
Abstract
Objective:
The aim was to assess the cytokine response to acute inflammation and infection in vascular surgery.
Design of Study:
Single-center, prospective cohort study.
Methods:
Blood samples from 96 consecutive patients undergoing elective vascular surgery were analyzed for C-reactive protein (CRP), total leukocyte counts (LPK), neutrophil CD64 expression, and cytokines using enzyme-linked immunosorbent assay.
Results:
Of the 25 investigated cytokines, 22 had lower postoperative mean values compared to preoperative values. Interleukin (IL) 6 (IL-6) was the only cytokine that increased significantly postoperatively. Combined analysis of CRP and CD64 together with IL-6 or IL-10 showed an individually unique association with postoperative infection (P < .05).
Conclusion:
We have shown a positive correlation with perioperative infection for the proinflammatory cytokines and the anti-inflammatory cytokine IL-10 as well as a number of chemokines. To our knowledge, this is the first report linking IL-10 and chemokine plasma levels to perioperative infection in vascular surgery.
Introduction
Postoperative infection in vascular surgery is a relatively common complication with potentially grave consequences. 1 This problem is further accentuated when prosthetic materials are used. 2 C-reactive protein (CRP) remains the most widely used biomarker for diagnosing postoperative infection; however, the quest for finding a more sensitive and specific test is ongoing.
Tissue injury, whether caused by trauma or infection, and the resultant acute inflammatory response has been the focus of extensive research. Cytokines are a group of polypeptides secreted by cells in response to injury. The role of cytokines is to organize a concerted response to tissue trauma, which involves recruitment of cells to the site of injury and instigation of a systemic response. Cytokines can generally be classified according to their role in either the acute or the chronic phase of inflammation or their specific effects on the inflammatory process, for example, stimulatory or inhibitory. Due to the pleiotrophic nature of these molecules, their interactions with different classes of immune cells are both complex and variable.
In order to better understand the clinically significant responses to surgical trauma, it is important to elucidate the underlying mechanisms that regulate the inflammatory response to this type of tissue injury. Given the central role of cytokines in regulating the immune response to tissue injury, it is reasonable to assume that by charting the perioperative variations in serum cytokine levels and their correlation with postoperative infection, a better understanding may be gained of the dynamics involved in this process.
The immune system can be broadly divided into 2 main branches—the specific and the native. The former possesses specificity and memory but is not initially efficient in eliminating bacteria unless previously primed. The native immune system recognizes bacteria through pattern recognition receptors (PRRs), such as the toll-like receptors. These receptors stimulate the secretion of proinflammatory cytokines interleukin (IL) IL-1β, IL-6, IL-8, IL-11, and tumor necrosis factor (TNF) α. 3 Both IL-1 (α/β) and TNF (α/β) are potent proinflammatory acute phase cytokines that can induce fever, cause vasodilatation, and stimulate the synthesis of IL-6. They can also be seen as potential targets in the treatment of life-threatening sepsis. 4
The native immune system includes monocytes and polymorphonuclear neutrophils (PMNs), among other cell types. Polymorphonuclear neutrophils are mainly involved in phagocytosis and are regulated by cytokines released by other immune competent cells. An example of this cytokine-mediated cross talk is the upregulation of CD64 receptors on neutrophils modulated by the release of interferon (IFN)-γ from natural killer (NK) cells exposed to IL-15 and IL-18. 5 CD64 is a potent cytotoxic trigger expressed exclusively on mononuclear phagocytes and activated PMN leukocytes. Polymorphonuclear neutrophil CD64 analysis has been shown to have a high sensitivity and specificity for the early detection of bacterial infection. 6 –10
The aim of this study was primarily to assess the cytokine response to acute inflammation caused by vascular surgery and, second, to evaluate the potential for the clinical utility of quantitative measurements of cytokines as markers for infection in conjunction with C-reactive protein (CRP) and CD64.
Patients and Methods
Patients
A consecutive series of 96 patients undergoing elective vascular surgery were analyzed in a prospective cohort study. In accordance with the normal practice at our institution, all patients received intravenously administered prophylactic antibiotics (Cefalotin 2 g × 1 preoperatively and 2 g × 2 postoperatively). All the patients included had given their informed, written consent. The study was approved by the local ethics committee.
Serum Analyses
Peripheral venous blood samples were taken preoperatively on admission and postoperatively within the first 24 hours. The samples were analyzed using enzyme-linked immunosorbent assay for the cytokines shown in Table 1.
Summary of Cytokines and a General Description of Their Major Functions and Effects.
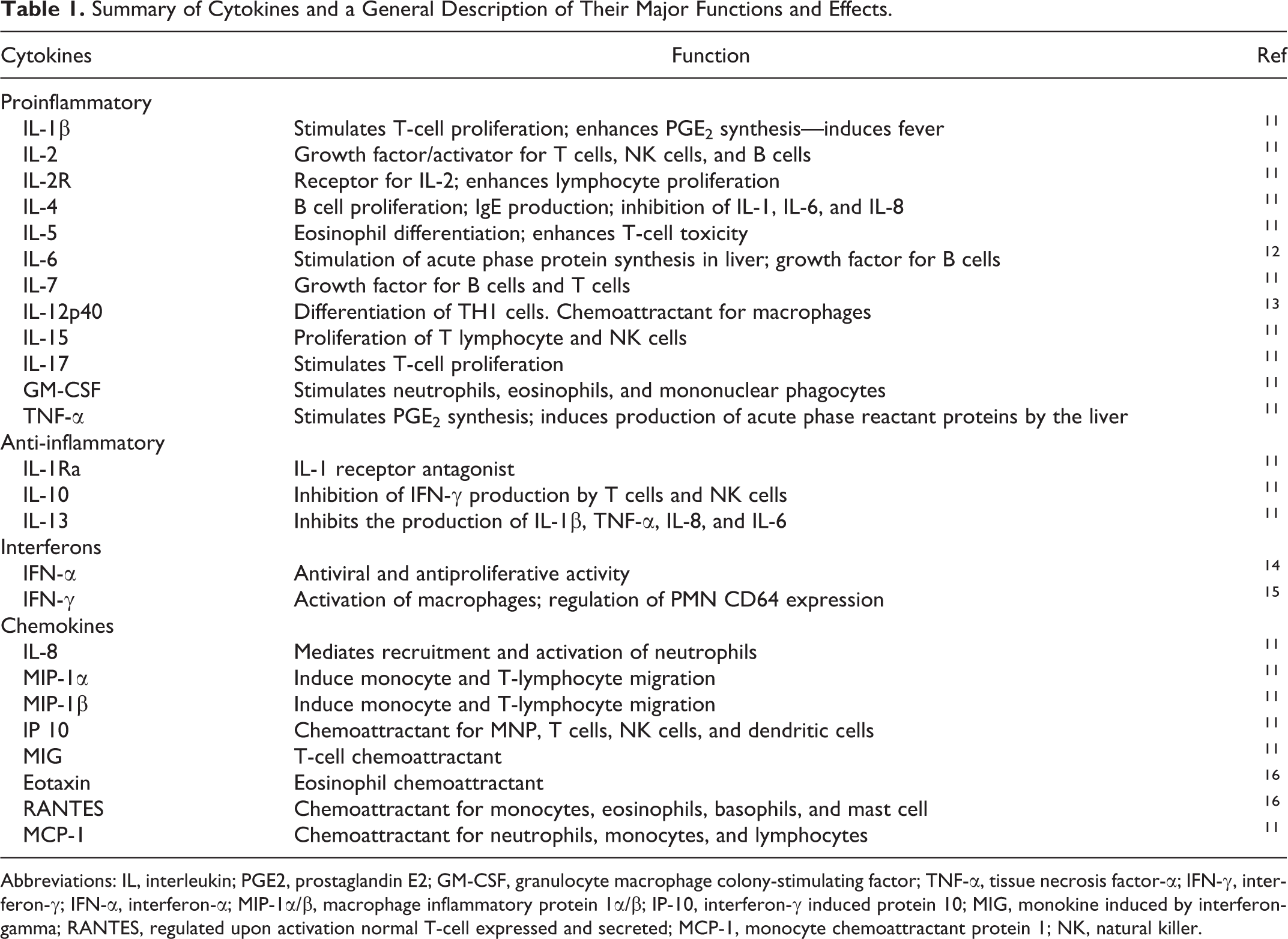
Abbreviations: IL, interleukin; PGE2, prostaglandin E2; GM-CSF, granulocyte macrophage colony-stimulating factor; TNF-α, tissue necrosis factor-α; IFN-γ, interferon-γ; IFN-α, interferon-α; MIP-1α/β, macrophage inflammatory protein 1α/β; IP-10, interferon-γ induced protein 10; MIG, monokine induced by interferon-gamma; RANTES, regulated upon activation normal T-cell expressed and secreted; MCP-1, monocyte chemoattractant protein 1; NK, natural killer.
The samples were also analyzed for CRP, total leukocyte counts (LPK), and neutrophil CD64 expression. The CRP (mg/L) and leucocyte counts (×109/L) were measured with the Cell Dyn (Abbott Laboratories. Abbott Park, Illinois, USA) Sapphire Hematology Analyzer. CD64 expression was measured using the LK64.H. Assay kit (Trillium Diagnostics, LLC: Brewer, Maine, USA) on the Cell Dyn Sapphire Hematology Analyzer. In addition to the laboratory tests, clinical parameters including body temperature, heart rate, blood pressure, and signs of local wound infection were observed and recorded. Blood and urine cultures were taken on the suspicion of infection. The diagnosis of infection, whether pre- or postoperative, was based on either a positive culture result or the presence of a clinically manifest wound infection. Fever was defined as body temperature ≥38°C.
Multiplex Cytokine Analysis
Cytokines in serum were detected using the Luminex immunobead technology, 25-plex kit (Invitrogen/Biosource, Carlsbad, California). In short, antibody-coupled beads were incubated with target analyte after which they were incubated with biotinylated detection antibody before finally being incubated with streptavidin–phycoerythrin. Samples were then read by the Luminex's laser-based fluorescent analytical test instrument Luminex 100 (Luminex Corporation Austin, Texas).The samples were analyzed for the cytokines listed in Table 1.
Statistical Analysis
The statistical program package SPSS was used (ver 18.0; SPSS Inc, Chicago, Illinois). The Pearson r, regression analysis, student t test, paired samples test, the Kruskal-Wallis, receiver–operating characteristic (ROC) analyses, and logistical regression were performed as indicated. The level for statistical significance was set at P < .05.
Due to the large variations and fluctuations in the serum levels of cytokines caused by the inherent dynamics of the immune system and the short half-life of certain cytokines, the data have been analyzed using mainly nonparametric statistical tests. This in turn precludes the use of covariates and by extension impedes the search for confounders.
Results
A total of 96 patients (71% men, n = 68; 28% women, n = 28) were consecutively included. Mean age was 71 years (range: 53-90 years). The relevant comorbidities are shown in Table 2. In the cohort undergoing vascular surgery, there were preoperative infections (n = 8), postoperative infections (n = 7), 2 of whom also had a preoperative infection, postoperative fever (n = 17), and no infection (n = 66). Vascular procedures and the related infections are shown in Table 3.
Relevant Comorbidities for the Patient Cohort.
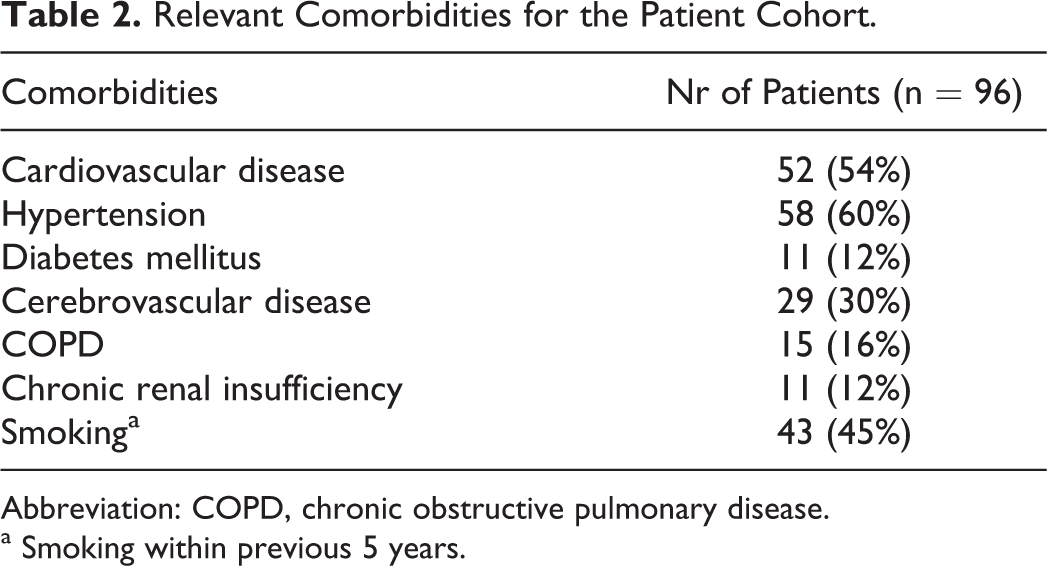
Abbreviation: COPD, chronic obstructive pulmonary disease.
aSmoking within previous 5 years.
Vascular Procedures and Related Infections.
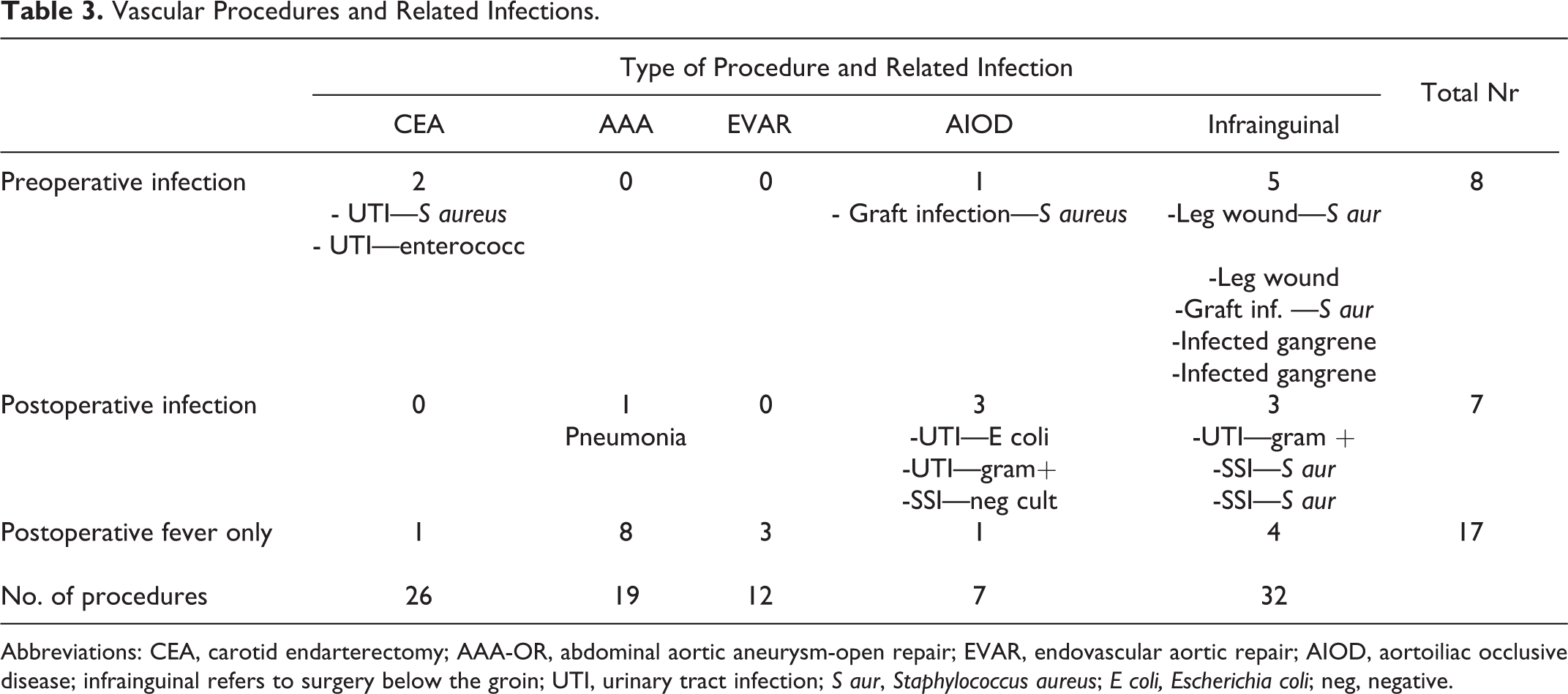
Abbreviations: CEA, carotid endarterectomy; AAA-OR, abdominal aortic aneurysm-open repair; EVAR, endovascular aortic repair; AIOD, aortoiliac occlusive disease; infrainguinal refers to surgery below the groin; UTI, urinary tract infection; S aur, Staphylococcus aureus; E coli, Escherichia coli; neg, negative.
Preoperative Versus Postoperative Cytokine Analyses
Of the 25 investigated cytokines, 22 had lower postoperative mean values compared to preoperative values (Table 4). A statistically significant decrease was shown for IL-1β, IL-2, IL-12p40, ganulocyte macrophage colony-stimulating factor (GM-CSF), interferon-g induced protein 10 (IP-10), monokine induced by interferon gamma (MIG), eotaxin, and monocyte chemoattractant protein 1 (MCP-1; P < .05). The IL-6 was the only cytokine that showed a significant increase postoperatively (P < .05). Both CRP (P < .028) and CD64 (P < .001) also showed a significant increase postoperatively.
Serum Cytokine Values Measured Pre- and Postoperatively.
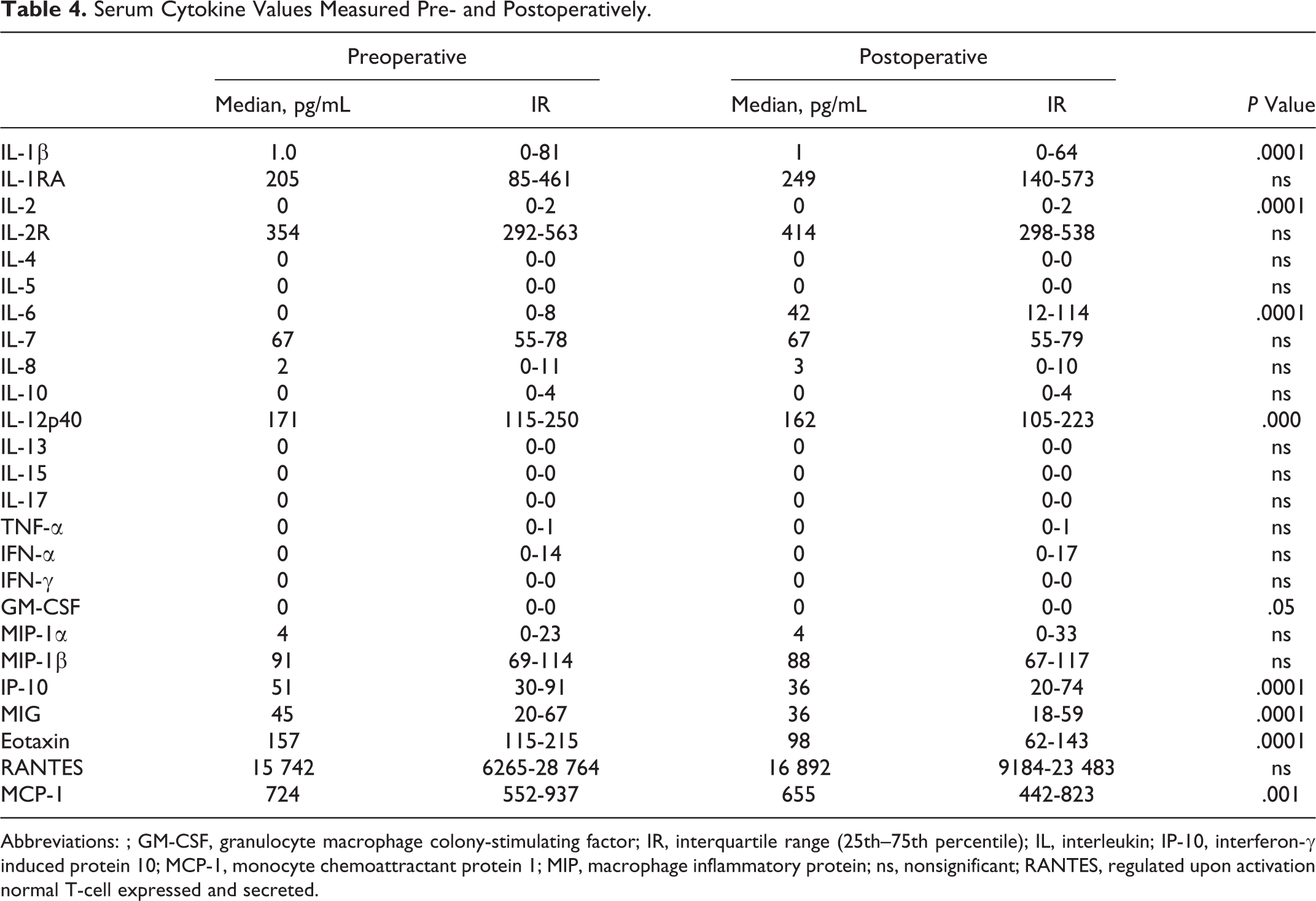
Abbreviations: ; GM-CSF, granulocyte macrophage colony-stimulating factor; IR, interquartile range (25th–75th percentile); IL, interleukin; IP-10, interferon-γ induced protein 10; MCP-1, monocyte chemoattractant protein 1; MIP, macrophage inflammatory protein; ns, nonsignificant; RANTES, regulated upon activation normal T-cell expressed and secreted.
Pre- and Postoperative Cytokine Analyses Based on Infection or Fever Compared to no Infection
Patients With Preoperative Infection
Associations with preoperative infection (Tables 5 and 6) were shown for pre- and postoperative values of IL-2R, IL-4, IL-6, macrophage inflammatory protein (MIP)-1α, in addition to preoperative values of IFN-γ and postoperative values of IP-10 and regulated upon activation of normal T cells expressed and secreted (RANTES; P < .05).
Serum Values of Indicated Cytokines Measured Preoperatively Analyzed Depending on Infection Status.
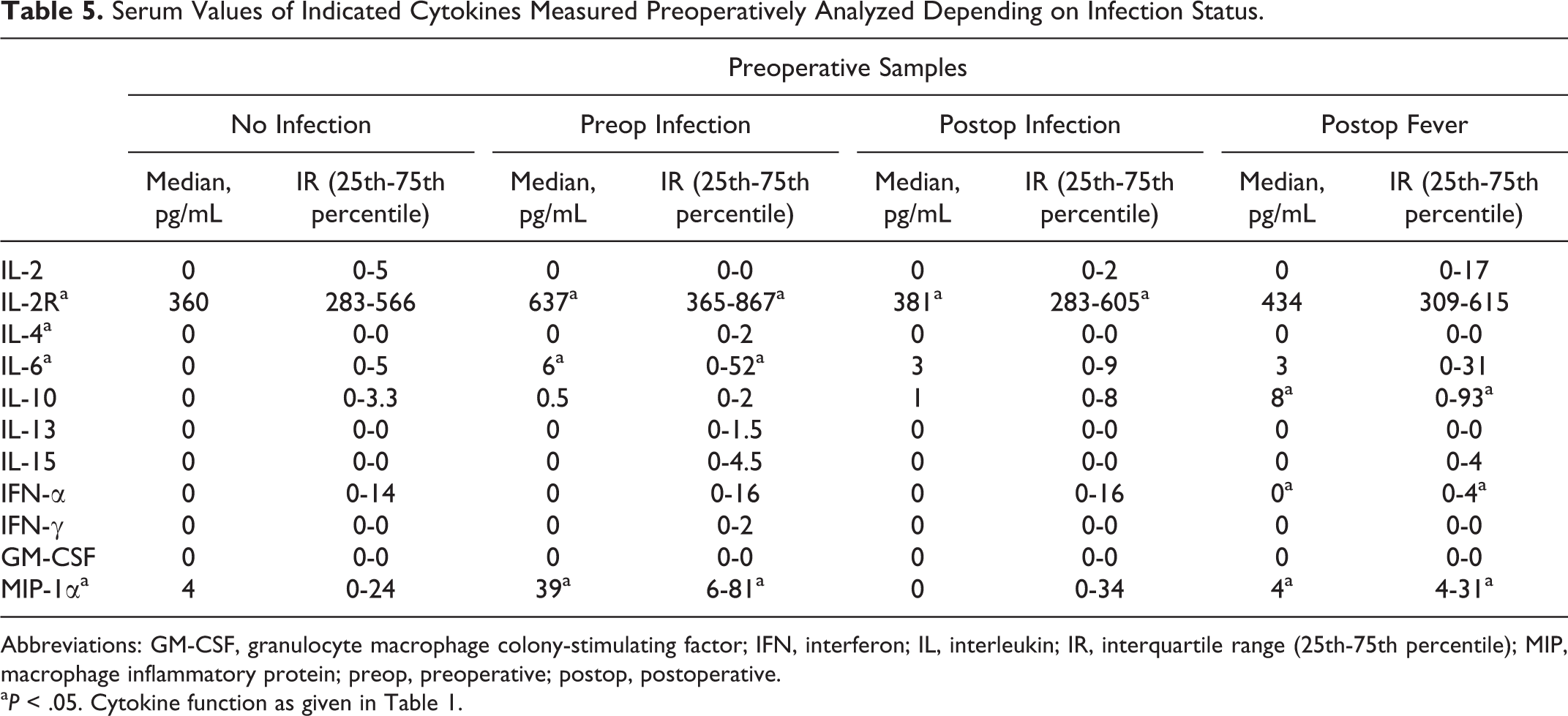
Abbreviations: GM-CSF, granulocyte macrophage colony-stimulating factor; IFN, interferon; IL, interleukin; IR, interquartile range (25th-75th percentile); MIP, macrophage inflammatory protein; preop, preoperative; postop, postoperative.
a P < .05. Cytokine function as given in Table 1.
Serum Values of Indicated Cytokines Measured Postoperatively Analyzed Depending on Infection Status.
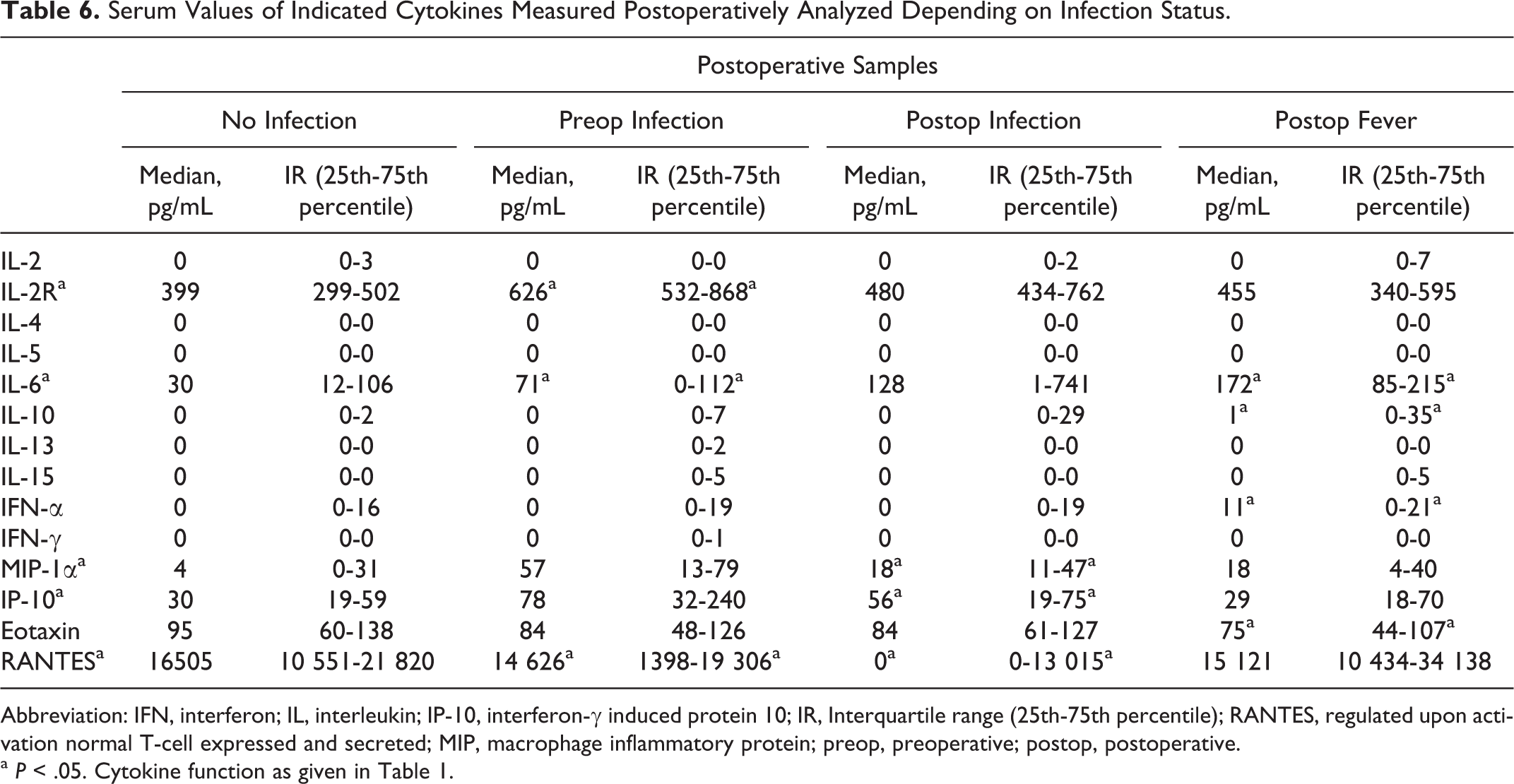
Abbreviation: IFN, interferon; IL, interleukin; IP-10, interferon-γ induced protein 10; IR, Interquartile range (25th-75th percentile); RANTES, regulated upon activation normal T-cell expressed and secreted; MIP, macrophage inflammatory protein; preop, preoperative; postop, postoperative.
a P < .05. Cytokine function as given in Table 1.
Patients With Postoperative Infection
Associations with postoperative infection (Tables 5 and 6) were shown for pre- and postoperative values of IL-2 and IL-13 as well as postoperative values of MIP-1α, IP-10, and RANTES (P < .05).
Patients With Early Postoperative Fever
Associations with EPOF (Tables 5 and 6) were shown for pre- and postoperative values of IL-10 and IFN-α in addition to preoperative values of GM-CSF, MIP-1α, and postoperative values of IL-6 and Eotaxin.
Cytokine, CRP, and CD64 Analyses Based on Postoperative Infection or Fever
Analysis of the postoperative values of CRP (P < .001) and CD64 (P = .028) together with IL-6 (P = .006) and IL-10 (P = .02) using logistical regression showed a statistically significant association with postoperative infection or fever when analyzed individually. Combined analysis with CRP and CD64 together with either IL-6 or IL-10 values showed a statistical significance when using a 1-tailed test.
Discussion
The results have shown a general decrease in cytokine levels following vascular surgery, the exception being IL-6 that showed a statistically significant increase postoperatively. As expected, both CRP and CD64 showed a significant increase in response to surgery. A significant association between both pre- and postoperative cytokine values and postoperative infection has been shown for IL-2 and IL-13. Preoperative infection was associated with values of IL-2R, IL-6, IL-15, and MIP-1α, measured both pre- and postoperatively. Isolated postoperative fever was associated with values of IL-10 and IFN-α measured both pre- and postoperatively. Furthermore, we found associations between postoperative values of several chemokines and cytokines (pro- and anti-inflammatory) with postoperative infection. However, due to the small amount of infections, we had no intention of drawing any conclusions about the predictive value of these cytokines.
The logistical regression analysis showed a significant predictive value for combining either IL-6 or IL-10 with CRP and CD64, in the diagnosis of postoperative infection. This implies a significant supplementary role for IL-6 and IL-10 in the postoperative diagnosis of infection. The association between the preoperative values of IL-10 and postoperative infection in combination with CRP and CD64 points to the potential usefulness of IL-10 as a diagnostic tool for early postoperative infection.
Early postoperative fever (EPOF) described as fever (temperature >38°C) during the first 48 hours after surgery is quite common in vascular surgery. 17 The etiology of the fever can be either infectious as caused by endotoxins or an acute phase response to surgical trauma, both of which are mediated by cytokines. 17 Further complicating the picture is the finding that postoperative infections do not necessarily present with fever 18 as shown in our series where only 2 of the postoperative infections (1 case of pneumonia and 1 case of urinary tract infection) were accompanied by fever. Although blood cultures were taken for all patients with clinical signs of infection, including fever, there were no positive culture results confirming bacteremia. Therefore, the patients with fever but no other clinical signs of infection have been assigned to a separate group.
Due to the paucity of postoperative infections in this material and the relatively small number of surgical procedures in each category, the results do not lend themselves to subgroup analyses based on the type of infection or surgical procedure. Furthermore, we cannot specify the source of the cytokines, as the samples were not differentiated into various cell type origins.
One of the thought-provoking observations in this study was the general decline in the serum concentrations of 22 of the 25 cytokines measured postoperatively. This decrease was statistically significant for 8 of the 22 cytokines. This phenomenon is made more intriguing, when considering the fact that all 8 are implicated in the proinflammatory response, where 4 (IL-1β, IL-2, IL-12p40, and GM-CSF) induce a proinflammatory response through the activation of T cells and mononuclear phagocytes (MNPs), and the remaining 4 (IP-10, MIG, eotaxin, and MCP-1) function as chemoattractants for various immunocompetent cell types. A possible explanation for this may involve the role of anesthetic agents and surgical stress in attenuating the cytokine-induced proinflammatory response. Previous studies have shown impaired neutrophil chemotaxis, MNP phagocytic capacity, and a decline in the number of circulating NK cells postoperatively. 19 The significance of this finding for the development of postoperative infection cannot be ascertained; however, given the substantive role of the involved cytokines in initiating an inflammatory response, it is difficult to disregard their potential contributing effect. The prophylactic use of antibiotics is another possible explanation for the postoperative decrease in the values of the 8 proinflammatory cytokines. Interleukin 10 which was significantly increased postoperatively provides a mechanism for the possible effect of antibiotics through its regulatory and repressive effect on proinflammatory cytokines during the recovery phase of infection. 20
We can only speculate about the exact effects of regional and general anesthetics on our patient cohort. Research into the immunologic effects of specific types of anesthesia, for example, local, regional, and general and anesthetic agents have revealed some of the effects of these agents on serum cytokine levels. 21 –24 Based on the type of procedure, the use of the different modalities of anesthesia was slightly in favor of general anesthesia, that is, 54% general anesthesia comprising carotid endarterectomy (CEA), abdominal aortic aneurysm open repair (AAA-OR), and aortoiliac occlusive disease (AIOD) and 46% spinal/epidural anesthesia comprised endovascular aortic repair (EVAR) and infrainguinal operations. Furthermore, blood transfusions are also considered to be associated with immunosuppression and an increased incidence of postoperative infections. 25,26 Since all patients in our study underwent elective procedures, there were no massive transfusions as might be required during emergency open repair of ruptured AAA. The share of procedures, which often require transfusion, that is, open aortic surgery (27%), is balanced in our study by the proportion of procedures that seldom require blood transfusions, that is, CEA (27%).
Proinflammatory cytokines are vital in modulating the acute inflammatory process. Among the cytokines that showed a statistically significant variation in this study were IL-6, IFN-γ, and MIP-1. Both IL-6 and IFN-γ have potent proinflammatory properties. Interleukin 6 has been found in relatively large quantities in human atherosclerotic plaques 27 and is thought to play an important role in the pathogenesis of coronary artery disease. 12 It has also been shown to correlate positively with prosthetic infection in patients operated with total hip and knee arthroplasty. 28,29 The IFN-γ is mainly produced by activated T cells and NK cells and among its many and varied effects are its interactions with PMNs that are particularly interesting. Interferon-γ plays a key role in the upregulation of CD64 on neutrophils, 15 which enhances the phagocytic ability of these cells. 8
Apart from the proinflammatory cytokines and chemokines that have shown significant variations in this study, there was also a group of anti-inflammatory cytokines represented by IL-10 and IL-13. The role of IL-10 in bacterial disease has not been fully elucidated, but it is thought that through its inhibition of proinflammatory cytokines it provides a protective function against the detrimental effects of systemic inflammation. 14 Interleukin 13 manifests its anti-inflammatory effects through the inhibition of IL-1β, IL-6, IL-8, and TNF-α. 11
Several of the chemokines showed a significant association with postoperative infection. Eotaxin, MIP-1, and MCP-1 are involved in the chemotactic migration and activation of PMN and other cell types, for example, monocytes and lymphocytes to sites of inflammation. 30
Mononuclear phagocytes are a major source of proinflammatory cytokines. 14 Since the majority of the cytokines that showed a significant variation in their serum concentrations in this study are derived from MNPs, it can be inferred that these cells have a prominent role in the host defense against infection. This is in accordance with the essential role of the innate immune system in combating bacterial infections.
In conclusion, we have shown a positive correlation between perioperative infection and both pro- and anti-inflammatory cytokines, in particular IL-10 and IL-13. To our knowledge, this is the first report linking IL-10 plasma levels to perioperative infection. Furthermore, the chemokines included in this study have shown a potential as diagnostic markers for postoperative infection in vascular surgery. Despite its shortcomings as already discussed, the study has generated some interesting results that can provide the basis for further research in this field.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded through research grants from the University of Bergen.