
Abstract
This study investigates whether ethnic minorities presenting with critical limb ischemia (CLI) are more likely to undergo major limb amputation compared to white patients. The Nationwide Inpatient Sample (NIS) database was used to identify all patients admitted with CLI; lower extremity revascularization; and major lower extremity amputation from 1998 to 2005. The NIS identified 240 139 patients presenting with CLI—68.2% white, 19.5% black, 9.0% Hispanic, and 1.24% Asian. In all, 83 328 patients underwent revascularization—73.7% white, 15.9% black, 7.4% Hispanic, and 1.1% Asian. The majority of the interventions were open. In all, 111 548 patients underwent a major lower extremity amputation—61% white, 25.4% black, 10.1% Hispanic, and 1.1% Asian. The mean Charlson comorbidity scores for amputation were 2.1 for whites, 2.0 for blacks, 2.3 for Hispanics, and 2.5 for Asians (for all data, P < .05).
Introduction
Several previous reports have shown that black patients are at a higher risk of undergoing a major lower extremity amputation as compared to white patients. 1–4 It has been noted that blacks are 2 to 4 times more likely to undergo an above- or below-knee amputation as compared to non-Hispanic whites. 1 It has also been reported that black patients are less likely to undergo lower extremity arterial revascularization procedures as compared to whites. 3,4 This study was undertaken in an attempt to evaluate the extent of this disparity in recent times and to determine whether an increase in the adoption of endovascular techniques 5 may have had an impact on this.
Methods
Three independent queries were performed of the Nationwide Inpatient Sample (NIS) database to identify (1) all patients who had been admitted with critical limb ischemia (CLI; International Classification of Diseases, Ninth Revision [ICD-9] 440.23 and ICD-9 440.24); (2) all patients who had undergone an open (ICD-9 39.25 and ICD-9 39.29) or a percutaneous (39.90 and 39.50) lower extremity revascularization procedure; and (3) all patients who had underwent a major lower extremity amputation (ICD-9 84.15 and ICD-9 84.17). The period of study was 1998 to 2005. Demographic data and comorbid conditions were recorded. Cardiac comorbidity was defined as the presence of congestive heart failure or coronary artery disease and a history of previous coronary revascularization. Pulmonary comorbidity was defined as the presence of an existing pulmonary diagnosis. Renal comorbidity was defined as dialysis-dependent end-stage renal failure; and diabetes mellitus was defined as a diagnosis of type I or type II insulin-dependent or noninsulin-dependent diabetes. Comparisons were done between the different ethnic groups—white, black, Hispanic, and Asian—in each of these queries. Statistical analysis was done using chi-square and Student t test to compare the differences among the groups and differences in the group means, respectively.
Results
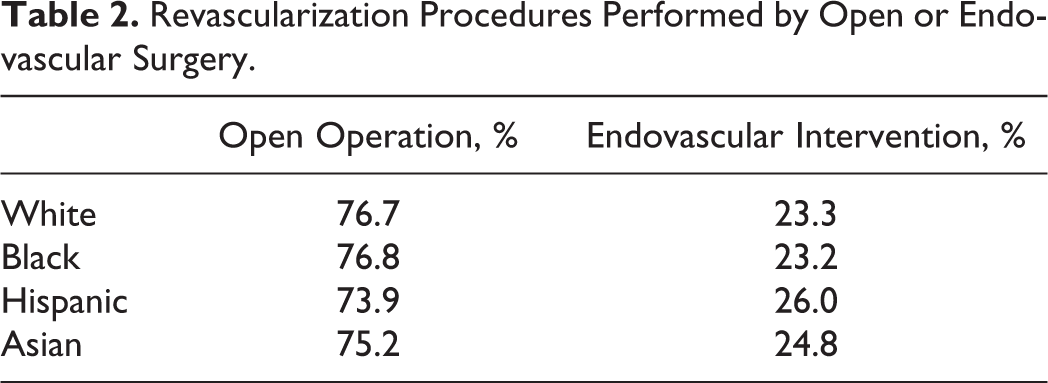
The first NIS query identified 240 139 patients presenting with CLI. Of the 186 239 (77.6%) patients who had ethnicity data, there were 68.2% white, 19.5% black, 9.0% Hispanic, and 1.2% Asian patients. The second NIS query identified 365 795 patients undergoing open or endovascular revascularization during the study period. Among these, 83 328 (22.8%) patients had CLI as their presenting diagnosis—that is, 22.8% of the revascularization procedures were performed for CLI. Of the 63 639 (76.4%) of these for whom ethnic data were available, 73.7% were white, 15.9% black, 7.4% Hispanic, and 1.1% Asian (Table 1). In all, 76.7% open and 23.3% endovascular interventions were performed in whites; 76.8% open and 23.2% endovascular interventions in blacks; 73.9% open and 26.0% endovascular interventions in Hispanics; and 75.2% open and 24.8% endovascular interventions in Asians. A third query of the NIS during the study interval showed that 111 548 patients underwent a major lower extremity amputation. Among the 84 498 (75.85) patients undergoing a major amputation who had race data recorded, 61% were white, 25.4% black, 10.1% Hispanic, and 1.1% Asian. Of note, overall 98% of the patients possessed some form of insurance.
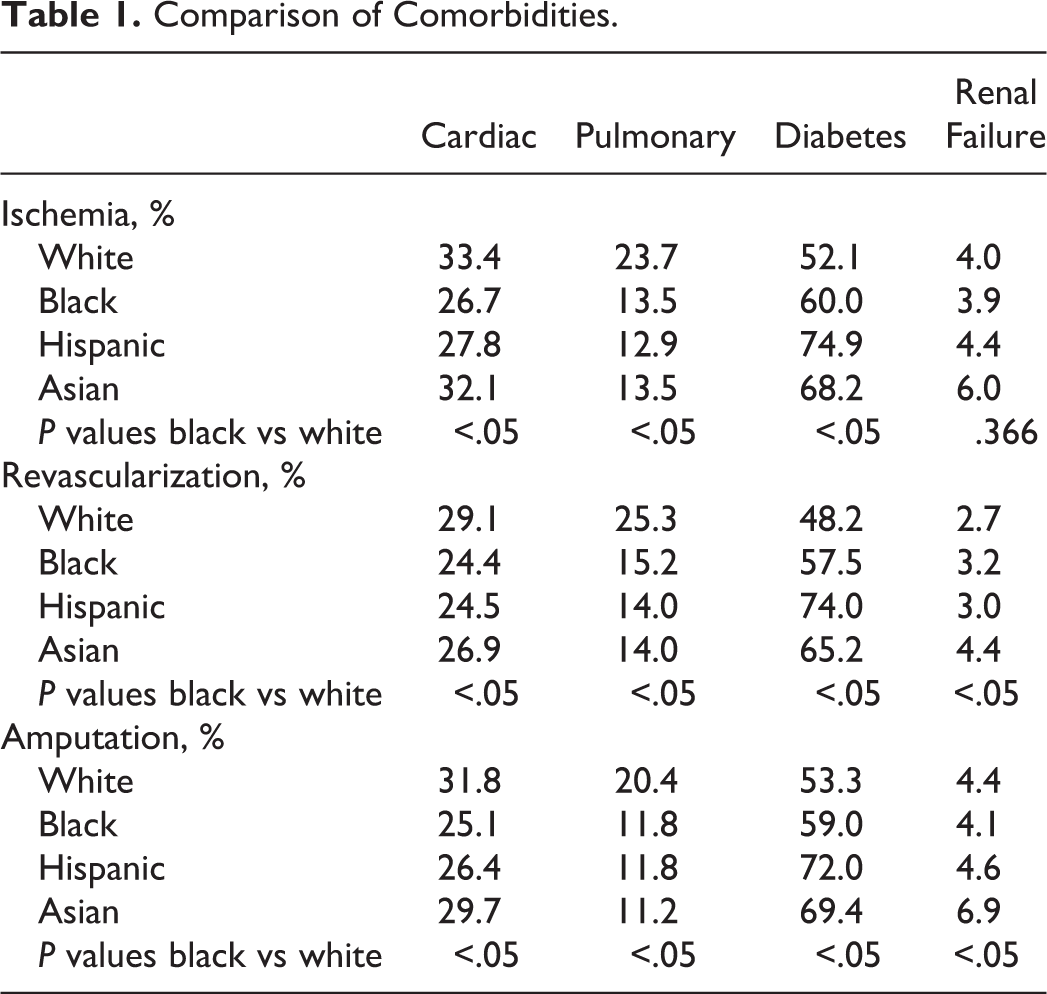
Comparison of Comorbidities.
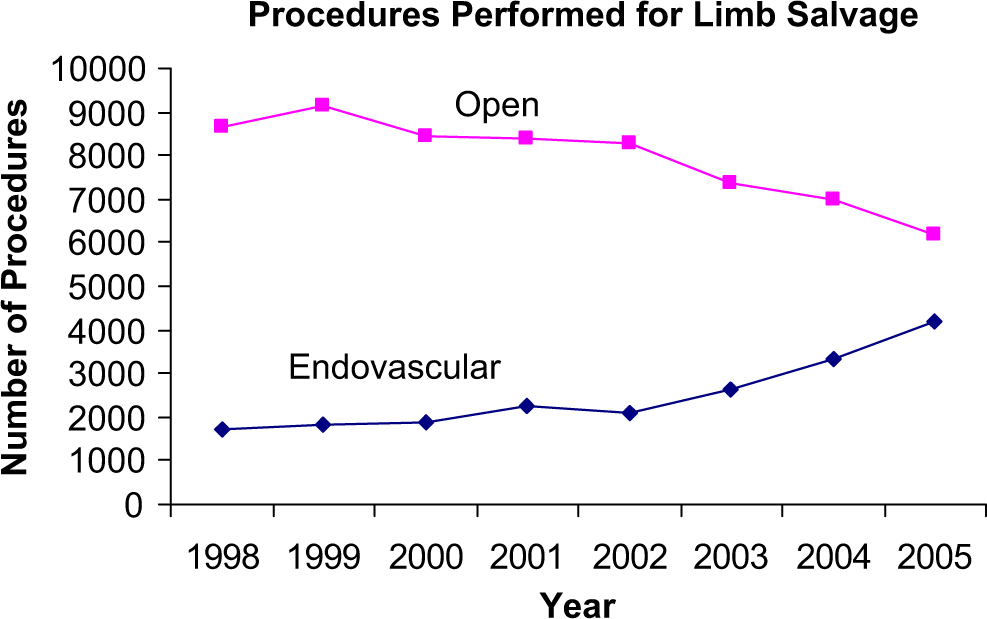
The percentage of open versus endovascular interventions performed among the different ethnic groups seemed to be comparable over the study period with about three-fourths of the procedures being performed open and a quarter being performed with endovascular techniques (see Table 2). Not surprisingly, a trend toward an increased use of endovascular interventions for CLI was noted among all ethnic groups with these interventions comprising 16.6% of procedures for CLI in 1998 as compared to 40.3% in 2005 (see Figure 1).
Patients with critical limb ischemia revascularized via open or endovascular surgery.
Revascularization Procedures Performed by Open or Endovascular Surgery.
When black and white patients were examined with respect to specific comorbidities (Table 1), there were consistent, statistically significant differences among the categories of cardiac and pulmonary comorbidities and the presence of diabetes mellitus. Whites were always more likely to have more cardiac and pulmonary comorbidities for patients presenting with CLI, patients undergoing revascularization as well as patients undergoing amputation. On the other hand, blacks were more likely to have diabetes mellitus across all the 3 queries. Dialysis-dependent renal failure was more likely to be present in whites undergoing amputation as compared to blacks; on the other hand, blacks undergoing revascularization were more likely than whites to have dialysis-dependent renal failure. There was no statistically significant difference in the incidence of dialysis dependence between blacks and whites for patients presenting with CLI.
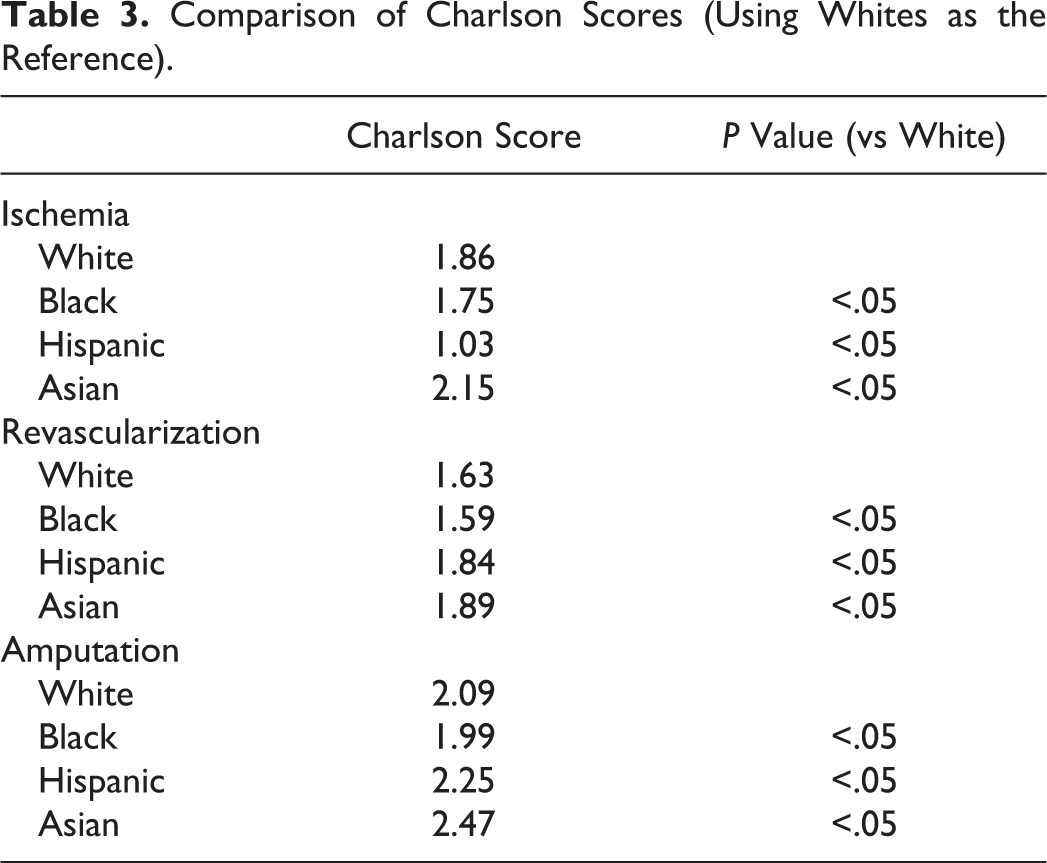
In an attempt to determine an overall comorbid status for these groups of patients, the mean Charlson comorbidity scores for the different ethnic groups were determined (Table 3). Using whites as a reference, the Charlson score differences among the ethnic groups were compared, and statistical significance was achieved across all the groups, that is, blacks were significantly healthier than whites in all categories, whereas Asians and Hispanics were less healthy than whites in the revascularization and amputation categories.
Comparison of Charlson Scores (Using Whites as the Reference).
Discussion
The NIS, developed as part of the Healthcare Cost and Utilization Project, is the largest all-payer inpatient care database in the United States containing data from approximately 8 million hospital stays each year. It comprises about 20% of all hospital discharges. A major strength of this study is the very large sample size, and the fact that it includes patients with all types of insurance as well as the uninsured. Our study shows that there remains a significant racial disparity in the treatment of peripheral arterial disease (PAD) with blacks undergoing a disproportionately higher number of major lower extremity amputations (overall 25% of amputations for a population comprising only 20% of the total).
This observed ethnic disparity in the treatment of PAD is not a novel concept, having been previously recognized by other studies. 1–4 Notably, Huber et al showed that although the incidence of treatment for the complications of PAD was comparable for white and black patients in the state of Florida, whites were more likely to be treated with revascularization, while blacks were more likely to be treated with amputation. 4 On a national level, Guadagnoli et al reporting from a 20% sample of Medicare beneficiaries (n = 19 236; 1989-1990; age > 64) also showed that blacks were more likely to undergo all types of lower extremity amputation but less likely to undergo angioplasty or surgical revascularization. 3 More recently, Feinglass et al have shown that racial disparities in lower extremity amputation rates have remained remarkably constant in a Northern Illinois population. It appears, unfortunately, that nationwide there has also been little improvement in this disparity over the last decade or so. It is interesting to note that the percentage of amputations attributed to the black population in our study—25%—is virtually identical to what was reported in 1996—25% of amputations—though blacks comprise just over 12% of the US population. 6 Traditionally postulated reasons for this disparity have included ethnic variations in disease distribution, differential access to care, and distrust in the medical system by some in the black community.
Because of an underlying belief that an increased incidence of prohibitive comorbidities might render blacks as less attractive candidates for revascularization, 7–9 we examined comorbidities comparing blacks to whites and were surprised to find that whites were significantly more likely than blacks to have cardiac and pulmonary comorbidities in all the 3 presentation categories (Table 1). As has been reported previously, 10 blacks on the other hand were more likely than whites to have diabetes mellitus also in all 3 presentation categories than whites. The Charlson comorbidity score index 11 (a measure of the overall comorbid status of a patient) was determined for the different ethnic groups, and blacks were found to have a statistically significantly lower Charlson comorbidity index than whites for all the 3 presentation categories (ie, blacks were healthier than whites; Table 2). It is important to note, however, that the overall low Charlson scores and the very small differences among the different racial groups would suggest that although statistical significance may have been achieved, these differences are likely not clinically meaningful. This is 1 potential disadvantage of such a large sample size, whereby fairly inconsequential clinical differences are determined to be statistically significant.
We did not separate out infrainguinal bypass procedures from aortoiliac procedures, and so we could not specifically corroborate the findings of Brothers et al, 12 Sidawy et al, 13 and other authors about the greater findings of infrainguinal disease in black patients. Given the higher incidence of diabetes in our black population, we would likely expect this to be so. In fact, it is quite possible that a higher incidence of diabetes in blacks may lead to this patient population being referred less often for revascularization. Despite multiple studies showing that patients with diabetes do just as well with peripheral revascularization 14–17 as nondiabetics, the antiquated concept of “small vessel disease,” 18 although successfully refuted, 19–21 continues to persist and remains responsible for unnecessary amputations in so many patients with diabetes presenting with foot ischemia.
It is noteworthy that once being selected for revascularization, blacks undergo endovascular intervention at the same rate as whites (Table 3). One could, thereby, be tempted to conclude that the level of sophistication of vascular care may, therefore, be just as high for blacks as it is for whites. On the other hand, the probably greater incidence of tibial artery disease in blacks, as suggested by the higher incidence of diabetes, would typically be associated with a somewhat greater likelihood of failure from endovascular intervention.
Insurance status is often implicated as a predictor of health outcomes. Within the scope of this study, almost 98% of the patients’ studied possessed insurance. We could not, therefore, stratify our results against this variable. We would suggest that this does not preclude the potential implications of insurance status on patients with peripheral arterial disease as is evidenced in other contemporary literature. 22
Our findings are consistent with the report from Rowe et al employing the same database and showing that although there has been an overall increase in nationwide employment of open and endovascular interventions for PAD with a concomitant decrease in limb amputations, black and Hispanic patients remained more likely to undergo amputation. 22 That article focused on the types of treatment offered to individuals, whereas the current article focuses on the comorbidities with respect to patient outcomes. One limitation of this study is that ethnicity data were available only in three-fourths of the patients in each presentation category. It is, nonetheless, unlikely that there was a difference in the completeness of the data being collected by patient’s race or ethnicity. Another limitation is that all amputations were taken into account without exclusion. This could be problematic since some amputations are done for trauma and oncologic disease, and not all amputations are for CLI. One would hope that with such a large sample size, such differences would be minimal. Additionally, the codes used to identify “CLI” do not differentiate the severity of ischemia in temporal reference or with respect to tissue loss. Finally, additional risk factors for peripheral disease such as tobacco use were not reliably available within the database. Undoubtedly, such information would have been useful for stratification.
Conclusion
In summary, there continues to be racial/ethnic disparities in the management of CLI, with blacks being more likely to undergo major lower extremity amputations and less likely to undergo lower extremity revascularization procedures. This disparity remained across the study period and has been unaffected by the increased adoption of endovascular intervention.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.