
Abstract
Vein graft stenosis is a well-recognized complication of infrainguinal bypass surgery. Balloon angioplasty is an accepted method for managing vein graft stenosis in selected patients. This intervention is not without complication. We present 2 cases of delayed pseudoaneurysm formation after balloon angioplasty of vein graft stenoses. Both cases showed a persistent contrast stain or blush as an indication of vein wall damage and propose that this is a radiological harbinger of delayed rupture and pseudoaneurysm formation.
Keywords
Introduction
Infrainguinal bypass is vulnerable to stenosis with the potential for limb loss. 1,2 Surveillance of patients who have undergone bypass allows early detection of graft stenosis and the potential for graft and limb salvage. 3
For grafts that are threatened by stenosis, surgery has long been seen as the gold-standard treatment modality, 4,5 but balloon angioplasty has been shown to be safe with an acceptable medium-term patency rate. 6,7 This intervention is commonly performed in selected patients as a first-line procedure. 8 Balloon angioplasty is not without complication. Risks include vessel rupture, hematoma, and pseudoaneurysm as well as systemic, embolic, and puncture site complications. 9,10 Early identification of the potential complications could allow close surveillance and prompt treatment and reduce the risk of surgical intervention with its associated morbidity and mortality and allow for limb and graft salvage.
We present 2 cases of patients who underwent balloon angioplasty for vein graft stenoses that were subsequently complicated by vessel wall damage and pseudoaneurysm formation. Both the patients showed a blush-like enhancement of contrast at the site of wall damage during the initial procedure. We propose that this stain of contrast or blush sign is a radiological marker of delayed vessel rupture and pseudoaneurysm formation.
Case 1
A 72-year-old male with arteriopathy who underwent a redo left femoral to posterior tibial bypass with cephalic vein presented 7 months later for routine graft surveillance. Duplex scan demonstrated a tight stenosis in the proximal graft. Catheter angiography confirmed this showing a mild stenosis at the proximal anastomosis, a tight stenosis in the upper thigh, and a further mild stenosis in the distal thigh (Figure 1).

Digital subtraction angiogram demonstrating moderate stenosis of the proximal anastomoses with tight beaded stenosis within the body of the graft 7 months post bypass graft.
The stenoses were dilated with a 5-mm angioplasty balloon. However, there was significant residual balloon wasting at 14 atm in the mid and distal thigh lesions leaving a significant residual stenosis.
A 5 mm × 2 cm cutting balloon was used to overcome this to good effect.
Following cutting balloon angioplasty, there was noted to be a small area of persistent enhancement of contrast (Figure 2). This blush of contrast settled with 5-mm balloon tamponade.

Digital subtraction angiogram after dilatation with a 5-mm cutting balloon. There is a blush of contrast at the angioplasty site (arrow).
Approximately 2 hours postprocedure, the patient developed sudden onset thigh pain with an associated pulsatile mass. There was no hemodynamic compromise. Arterial duplex suggested pseudoaneurysm, and computed tomography angiogram (CTA) confirmed a large pseudoaneurysm arising from the vein graft at the site of the proximal thigh stenosis.
The patient was taken back to angiography, and a covered stent graft was inserted. During deployment of the 7 × 100 mL Viabahn (WL Gore, USA) stent graft, the thigh was compressed with a sphygmomanometer cuff in order to exsanguinate the sac and reduce its mass effect. The stent was postdilated with a 5-mm balloon. There was a good angiographic result, and graft runoff was preserved (Figure 3A-C).
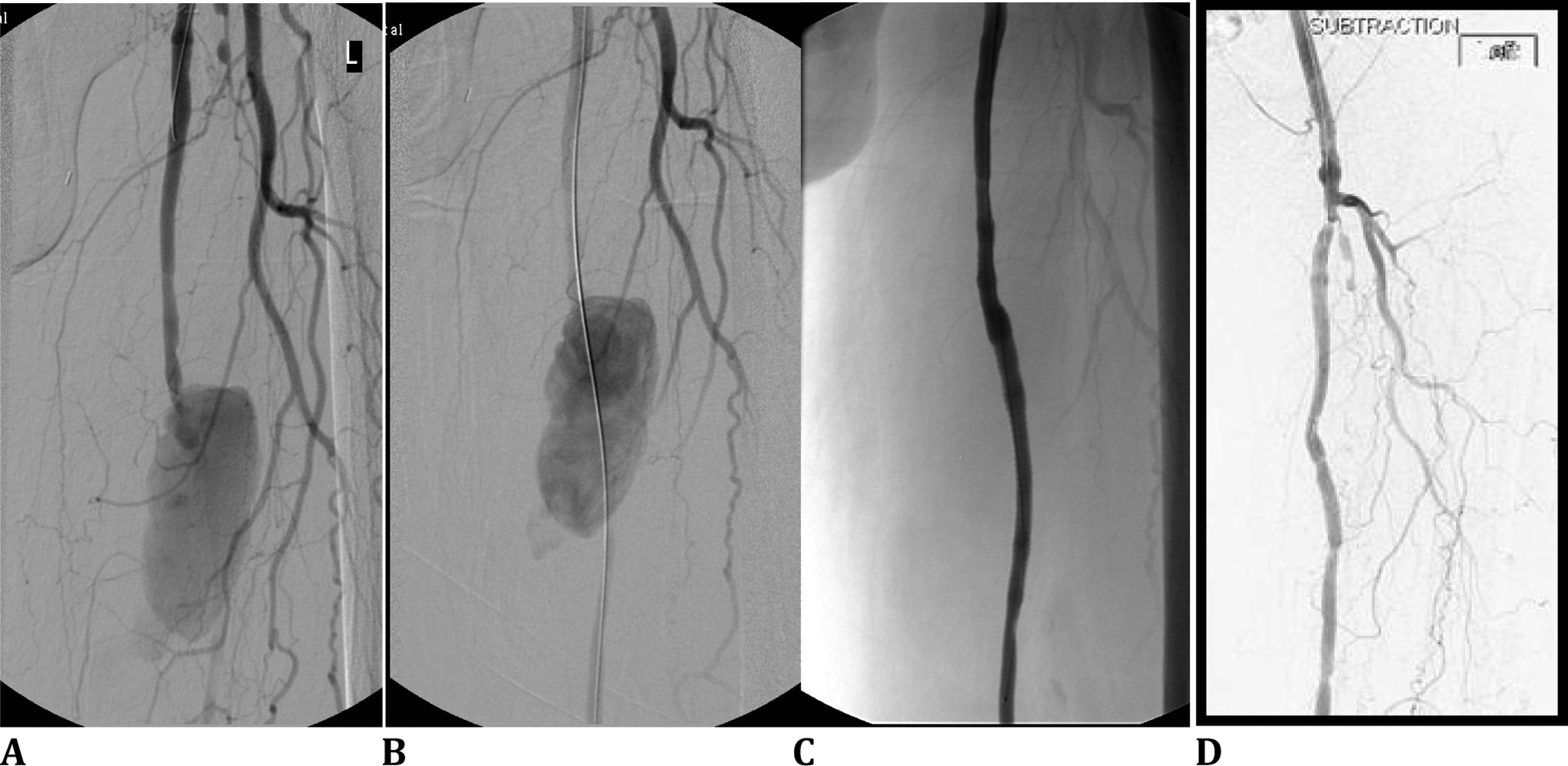
A, Digital subtraction angiogram shows contrast filling of a large pseudoaneurysm sac. B, The passage of a guidewire across the neck of the sac. C, Completion digital subtraction angiogram (DSA) following placement of Viabahn covered stent graft device. D, Follow-up DSA after 3 years.
The patient remained under routine graft surveillance for 3 years and recently attended for angiography and repeat angioplasty of a proximal anastomotic stenosis (Figure 3D).
Case 2
A 63-year-old male heavy smoker was under surveillance for a femoral to peroneal artery bypass with an ipsilateral long saphenous vein graft. Duplex graft surveillance at 4 months detected proximal graft stenosis.
Balloon angioplasty was performed twice in the following 4 months for recurrent graft stenosis before he presented as an emergency to the clinic with short distance claudication of the affected leg. A further angiogram demonstrated occlusion of the common femoral artery and graft, and he proceeded to undergo common femoral artery endarterectomy with vein patch angioplasty and embolectomy of the graft.
He continued to smoke heavily and presented 6 months later as an emergency with graft reocclusion. A heparin infusion was commenced, and an angiogram was performed confirming the clinical diagnosis of an occluded graft (Figure 4A). Mechanical thrombolysis was carried out using the AngioJet thrombectomy device (Medrad inc, Warrendale, Pittsburgh; Figure 4B.
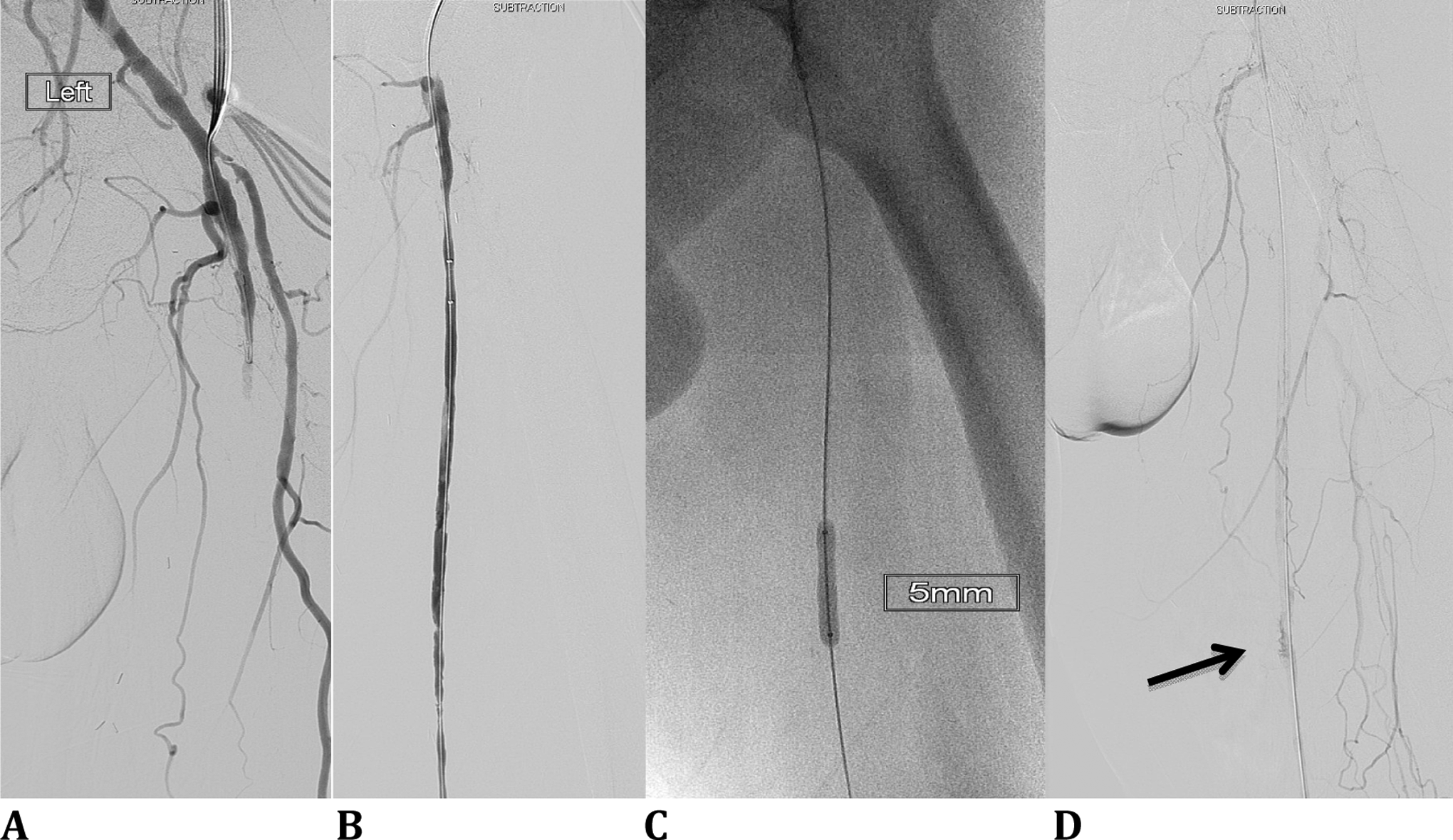
A, Antegrade digital subtraction angiogram demonstrates vein graft occlusion. (B) during AngioJet mechanical thrombolysis, (C) during balloon angioplasty, and (D) postangioplasty showing the persistent contrast blush (arrow).
The multiple stenoses within the main body of the vein graft were dilated with 4-mm and 5-mm balloons to good effect (Figure 4C). He was well postprocedure, commenced on Warfarin, and discharged home. A few days later he developed thigh pain and was seen in the vascular clinic. Duplex surveillance demonstrated a 3.4-cm false aneurysm arising from the graft. The CTA showed a significant 7-mm long defect in the vein.
A review of the previous digital subtraction angiogram images showed a persistent contrast blush in the same segment following recent balloon angioplasty (Figure 5A).

A, Subsequent digital subtraction angiogram demonstrating the vein graft pseudoaneurysm, (B) after endovascular repair with Viabahn stent graft device.
A 5 × 100 mm Viabahn covered stent graft was deployed across the defect and postdilated with a 5-mm balloon. Postprocedure angiogram showed a good result (Figure 5B) with 2 vessel runoff. The patient remains on Warfarin, and 6 months postprocedure his graft remains patent with good triphasic signal in the peroneal artery and no further graft-related stenosis.
Discussion
Balloon angioplasty is now commonly used in the management of failing infrainguinal grafts. Complications are likely to be encountered with increasing frequency, as the use of endovascular techniques increases. Early recognition of complications may allow for prompt treatment with reduced patient morbidity and mortality, especially important as endovascular interventions are frequently performed as day case procedures.
There are no published reports of radiological markers signaling potential delayed false aneurysm formation.
We propose that the persistent stain of contrast seen in these 2 cases following balloon angioplasty is a likely indicator of delayed vessel wall rupture and false aneurysm formation. Observation of this sign should lead the clinician to have a high index of suspicion that pseudoaneurysm may form. The patient may then be actively monitored for this and treated promptly minimizing the risk to the patient.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.