
Abstract
Objective:
We conducted a retrospective study to compare short- and mid-term patencies of Viabahn with surgical above-knee prosthetic bypass (pAKB).
Methods:
The records of 52 patients with either pAKB (n = 25) or Viabahn (n = 27) were reviewed. The majority had Rutherford clinical grade 3. Patients were followed after 3, 6, and 12 months and yearly thereafter.
Results:
For Viabahn, the short-term (1-16 months) primary patency rate was 60% with a secondary patency rate of 90%, and mid-term (1-68 months) patencies of 47% and 83.3%, respectively. In pAKB, the short-term results revealed a primary patency rate of 78% with a secondary patency of 91% and mid-term results of 65% and 90%, respectively. No statistical difference was found concerning short-term patencies. Mid-term primary patency was lower for Viabahn (P < .05) and secondary patency proved no significant difference.
Conclusion:
Viabahn revealed similar short-term primary and secondary patencies but lower mid-term primary patency. It provides a good alternative therapy to pAKB.
Keywords
Introduction
The most common location of the peripheral atherosclerotic disease in the lower limb is the superficial femoral artery (SFA). 1 So far, there are different treatment modalities such as surgical bypass, percutaneous transluminal angioplasty (PTA), stent implantation, and the endovascular implantation of endoprosthesis. Among these options, the surgical above-knee bypass (AKB) is still considered the “gold standard” in the treatment of SFA occlusive disease. 2 However, technical advances in endovascular therapy offer a considerable alternative to the surgical treatment. After encouraging results of the endovascular implantation of a self-expanding expanded polytetrafluoroethylene (ePTFE)/nitinol stent graft called Hemobahn endoprosthesis (WL. Gore, Flagstaff, Ariz) from an international trial, 3 the graft was modified and introduced as Viabahn endoprosthesis. 4 Although several subsequent studies since that time confirmed the initial respectable patency results, 5 –9 fewer reports exist comparing the outcome of the Viabahn with that of the surgical AKB for the treatment of SFA occlusive disease. 4,10,11 The purpose of our study was to evaluate and compare the outcome of Viabahn endoprosthesis with the surgical AKB for the treatment of SFA occlusive disease in a real-world setting by retrospective analysis of patients treated by both modalities.
Materials and Methods
Patients
From 2005 to 2011, 52 (60 limbs) consecutive patients who underwent either surgical AKB or Viabahn endovascular prosthesis implantation were identified. The medical records of these patients were retrospectively reviewed, including demographic details, risk factors, clinical characteristics, diagnostic images, type of revascularization procedures, and their results. In all, patients conservative therapy was maxed out. All patients had chronic ischemia and were categorized by Rutherford categories based on symptoms and clinical presentation at the time of the revascularization. Patient demographics and the associated risk factors are shown in Table 1.
Patient Demographics and Risk Factors.
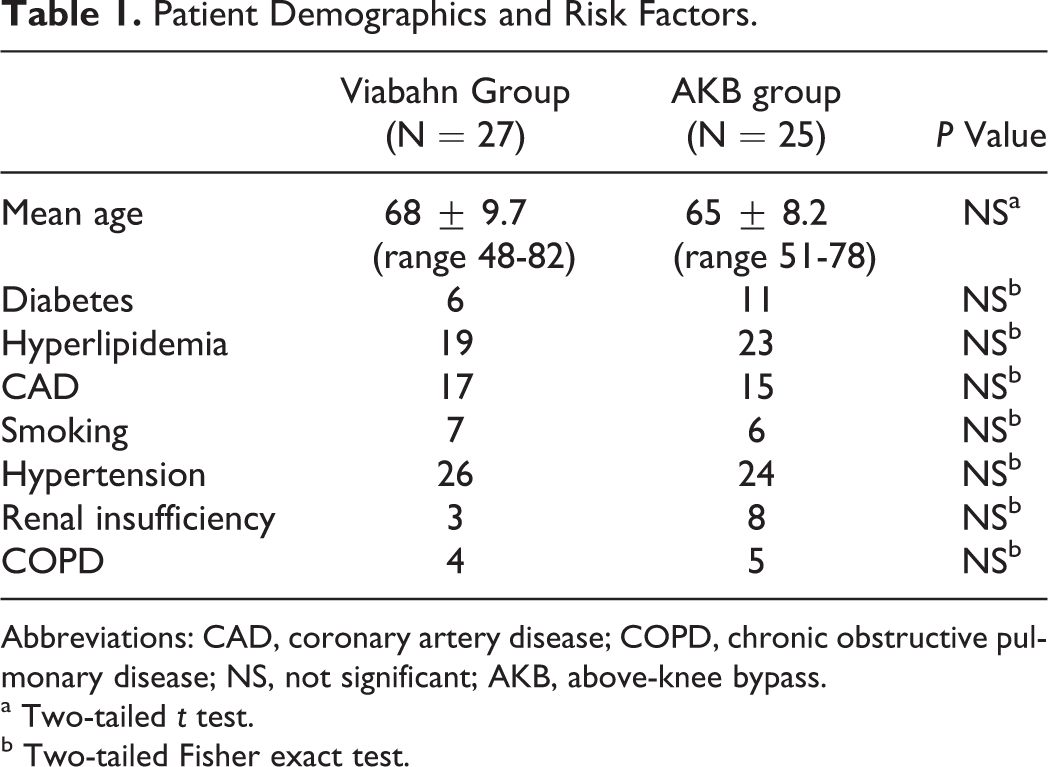
Abbreviations: CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; NS, not significant; AKB, above-knee bypass.
a Two-tailed t test.
b Two-tailed Fisher exact test.
Technique
Both techniques were performed under general anaesthesia. The Viabahn stent graft implantation was performed using standard small surgical exposure of proximal SFA and subsequent traditional angioplasty stenting techniques. The surgical AKB was accomplished in the usual surgical fashion. As conduit, ePTFE grafts were chosen. All patients received heparin (5000 units) during the procedure. After treatment, combined antiplatelet therapy with aspirin (100 mg/d) and clopidogrel (75 mg/d) was administered for at least 6 months and one of them thereafter in the Viabahn group. The surgical AKB received aspirin 100 mg/d alone. In case of associated comorbidities requiring oral anticoagulation therapy, warfarin was added to the antiplatelet therapy.
Follow-Up
Follow-up was performed at 1, 3, 6, and 12 months and yearly thereafter and included clinical assessment and resting ankle-brachial index (ABI) measurement. In the case of abnormal findings, duplex imaging or computed tomography angiography was performed to confirm the graft patency. Graft patency was analyzed by primary and secondary patencies. Primary patency was defined as uninterrupted freedom of restenosis or occlusion within the treated vessel, and secondary patency was defined as restored graft patency after occlusion or stenosis. 12
Statistical Analysis
In statistical analysis, 2-tailed Fisher exact test was used to determine the differences in patient risk factors and 2-tailed t test was used to calculate differences in patient demographics. Generalized Fisher exact test was used to assess differences in grades of limb ischemia. The Kaplan-Meier method with the log-rank test was applied to compare the graft patency. A P value less than .05 was considered statistically significant.
Results
The retrospective analysis included medical records of 52 patients treated between 2005 and 2011 with either implantation of Viabahn endovascular prosthesis (27 patients, 31 limbs) or femoral to AKB (25 patients, 29 limbs). No significant difference in demographics and risk factors was found between the 2 treatment groups. Rutherford classification of limb ischemia was used to assess the clinical status of patient’s limb prior to treatment (Table 2).Technical success was achieved in all the treated patients. In all, 50 Viabahn endoprosthesis were implanted in 31 limbs, with a mean of 2 ± 0.83 grafts per limb. The mean treated lesion length was 19 ± 11.06 cm. The mean Viabahn diameter was 6 mm (range 5-8). In the surgical AKB group, ePTFE grafts were used in all patients. Patients showed a mean total lesion length of 24.39 ± 1.97 cm. Here, the mean graft diameter was 7 mm (range 6-8). The difference in graft diameter proved to be statistically significant (P < .01). Procedural-related or early postoperative complications were not noted in both the groups. Analysis of hospital stay was performed for both groups and revealed a significantly shorter duration of hospital stay (P < .01) in the Viabahn group with a mean of 4.8 ± 4.05 days, whereas the mean hospital stay in the surgical group was found to be 9.8 ± 5.53 days.
Rutherford's Clinical Grades of Chronic Limb Ischemia in Study Patients.
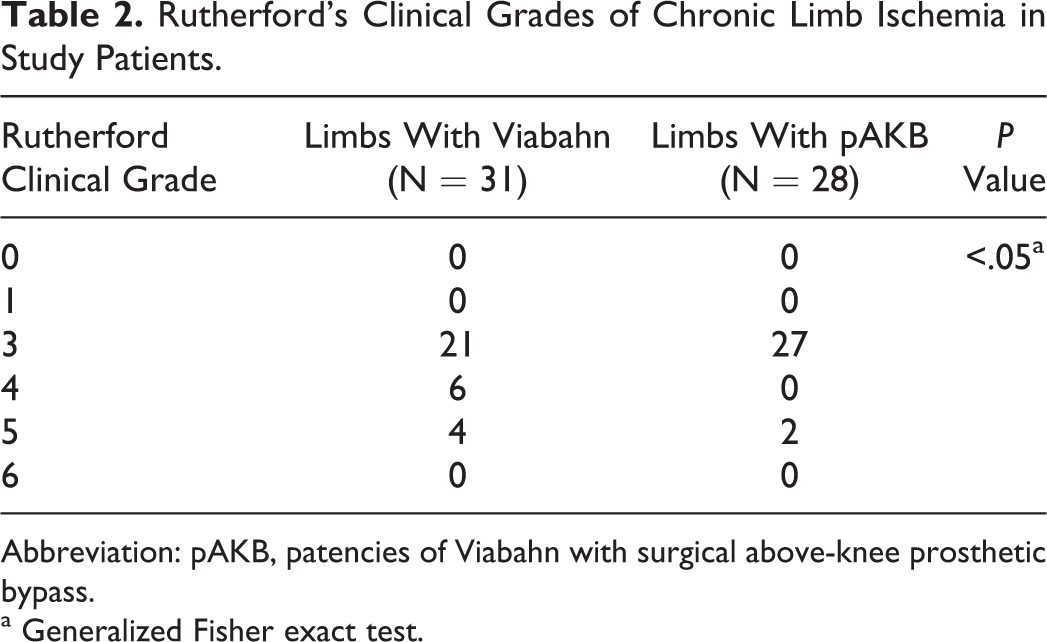
Abbreviation: pAKB, patencies of Viabahn with surgical above-knee prosthetic bypass.
a Generalized Fisher exact test.
Short-Term Results
Mean short-term follow-up was 7.5 months (1-16). In the Viabahn group, a total of 12 (27%) grafts failed due to thrombosis. There was no Viabahn graft thrombosis during postprocedural hospital stay. Two stent graft failures occurred during the first month after implantation. The remaining failed after a mean period of 7 ± 4.2 months. Among the 7 patients with failed Viabahn grafts, 2 patients were in Rutherford clinical grade 5 and 2 patients in Rutherford clinical grade 4, the remaining 3 patients were in Rutherford clinical grade 3 previous to therapy. Two patients with occluded grafts had interrupted the antiplatelet therapy because of other surgical procedures. Failed Viabahn grafts were treated with thrombectomy alone (3 limbs) and additional implantation of new Viabahn grafts (5 limbs) or conservatively (4 limbs). The mean pretreatment ABI improved significantly from 0.52 ± 0.16 to 0.71 ± 0.23 at the follow-up (P < .01).
In the pAKB group, 5 cases of bypass failure due to thrombosis were noted during the follow-up. Graft failure occurred after a mean time of 7 ± 3.9 months. One of these patients had Rutherford clinical grade 5; the remaining patients had shown Rutherford clinical grade 3 prior to therapy. All occluded grafts were successfully treated with thrombectomy. The mean pretreatmental ABI improved significantly from 0.54 ± 0.13 to 0.84 ± 0.17 at the follow-up (P < .01).
Primary and secondary patency rates calculated by the Kaplan-Meier method were 60% and 90% in the Viabahn group and 78% and 91% in the pAKB group, respectively (Figures 1 and 2). No statistical difference was found between the 2 graft groups. Leg salvage and survival were 100% in both the groups.
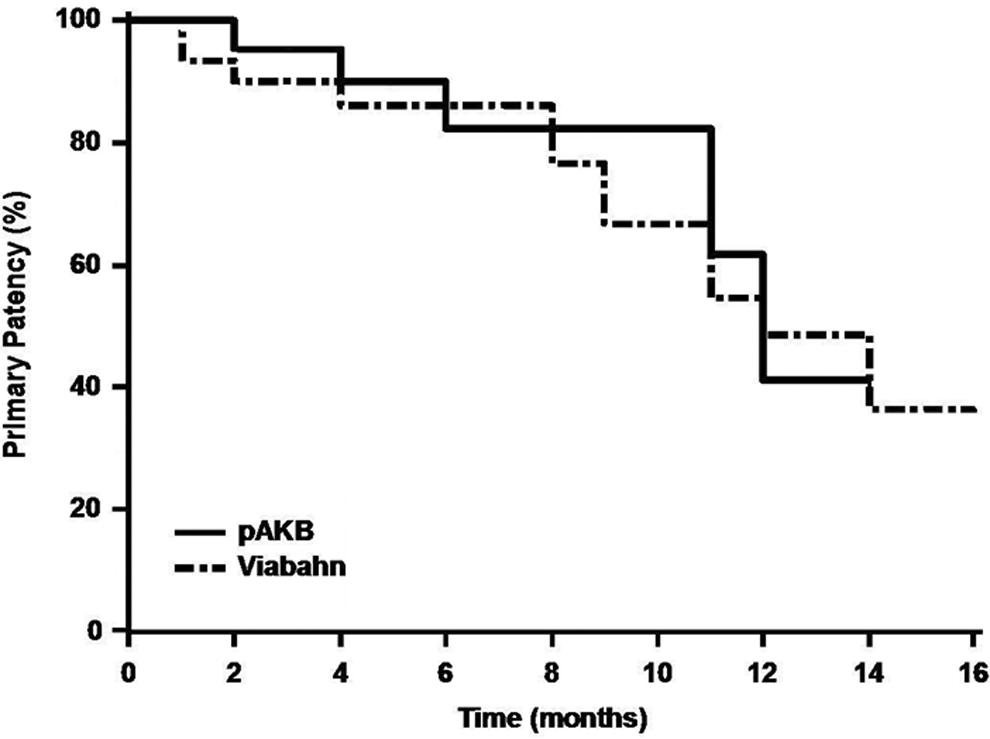
Short-term primary patency during follow-up by Kaplan-Meier analysis (log-rank test: P > .05).
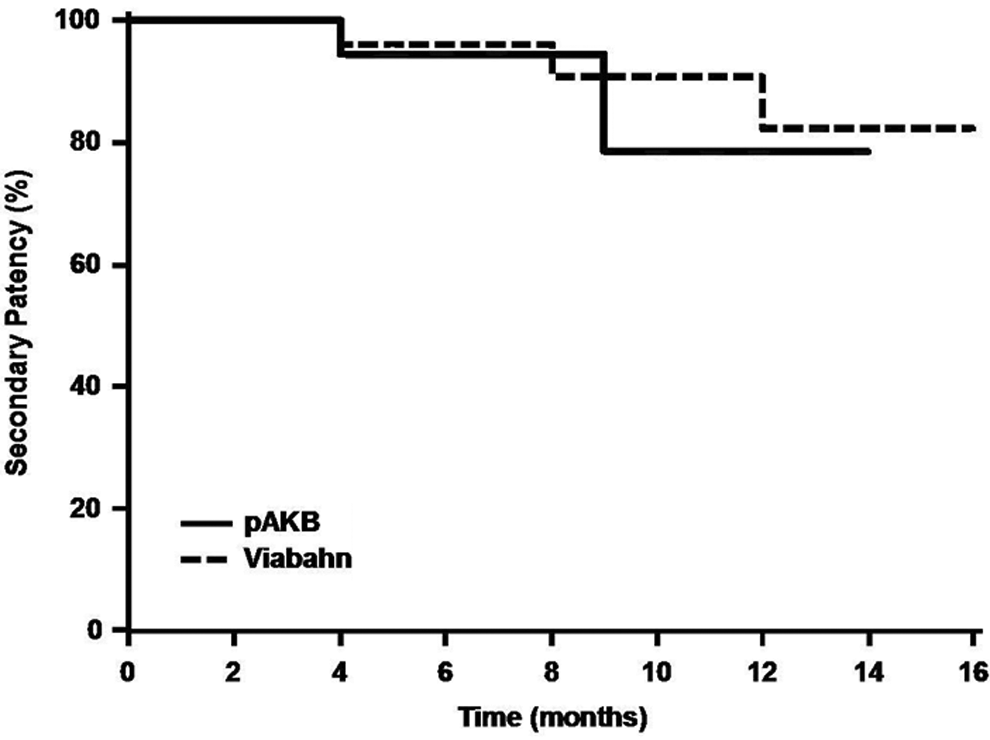
Short-term secondary patency during follow-up by Kaplan-Meier analysis (log-rank test: P > .05).
Mid-Term Results
The overall mean follow-up was 24.5 (1-68) months . In the Viabahn group, failure was observed in 16 (53%) cases after a mean time of 12 ± 8.9 months. Five graft failures occurred beyond the first year of follow-up. The majority (n = 11) of the patients with graft failure had Rutherford clinical grade 3. The remaining 3 patients had presented with grade 4, and 2 patients with grade 5. 11(69%) were treated successfully. Intervention procedures included additional implantation of new Viabahn due to progression of disease (n = 9), solely thrombectomy (n = 3), and implantation of surgical bypass (n = 1). Three patients were treated conservatively. The mean ABI remained significant when compared to the preprocedural ABI (0.52 ± 0.16 vs 0.72 ± 0.25, P < .01).
The pAKB group showed a total of 9 (36%) graft failures due to thrombosis. Graft failure appeared after a mean of 20.1 ± 15.6 months. Four graft failures occurred beyond the first year of follow-up. The remaining 5 were seen within the first year of follow-up. Only 1 of the patients with graft failure had shown Rutherford clinical grade 5; the remaining had Rutherford clinical grade 3 prior to treatment. Four patients were treated successfully after a reintervention. Redo procedures included solely thrombectomy (n = 6), implantation of Viabahn at the level of the distal anastomosis (n = 2), and surgical bypass (n = 1). The mean ABI was still superior when compared to the pretreatmental ABI (0.54 ± 0.13 vs 0.81 ± 0.19, P < .01).
Primary patency rates calculated by the Kaplan Meier method were 47% in the Viabahn group and 65% in the pAKB group (Figure 3). This difference proved to be statistically significant (P < .05). Secondary patency rates in the Viabahn group did not differ significantly from the pAKB group as shown in Figure 4 (83.3% vs 90%, P > .05). Leg salvage and survival were 100% in both the groups.
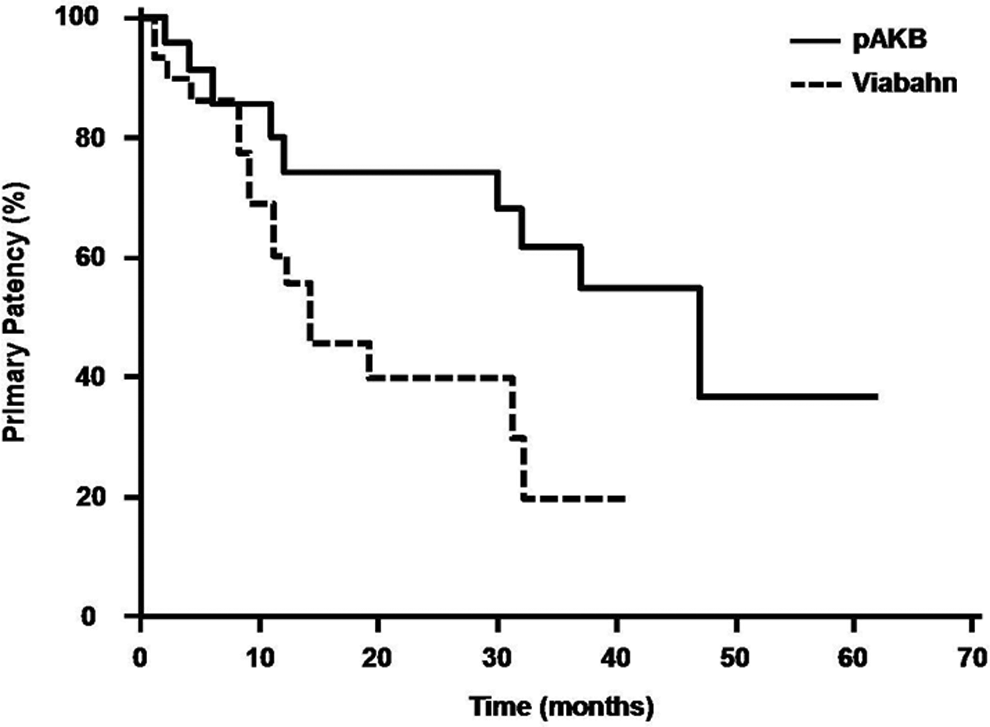
Mid-term primary patency during follow-up by Kaplan-Meier analysis (log-rank test: P < .05).
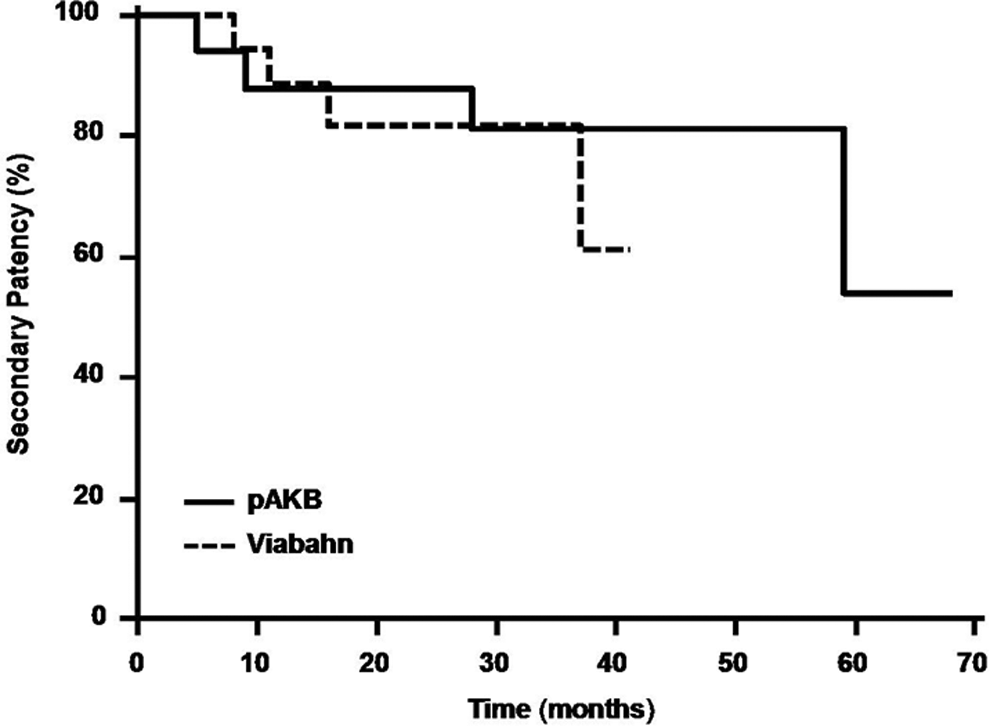
Mid-term secondary patency during follow-up by Kaplan-Meier analysis (log-rank test: P > .05).
Discussion
With continuing technical advances in the field of endovascular treatment, the traditional surgical procedure to treat SFA disease is challenged more and more. The latter requires open arterial bypass where the autologous vein is still considered by the majority as the gold standard choice of bypass conduit. This assumption which is also our belief is confirmed by numerous reports. 13 –15 However, synthetic graft material such as Dacron or ePTFE is often used instead of autologous vein due to various reasons. The absence of suitable venous material in some patients inevitably leads to the use of synthetic grafts. Some surgeons believe that using vein is more time consuming; others intend to preserve the vein for below-knee bypasses, where it provides superior results compared to synthetic grafts. 16 –18 Among synthetic grafts, the use of Dacron or ePTFE has not shown any significant difference in outcome. 19,20 The technological improvement and development of endovascular surgery have been providing a less invasive option to treat SFA disease. Starting to treat SFA disease with PTA resulted in moderate patency results, 21 and subsequent step-up with self-expanding nitinol stents could provide slightly better results. 22 –24 However, late clinical failure caused by in-stent stenosis and stent fracture raised considerable concern. 25 With the introduction of endovascular prosthesis for peripheral occlusive disease (Hemobahn, later Viabahn, W L Gore, Flagstaff, Ariz), higher patency rates and reduced delayed stent graft failure could be achieved. 3,5 –7,26 Having these encouraging results presented in numerous reports, the question emerges whether the open bypass surgery can be replaced by the less invasive endovascular treatment. Since reports about comparison of these 2 therapeutic modalities are still scarce, we intended to compare the efficacy of the Viabahn graft with the surgical AKB for the treatment of SFA occlusive disease.
The technical success rate in both the treatment groups was 100%. Short-term primary and secondary patency rates were not significantly different between both the arms. However, the primary patency rate in the Viabahn group was lower than that described in previous published reports. 4,10,27 Although mid-term secondary patency rates were similar in both the treatment groups, the primary patency rate was significantly less in the Viabahn group. Although our results differ partially from previous studies comparing Viabahn with pAKB, they in general confirm former published reports. 4,10 Lower patency rates in the Viabahn group can be explained by a significantly higher Rutherford clinical grade of limb ischemia, long mean-treated lesion length, and a significantly smaller graft diameter. Certainly, a learning curve in the beginning and the tendency to cover only the portion of the SFA, which has been treated by angioplasty and no angioplasty outside the covered area, have to be mentioned. The hospital stay in the Viabahn group remains significantly shorter compared to the pAKB as reported in other investigations. 10,11
Although our study has several recognized limitations including the retrospective character of our study, lack of randomization, small total patient number, and a single-center experience, we could show a comparable secondary patency by implantation of endovascular prosthesis with a less invasive procedure and with shorter hospital stay making this procedure cost effective. Considering the fact that patients with peripheral arterial disease are high-risk patients and hospital reimbursement is an important issue, these 2 advantages have to be taken into concern.
Conclusion
In conclusion, the pAKB surgery remains a good choice for the treatment of SFA disease. However, endovascular treatment is a sincere alternative option to open bypass surgery, especially in the absence of autologous vein. It is less invasive and reduces the hospital stay. The choice of treatment modality remains a point of discussion. Further clinical trials comparing stent grafts with bypass surgery are warranted to enrich this discussion.
Footnotes
Authors’ Notes
This study was presented at the 61st International Congress of The European Society for Cardiovascular and Endovascular Surgery; April, 2012 (oral presentation), and at the 28th Congress of German Society for Vascular Surgery; October, 2012 (ePoster).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.