
Abstract
Duplication of inferior vena cava (IVC) is the most common IVC anomaly. We report a successful iliac vein and collateral stenting for venous decompression in a patient with an occluded right femorocaval graft with a duplicated IVC. We also review the literature of embryological development of IVC.
Introduction
Incidence of post-thrombotic syndrome in iliofemoral deep vein thrombosis (DVT) is near 30% if treated with only anticoagulation and compression. 1 It is well known that patients with severe chronic venous insufficiency (lipodermatosclerosis and healed or active ulcer: C4b, C5, C6) can be effectively investigated by intravascular ultrasound (IVUS). 2 In most places where IVUS is not available, computed tomographic (CT) venogram or magnetic resonance venogram can be effectively used to rule out iliac vein stenosis or occlusion as a cause of secondary deep venous reflux.
The role of iliac vein stenting for symptomatic iliac vein stenosis or occlusion is also well established. 3 Unlike arterial lesions, stenting across inguinal ligament can be performed without significantly increased risk of stent deformation or in-stent stenosis. 4
We report a successful iliac vein and embryological collateral stenting for venous decompression in a patient with an occluded right femorocaval graft with a duplicated inferior vena cava (IVC).
Case Report
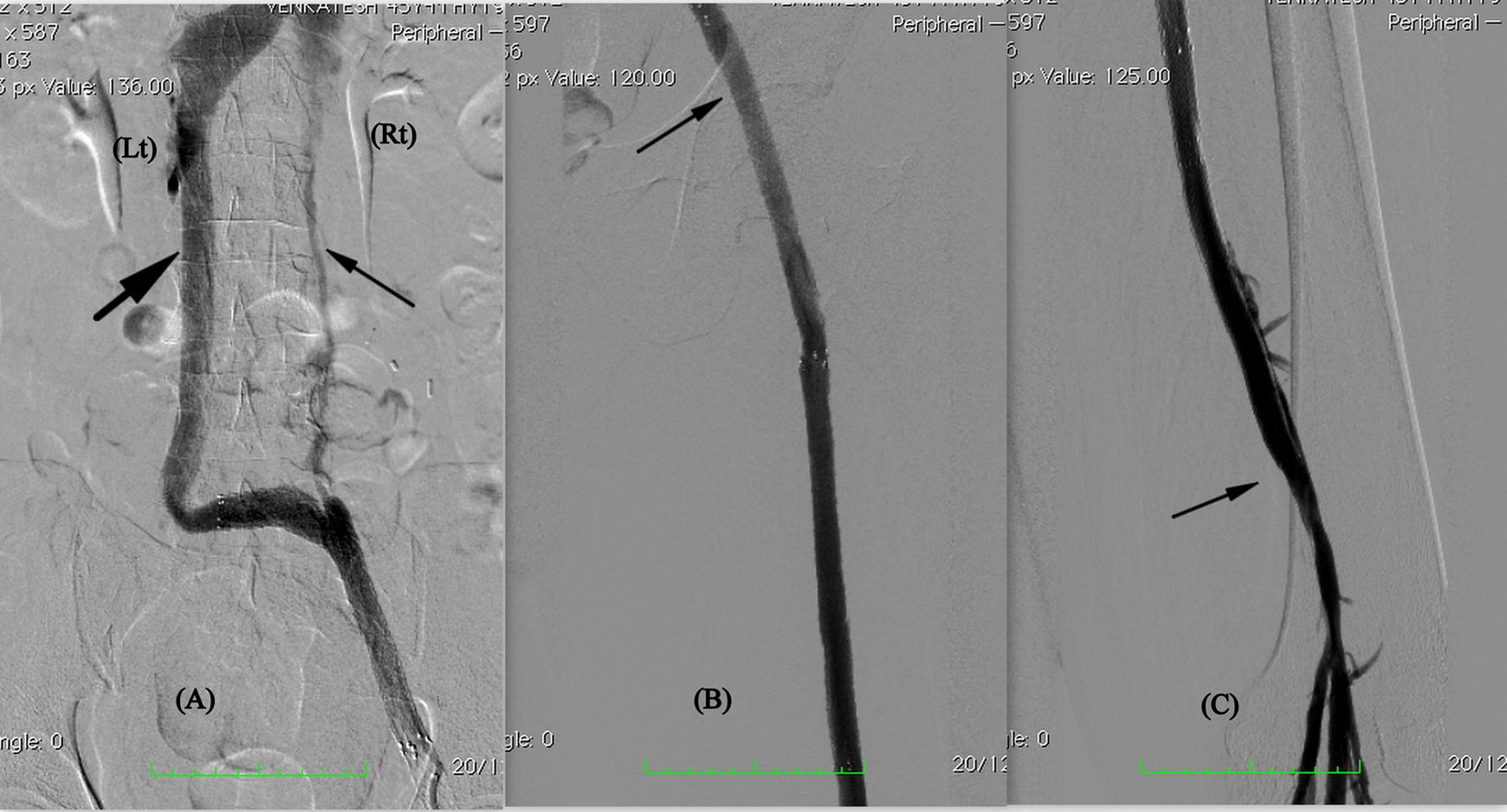
A 45-year-old male underwent a right femorocaval bypass at another center. He had a history of venous ulceration for the preceding 6 years following a posttraumatic chronic iliofemoral DVT. This ulcer was healed following surgery for the initial 2 months but worsened in size, local pain, and leg swelling thereafter. He was referred to our institute with a recurrent venous ulcer in his right leg. A CT venogram demonstrated duplication of the infrarenal IVC with chronic thrombosis of right trunk of the IVC, common iliac, external iliac, and common femoral veins. An occluded graft was also seen extending from right common femoral vein to occluded right-sided infrarenal IVC (Figure 1A). Prothrombotic workup was negative for any hypercoagulable state.

A, CT venogram showing duplicated IVC with occluded right IVC. B, Venogram with patient in prone position shows trabeculations in femoral vein, popliteal vein, and in occluded right iliac vein and (C) in patent communicating vein and left-sided IVC. CT indicates computed tomographic; IVC, inferior vena cava.
In view of his active ulcerative disease and occlusion of the graft, we decided to one more attempt an endovascular recanalization.
Under ultrasound guidance, the short saphenous vein was punctured with the patient in prone position. Venogram demonstrated chronic trabeculations in the femoral and popliteal veins with complete occlusion of right iliac veins (Figure 1B). A 0.038-hydrophilic wire was negotiated into the right common iliac vein. Venogram from this position showed a good caliber, straight, nontortuous vein joining the left common iliac vein, which was draining into a patent left IVC trunk (Figure 1C). The wire was negotiated through this communicating vein into the patent left iliac vein. Right common iliac vein, external iliac vein, and femoral vein were serially predilated with 8-, 10-, and 12-mm balloons.
A 12 × 100-mm nitinol self-expandable bare stent-Eluminexx (Bard Peripheral Vascular Inc, Tempe, Arizona) was placed across the communicating vein extending through the right common iliac and external iliac veins. Further 2 Eluminexx stents of length 10 × 100 mm (Bard Peripheral Vascular Inc) were deployed from external iliac to femoral vein and 9 × 40 and 8 × 100 mm Absolute Pro (Abbott Vascular Devices, Illinois) self-expandable bare stents were deployed in femoral vein to proximal popliteal vein. Balloon molding was done with 12, 10, and 8 mm balloons (Figure 2).
Postvenoplasty and stenting venogram.
Considering previous occlusion of bypass graft and metal stents extending to thigh, postoperatively lifelong anticoagulation was commenced with a target international normalized ratio of 2 to 3 and below-knee Class II compression stockings. Complete ulcer healing was achieved within 4 weeks. Venous duplex at 3, 6, 9, and 12 months showed patent stents with no evidence of stenosis. No recurrence of ulcer in 18 months of follow-up.
Discussion
Duplication of IVC is the most common IVC anomaly and has a reported incidence of 0.2% to 3%. 5 It is probably much commoner among patients with a DVT, and Chee et al identified IVC anomalies in 5% to 6.7% of patients (<40 years) presenting with DVT. 6
Embryological Development of IVC
Brief embryological development of IVC has been shown in Figure 3(A-D). Paired anterior cardinal veins
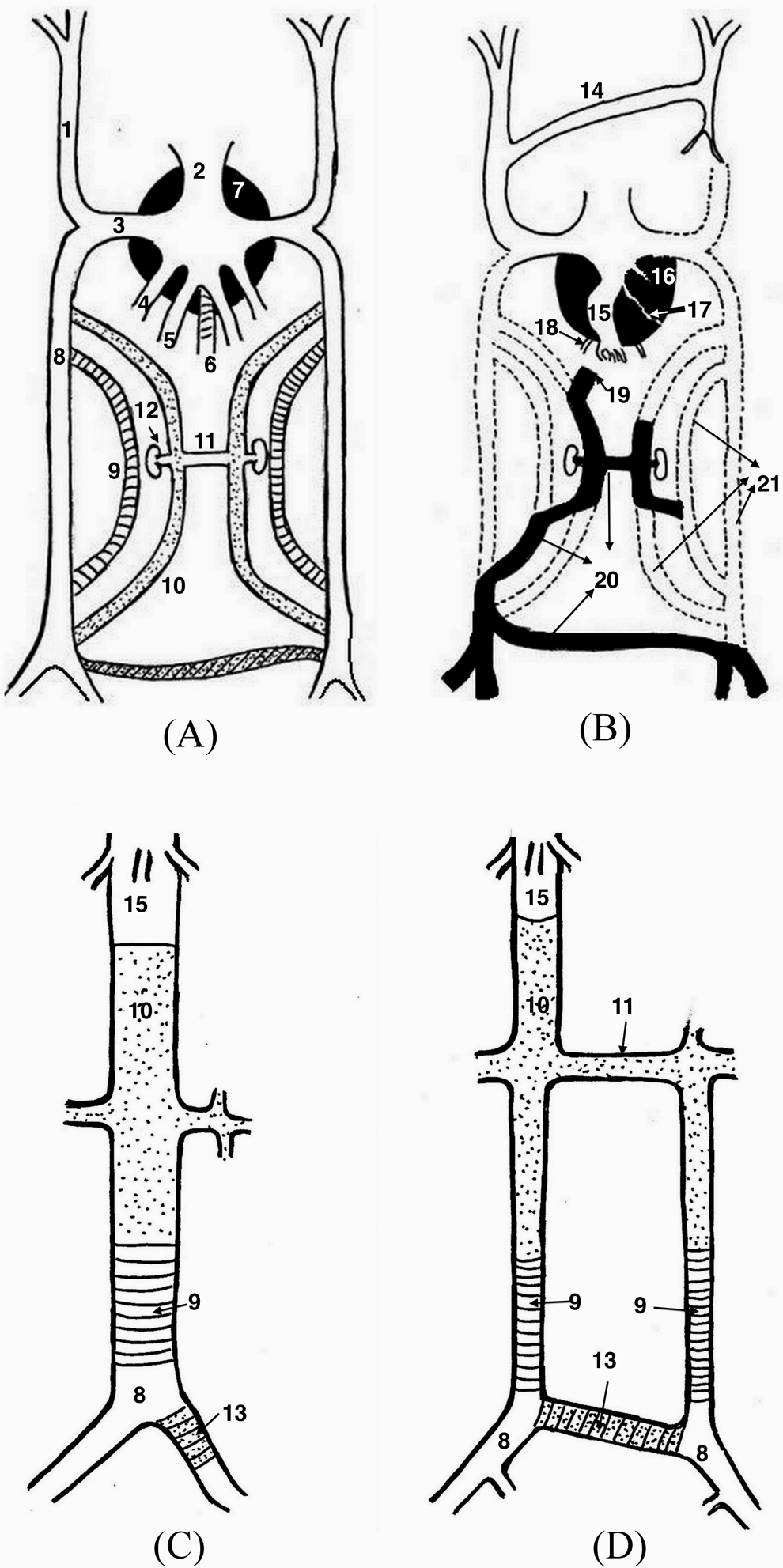
Embryology of IVC. IVC indicates inferior vena cava.
Right umbilical vein regress, and left umbilical vein forms ductus venosus which persists as ligamentum venosum
At the same time, pair of subcardinal veins
Caudally bilateral posterior cardinal veins also develop a communicating vein, future left common iliac vein
During development, parts of left-sided sub, supra, and posterior cardinal veins may not regress and form a duplicated infrarenal IVC. Interposterior cardinal vein may also persist as a communicating vein between right and left iliac veins (Figure 3D).
In our case, this communicating vein
Conclusion
In a duplicated IVC with occlusion of one of the trunks, native embryological pathways may be successfully opened up to allow venous drainage, provided adequate venous inflow has also been ensured.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.