Talent Thoracic Stent Graft (Medtronic Inc, Minneapolis, Minnesota) was selected for the repair. The Talent proximal main body device dimensions were 40×40 × 115 mm. The system required the use of 3 devices to cover the dissection and to accommodate the change in diameter between the proximal and the distal landing zones. One limitation of the proximal main body device was the presence of the uncovered proximal stent. Although these are not a concern when treating the descending aorta, in this case, it would have limited the seal zone, as we did not have enough length from the aortic valve to the aneurysm to accommodate the uncovered stent and still gain seal with the covered portion of the stent graft.
In order to facilitate maximum proximal seal, the main body device was deployed on the back table and reversed so that that the proximal end did not have any uncovered stent area. The uncovered area was now in position to be deployed as the distal end. The reversed stent graft was carefully repacked into the delivery device (Figure 3). After gaining wire access into the left ventricle, we positioned the tapered tip of the device in the ventricle under direct visualization and performed arteriography to define coronary artery anatomy. Adenosine was used to attempt arrest of the heart, while the graft was deployed distal to the coronary arteries; however, cardiac arrest was not achieved as the transplanted heart had been denervated. We used the left coronary artery as the proximal extent of the proximal landing zone. Given the change in diameter from the transplanted to the native portions of the ascending aorta, the second device used was a tapered graft that measured 40 × 44 mm and which bridged between the proximal and distal devices. For the native aorta at the distal seal zone, a 46 × 46 × 115 mm device was selected. The device was positioned so that the distal most aspect landed just proximal to the takeoff of the innominate artery.
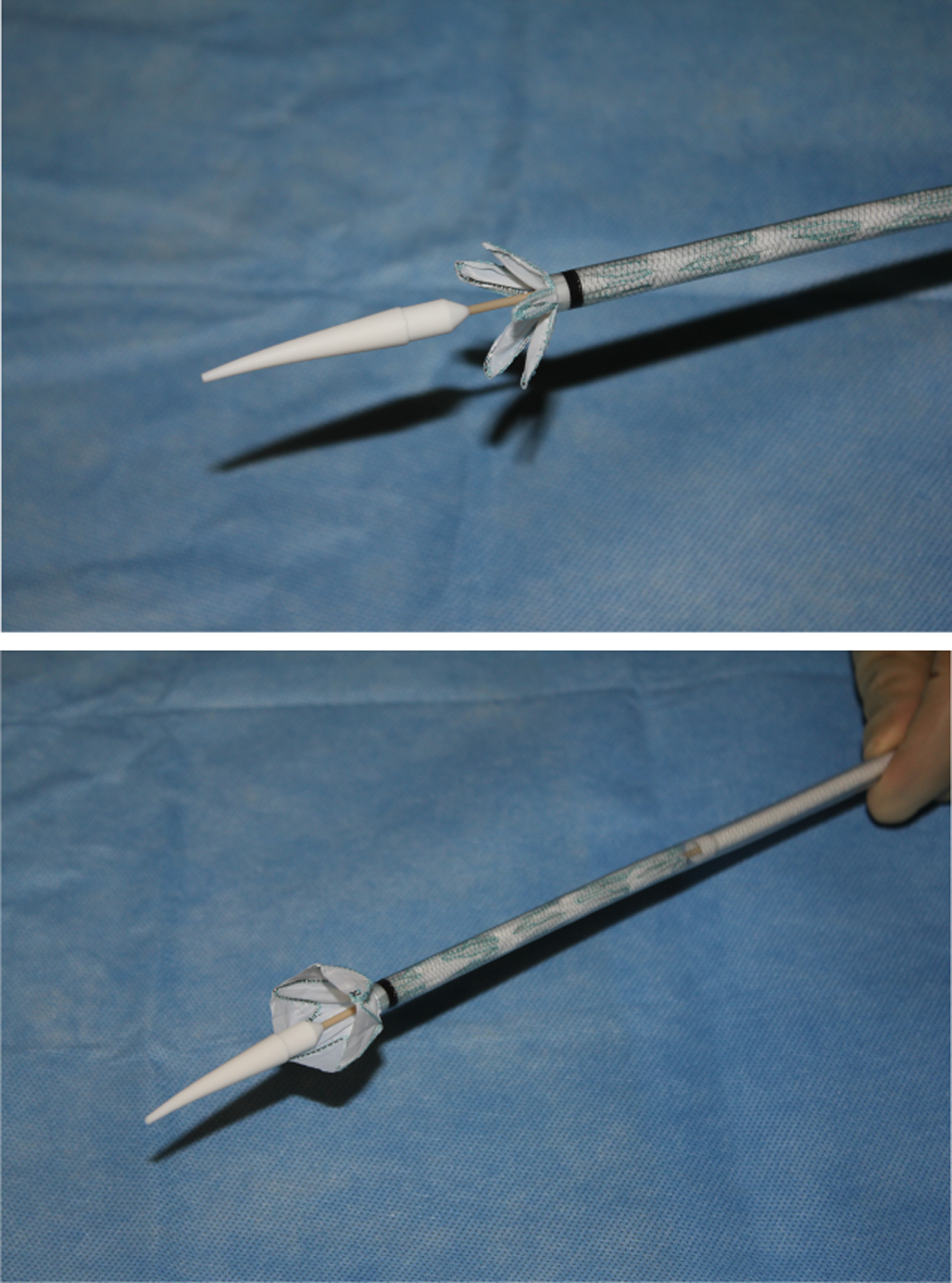
Demonstration of backtable graft deployment, reversal, and repacking into delivery system.
Completion angiography confirmed exclusion of the aortic rupture, patent right and left coronary arteries, and unobstructed flow to the innominate artery and distal aorta (Figure 4). At the completion of the case, a single 36F chest tube was placed on the right side, and 1000 mL of blood was evacuated from the right chest. The patient was admitted to the intensive care unit and had an uneventful recovery.
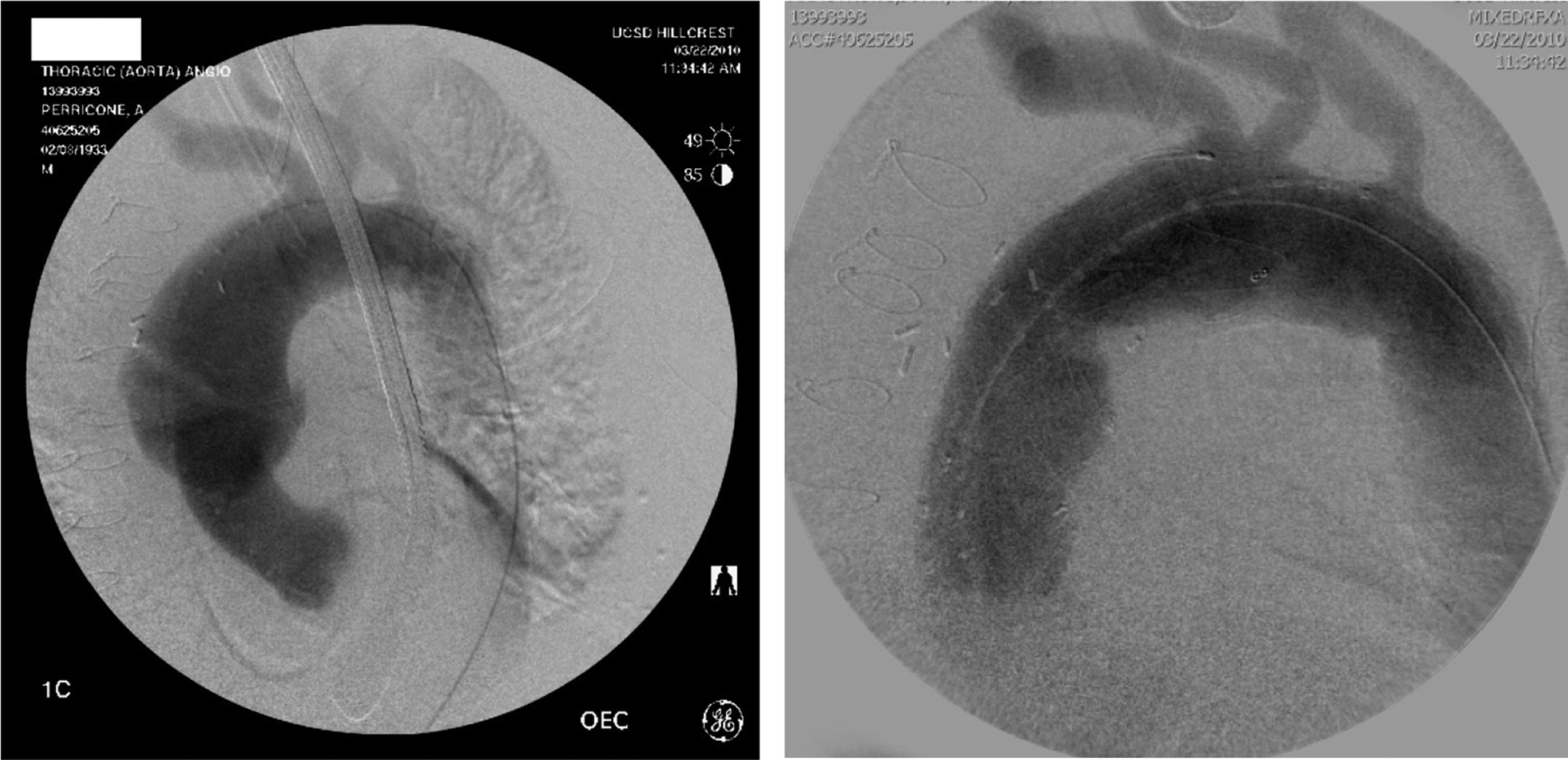
Pre- and Post-stenting angiogram demonstrating exclusion of the rupture.
Imaging at 19 months after endovascular repair verified exclusion of the aneurysm and stable aneurysmal size. The hemothorax had resolved. However, incidental imaging at 25 months revealed further aneurysmal degeneration of the distal seal zone, Type Ib endoleak, and enlargement of the aneurysm. At that time, he was no longer an endovascular candidate from an anatomic and medical standpoint. He did not have a distal seal zone proximal to the innominate artery origin and would have required an aortic arch debranching in order to obtain a distal seal. He was not a candidate for an open operation or a hybrid procedure due to his preexisting medical comorbidities and newly diagnosed metastatic prostate cancer.
Discussion
Thoracic aortic endografting is widely used for disease of the descending thoracic aorta. The anatomy of the ascending aorta poses additional problems when considering endovascular treatment options. The proximal location of the heart and aortic valve make injury to these structures, including free ventricular perforation, a significant risk. 2 In addition, the presence of the coronary arteries limits the proximal extent of the landing zone.
The endovascular treatment of the ascending thoracic aorta has been reported, including pseudoaneurysm, 3 dissection, 4–10 and intramural hematoma 11,12 (Table 1). Vaughan-Huxley et al 3 report a case of an acute repair of a mycotic pseudoaneurysm which, although not treated emergently, bears similarity to our case in that it was attempted as an option of last resort in a patient likely to perish without the intervention. Metcalfe et al 5 report the repair of an acute ascending aortic dissection with a device designed specifically for this purpose, the Cook Zenith Ascending Dissection device. Their case illustrates a point of frustration for American vascular interventionalists confronting ascending aortic pathology, as devices available in Europe and elsewhere abroad are not available in the United States. With the exception of the report by Ihnken et al 8 from Stanford University in 2004, no reports originate from the United States.
Reports of Endovascular Repair of Ascending Aortic Pathology.
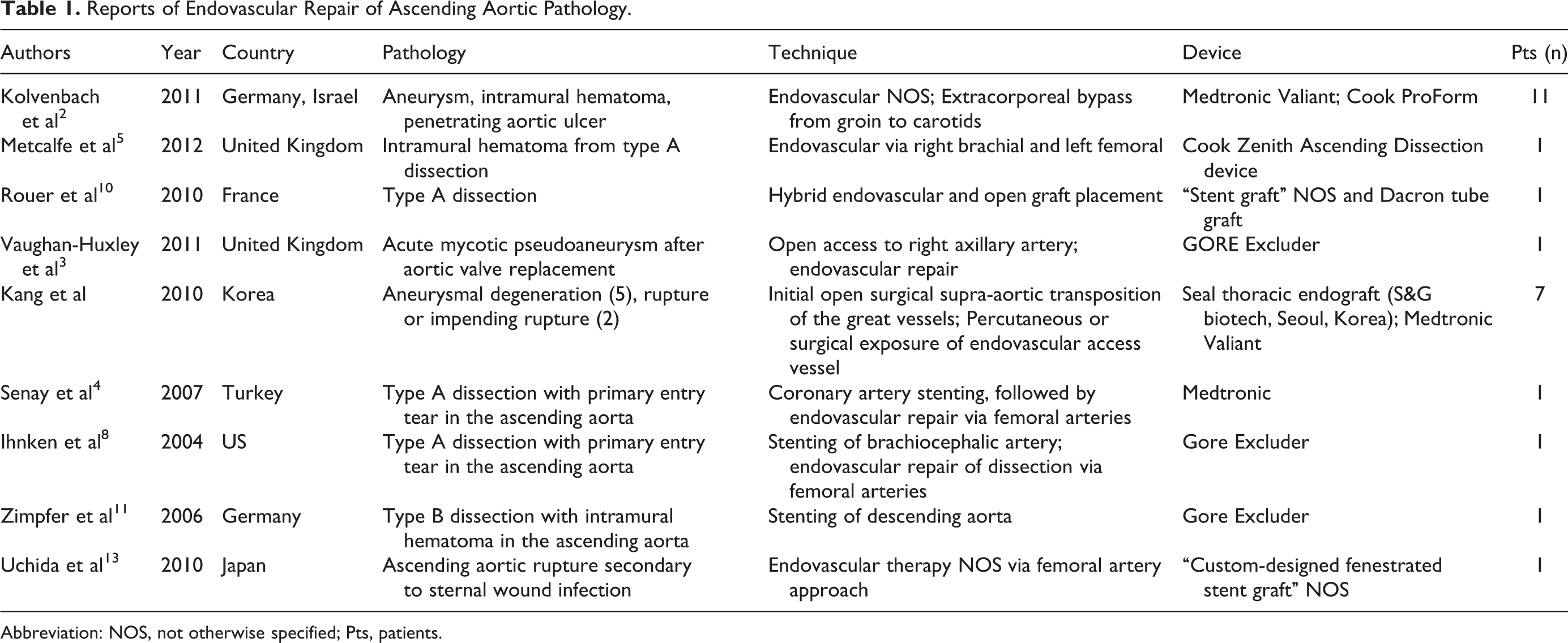
Abbreviation: NOS, not otherwise specified; Pts, patients.
We believe that ours represent the first reported case of a ruptured ascending dissection treated by endovascular techniques alone. Although we were able to seal proximal to the takeoff of the innominate artery, the use of a fenestrated graft to extend the distal seal zone beyond the takeoff of the carotids has been described in cases of ascending aortic rupture. 13,14 Factors that enabled the treatment of this patient via endovascular approach were the presence of an aortic suture line that limited the extent of the dissection and subsequent aneurysm from the aortic valve as well as the long length of the ascending arch. This patient was not a candidate for open repair due to the presence of a circumferentially calcified aorta, his medical comorbidities, and the risks associated with what would have been his fifth sternotomy. As stent graft technology continues to evolve and branched and fenestrated devices become available, the endovascular repair of the ascending arch will become broadly applicable.
This case illustrates the successful use of a stent graft for the repair of a ruptured ascending aorta that was secondary to a chronic dissection. Although the repair was not durable, it was successful in treating the acute rupture that otherwise would have been fatal.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.