
Abstract
Abdominal paracentesis complicated by perforation of a penetrating arterial branch is an extremely rare complication. We report 2 patients who presented with abdominal wall pseudoaneurysms following abdominal paracentesis for the evaluation and treatment of their hepatic dysfunction. We subsequently review the treatment modalities and interventions performed in each case.
Case Series
Patient 1
A 58-year-old male presented with decompensating end-stage liver disease associated with hyponatremia (113 mEq/L), deteriorating serum creatinine (1.0-2.1 mg/dL), and a model for end-stage liver disease (MELD) score of 37. He had a past medical history of treatment-naive hepatitis C (genotype I, IL-28B CT) complicated by ascites, hepatocellular carcinoma, hepatic encephalopathy, and esophageal varices. He had an abdominal paracentesis and microwave ablation of a caudate lobe lesion performed 4 days and 3 weeks prior to this presentation, respectively. The patient’s mental status had been stable. He described increasing fatigue with associated nausea and vomiting but denied fever, chills, shortness of breath, cough, chest pain, or limb swelling.
On examination, the patient was afebrile but jaundiced and dehydrated with a pulse rate of 63 beats/min, blood pressure of 121/90 mm Hg, and room air oxygen saturations of 99%. Physical examination elicited reduced breath sounds in both lung bases, abdominal ascites, and mild lower limb peripheral edema. The previous paracentesis wound was satisfactory. Hematological analysis revealed a hemoglobin of 11.4 g/dL, white blood cell count 12.4 × 109/L, platelets 102 × 109/L, international normalized ratio (INR) 2.65, and mildly elevated liver function tests (total bilirubin 28 mg/dL, alkaline phosphatase 165 U/L, alanine transaminase 86 U/L, and aspartate transaminase 175 U/L). Following hospital admission and evaluation, ultrasound-guided paracentesis was performed using 1% lidocaine under aseptic conditions followed by the placement of an 18-gauge YUEH Centesis Catheter (Cook Medical, Bloomington, Indiana) into the largest fluid collection in the right lower quadrant of the abdomen. Approximately 2700 mL of amber fluid was removed.
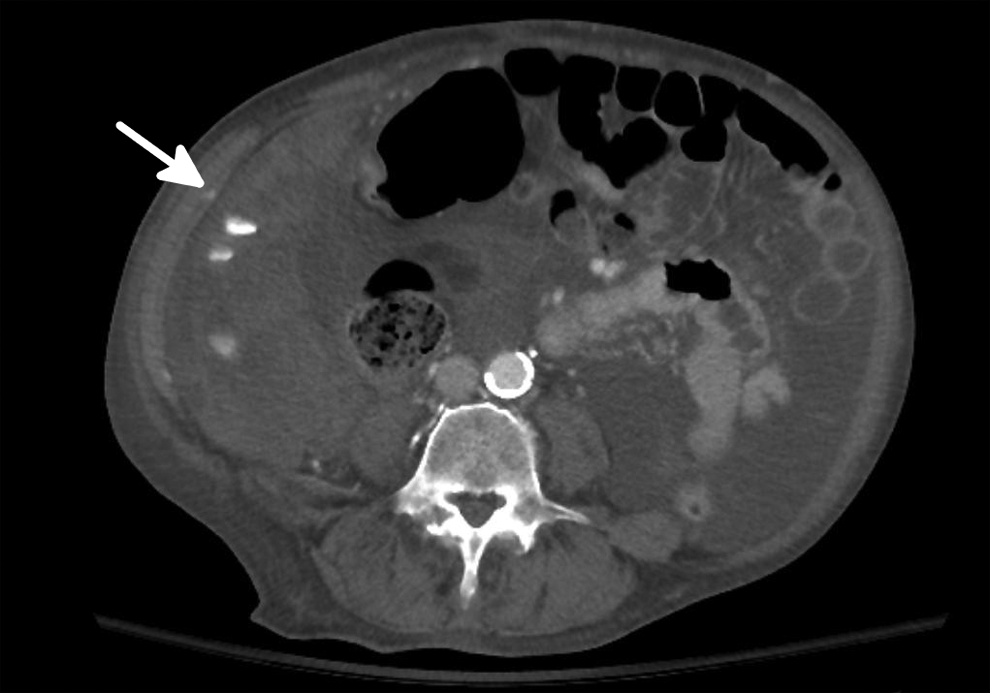
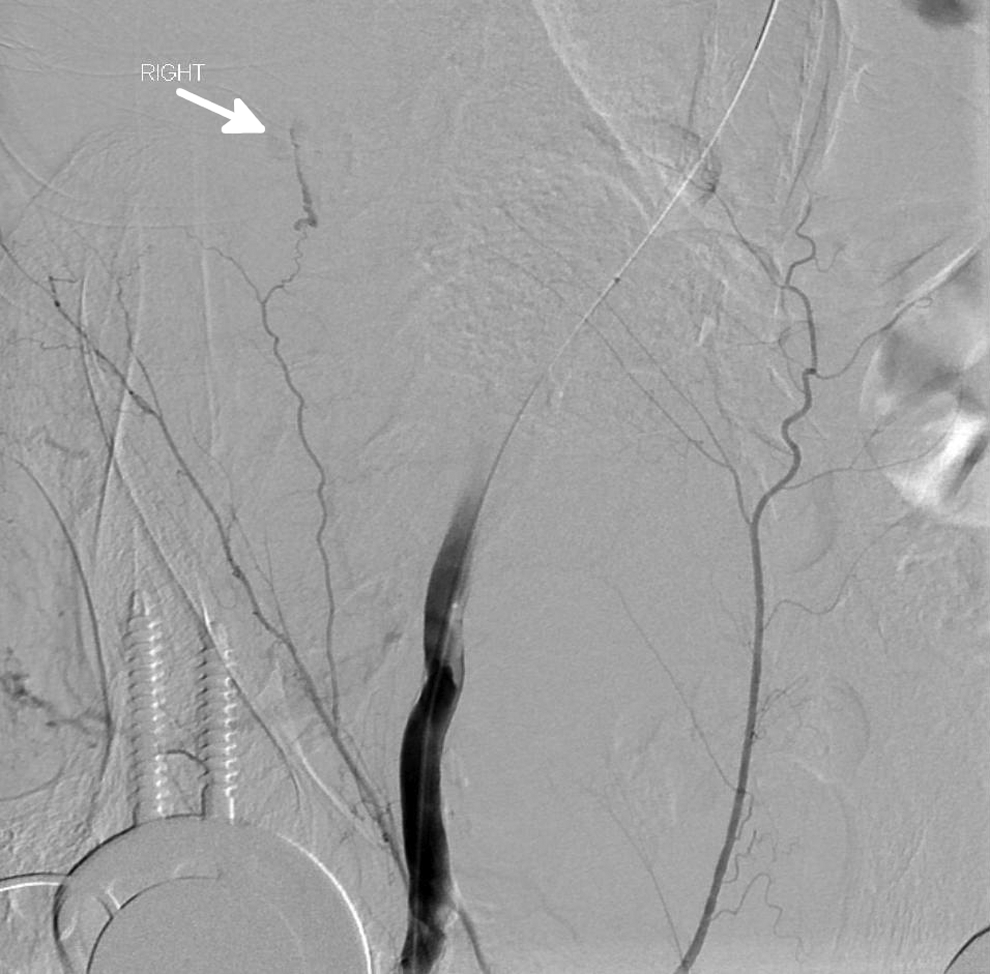
On the following day, the patient acutely deteriorated complaining of severe upper abdominal pain. On examination, he had a wide complex tachycardia (120/min) and a blood pressure of 85/50 mm Hg. His hemoglobin dropped to 7.4 g/dL. Despite receiving 4 units of packed red cells (pRBCs), he remained hemodynamically unstable with further decline in hemoglobin to 7.2 g/dL. He required additional blood transfusion products (4 pRBCs and 2 fresh frozen plasma [FFP]) and was commenced on inotropic support with dopamine at 15 µg/kg/h. An emergency computed tomography (CT) angiogram of the abdomen and pelvis confirmed active hemorrhage adjacent to the perihepatic region of the right upper quadrant (Figure 1). A transfemoral arteriogram revealed a 6.0 × 8.0 mm pseudoaneurysm along the right lateral abdominal wall originating from the deep circumflex iliac artery (Figure 2). Unfortunately, the common femoral arterial (CFA) puncture site and subsequent 5F sheath were positioned too proximal to facilitate access to the deep circumflex iliac artery. Therefore, percutaneous thrombin injection (3000 U) was administered into the pseudoaneurysm using a 25-gauge needle with successful thrombosis.
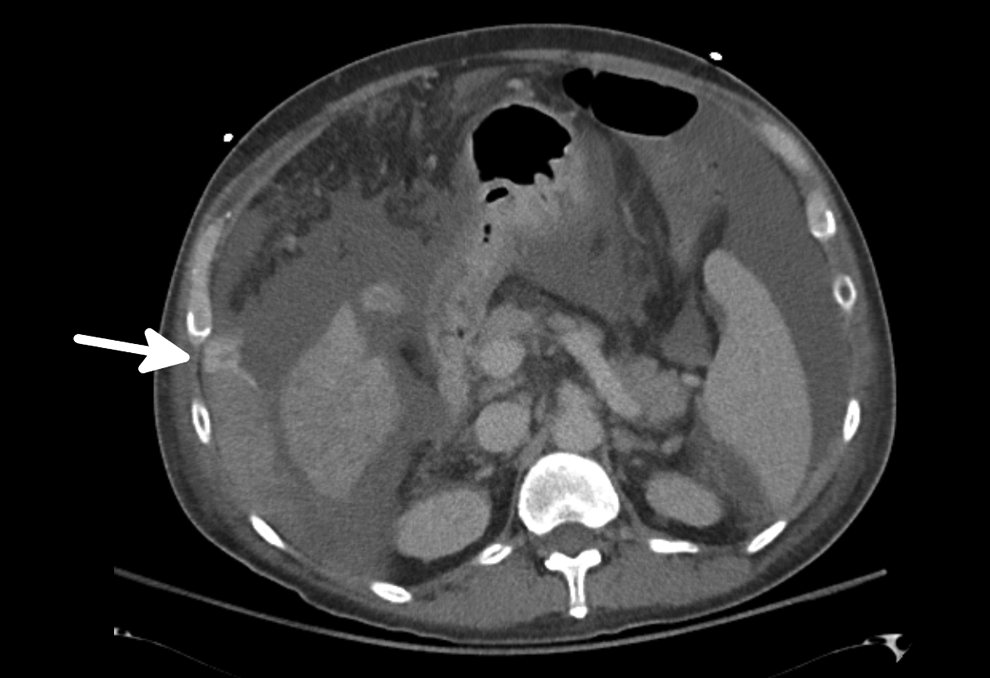
Delayed venous phase computed tomography (CT) angiogram of abdomen and pelvis, demonstrating a serpiginous stream of high-density material spanning between the right upper quadrant perihepatic/hepatic region and the right lower quadrant superficial tissues consistent with active hemorrhage (white arrow).
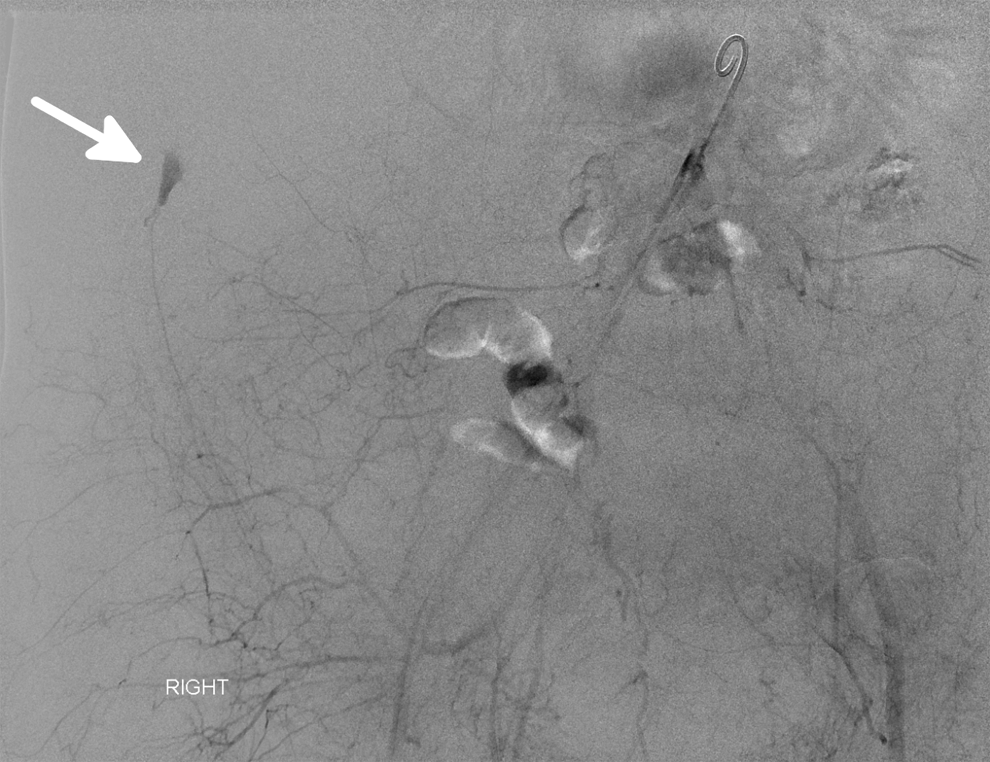
Transfemoral arteriogram demonstrating 6 × 8 mm pseudoaneurysm along the right lateral abdominal wall supplied by the deep circumflex iliac artery (white arrow).
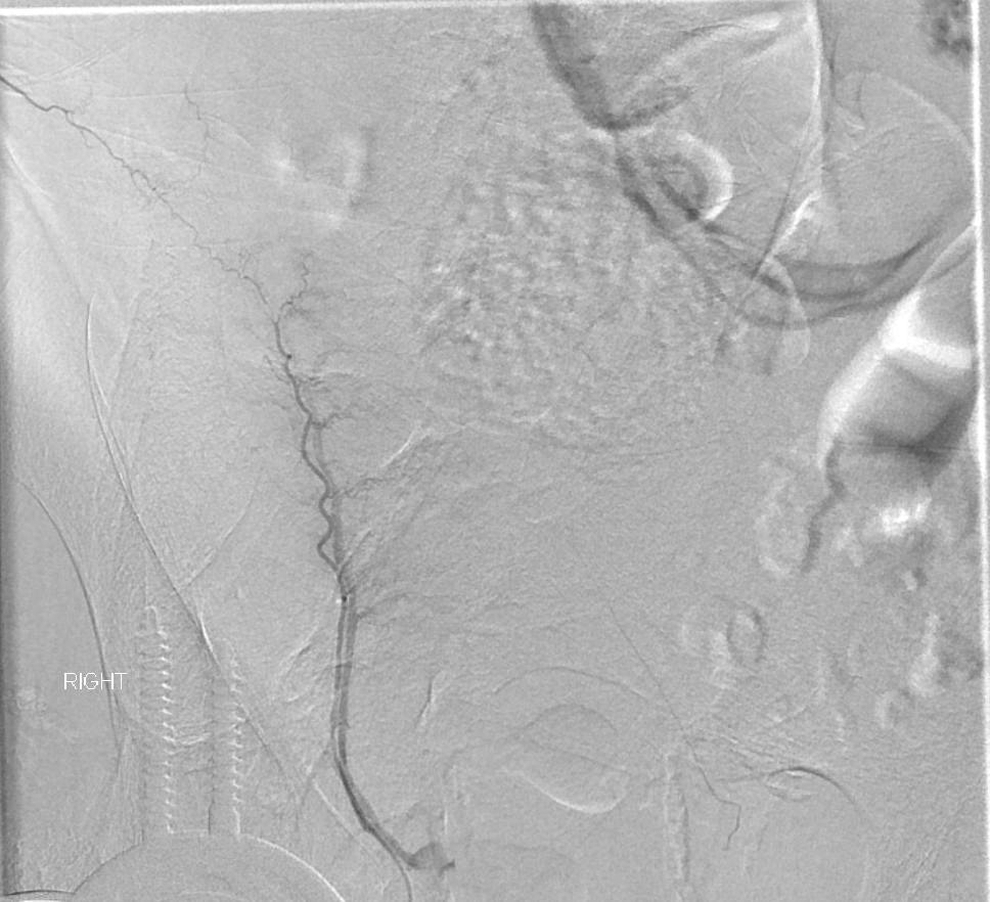
Unfortunately, the patient deteriorated the following day with recurrence of hemodynamic instability and requirement for additional blood products. A repeat transfemoral arteriogram, using a lower CFA puncture under ultrasound guidance, demonstrated partial thrombosis of the right deep circumflex iliac artery pseudoaneurysm (Figure 3). A microcatheter was advanced into the deep circumflex iliac artery. Polyvinyl alcohol (PVA) foam embolization particles (200 μm; Cook Medical, Bloomington, Indiana) were injected followed by deployment of 3 coils (VortX 18 Vascular Occlusion Coil, Boston Scientific, Quincy, Massachusetts). Postembolization angiogram demonstrated satisfactory occlusion of the pseudoaneurysm (Figure 4).
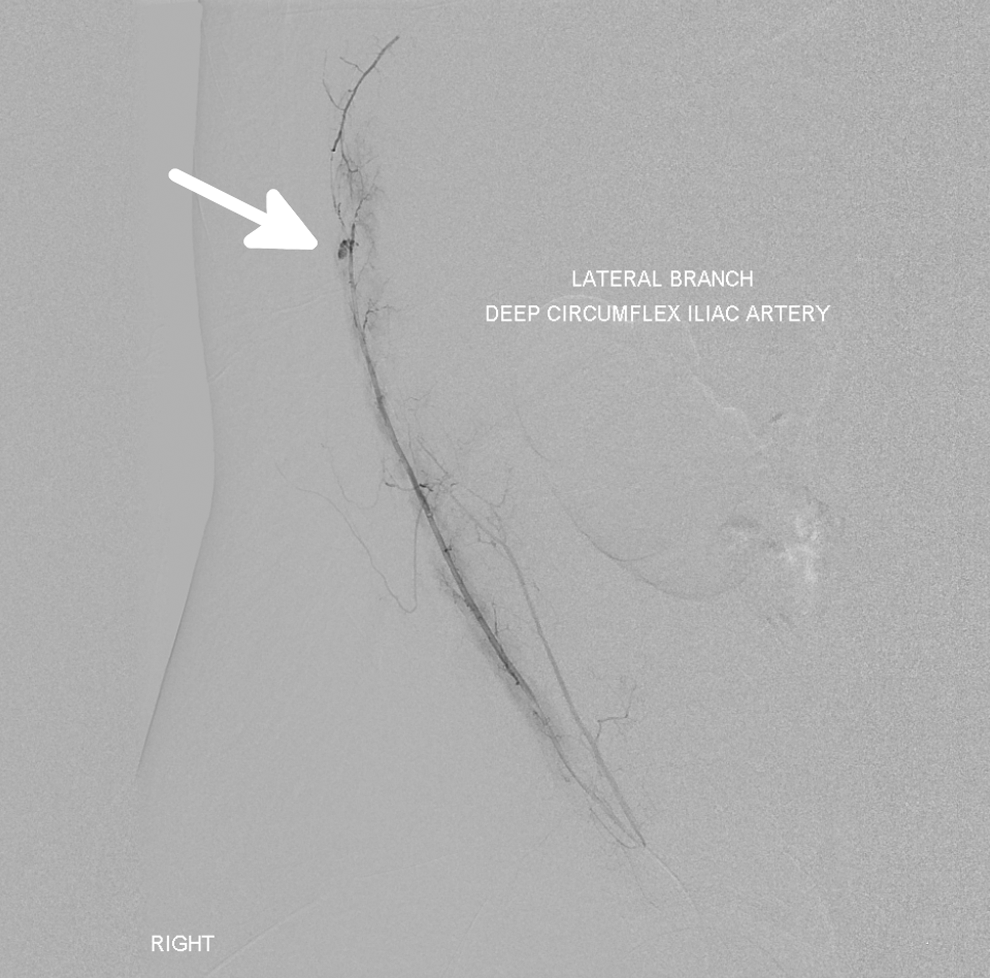
Transfemoral arteriogram confirming partial thrombosis of the right deep circumflex artery pseudoaneurysm (white arrow).
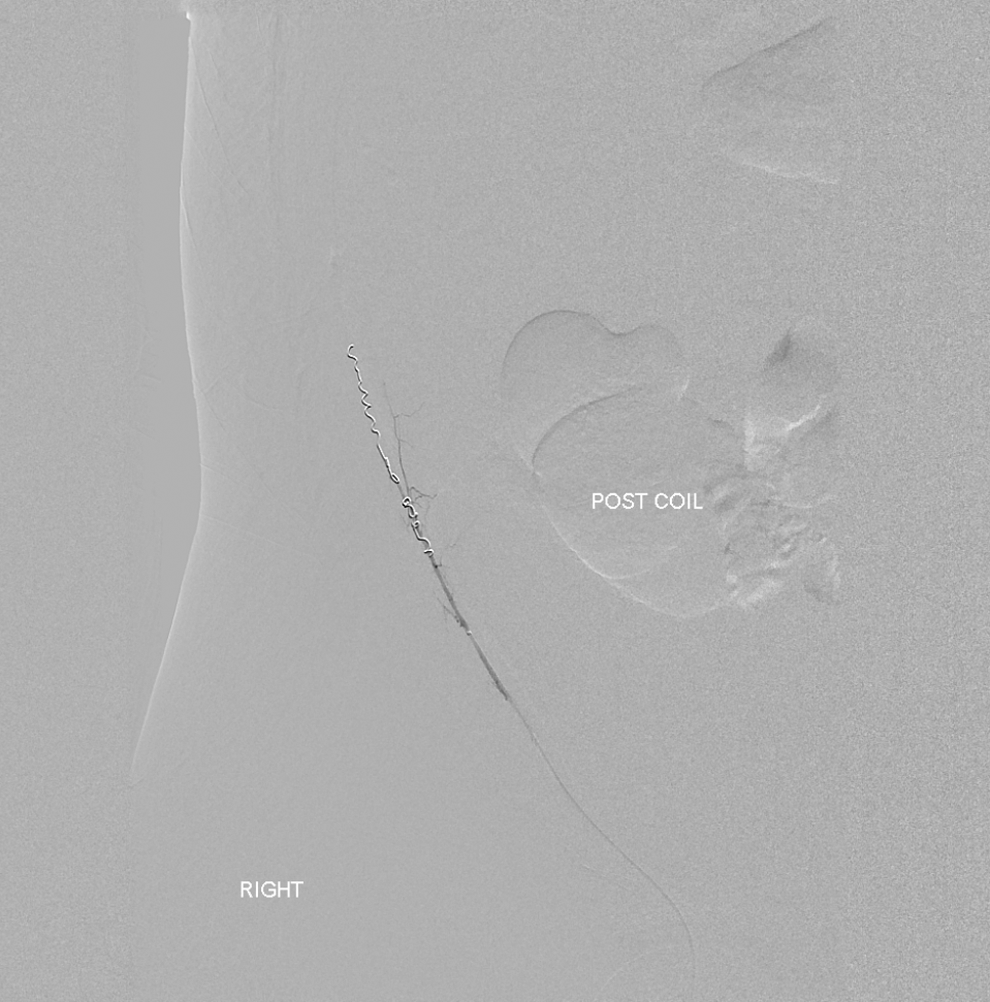
Transfemoral arteriogram confirming successful particulate and coil embolization of the right deep circumflex iliac artery.
The patient remained hemodynamically stable following the procedure and was actively listed for a liver transplant. Unfortunately, 2 days later, he developed significant gastrointestinal bleeding from esophageal varices. Despite mobilization of the massive blood transfusion protocol and emergency endoscopic treatment, his bleeding continued. He progressively deteriorated, and following discussion with the patient’s family, further treatment was withdrawn and the patient died.
Patient 2
A 68-year-old male presented for evaluation of liver metastases. The patient had previously opted only for serial imaging for a right renal mass that had increased in size from 3.8 to 4.2 cm over the last year. He had undergone a paracentesis 14 days prior to admission, which had yielded 40 mL of dark yellow-colored fluid that had rare atypical cells consistent with inflammatory reaction. He had a past medical history of type 2 diabetes mellitus, dialysis-dependent end-stage renal disease secondary to diabetic nephropathy, ischemic cardiomyopathy with an ejection fraction of 40%, and peripheral arterial disease with a previous right below-knee amputation. He was prescribed warfarin for atrial fibrillation. On examination, the patient’s vital signs were all within normal limits. There were decreased breath sounds in both lung bases, abdominal distension, and bilateral lower extremity pitting edema. His previous paracentesis wound was satisfactory. Hematologic analysis revealed a hemoglobin of 11.0 g/dL, white cell count 7.7 × 109/L, platelets 204 × 109/L, INR 1.47 and liver function tests that were within normal limits except for a mildly elevated alkaline phosphatase (128 U/L).
Prior to a percutaneous liver biopsy, ultrasound-guided paracentesis was performed, yielding 700 mL of amber fluid. No immediate procedural complications were evident. The following morning, the patient became hypotensive with a systolic blood pressure of 80 mm Hg and his hemoglobin was 8.5 g/dL, which further decreased to 6.9 g/dL. He received 2 units of pRBC and 1 unit of FFP. An emergency CT angiogram of the abdomen and pelvis confirmed active hemorrhage from the right anterolateral abdominal wall into the abdominal cavity, most likely arising from the deep circumflex iliac artery (Figure 5). A transfemoral angiogram identified active extravasation from the right deep circumflex iliac artery (Figure 6). A microcatheter was advanced into the superficial iliac circumflex artery. The PVA foam embolization particles (200 μm; Cook Medical) were injected followed by deployment of 2 coils (VortX 18, Vascular Occlusion Coil; Boston Scientific). Check angiography confirmed cessation of bleeding (Figure 7).
Delayed venous phase computed tomography (CT) angiogram of abdomen and pelvis, demonstrating active hemorrhage from the anterior right lateral abdominal wall into the abdominal cavity arising from the superficial iliac artery (white arrow).
Transfemoral arteriogram demonstrating active hemorrhage along the right lateral abdominal wall supplied by the deep circumflex iliac artery (white arrow).
Transfemoral arteriogram confirming successful coil embolization of the right deep circumflex iliac artery.
A further 1 pRBC unit was transfused and the patient remained hemodynamically stable. Four days later, the previously planned ultrasound-guided liver biopsy was performed without complication. Although the liver biopsy was nondiagnostic, subsequent biopsy of the renal mass revealed a renal carcinoma with papillary and clear cell features for which the patient is currently being treated.
Discussion
Severe hemorrhage requiring blood transfusion after abdominal paracentesis is a very rare (<1%) but potentially lethal complication, with reported death rates of 0.016% to 0.039% in patients with liver dysfunction. 1 Although the risk of bleeding may not be related to operator experience, increased bleeding rates have been reported in patients with renal failure, low platelets, elevated prothrombin/INR levels, and high MELD scores, which were all identified in our patients. 1
Management of arterial bleeding in patients with end-stage liver disease can be especially difficult due to the patient’s compromised clotting function and the nature of the injury sustained. An injured circumflex iliac artery also presents a diagnostic challenge with minimal clinical findings compared to other abdominal wall arterial injuries such as the inferior epigastric artery that often presents with symptomatic palpable hematomas. 2 -4 As noted on both CT scans, patients can bleed directly in the peritoneum without a large pseudoaneurysm or hematoma. In such cases, percutaneous thrombin injection is less valid than the conventional endovascular embolization due to the absence of a clearly identifiable pseudoaneurysm. A high level of clinical suspicion is therefore warranted in such patients following a lateral abdominal wall puncture after paracentesis. 1 The overall clinical context of the patient often influences the modality utilized for the diagnosis of hemorrhage after paracentesis where ultrasound, repeat paracentesis, contrast-enhanced CT imaging, or endovascular visualization under fluoroscopic guidance have been used. Close peri- and postprocedural monitoring is warranted in these high-risk patients.
Embolization of the culprit artery can be used for definitive management of acute bleeding. 5 Loffroy et al reported a superselective coil embolization packing technique, with preservation of the parent artery for peripheral pseudoaneurysms affecting the splenic, carotid, hepatic, superior mesenteric, cystic, uterine, and hypogastric arteries. 6 These authors demonstrated a technical success rate of 100%, complete pseudoaneurysm exclusion with a single procedure in 93.8% (15 of 16) patients, and no major complications or late recanalization during a mean follow-up of 24.7 months.
In patients where direct embolization is not possible, percutaneous thrombin injection has been previously shown to be an efficacious method of treating iatrogenic pseudoaneurysms, with less than 2% of patients having downstream occlusion of the artery being treated. 7 -9 Although there is a theoretical risk of allergic reaction to thrombin, this has not yet been reported in the literature. Percutaneous collagen injection has also been shown to be very successful in the management of femoral artery pseudoaneurysms, with reported success rates of 97.3%. 10 Although the majority of published literature regarding percutaneous thrombin injection relates to iatrogenic femoral artery pseudoaneurysms, the authors believe this to have been a valid approach in a patient with hemodynamically unstable coagulopathy where the initial femoral arterial access point was deemed too high, precluding endovascular treatment with the initial arteriogram. The authors acknowledge that other endovascular modalities may have been considered at this stage such as sheath withdrawal, use of a reverse angled catheter, or even contralateral access. Technically, when treating circumflex iliac or inferior epigastric arterial bleeds, a lower common femoral arterial puncture site assists the cannulation of these smaller proximal arterial branches. Ultrasound guidance can be used to help facilitate puncture. Despite successful occlusion of pseudoaneurysm in patient 1 during the first procedure, recurrence of hemodynamic instability necessitated a second endovascular intervention where a lower CFA puncture was utilized. The authors postulate that an early surveillance strategy using ultrasound of thrombin-treated pseudoaneurysms in high-risk patients with coagulopathy may identify potential treatment failures.
Conclusion
Severe hemorrhage after abdominal paracentesis is a rare but recognized complication that can occasionally be fatal in patients with severe liver disease and coagulopathy. Prompt recognition, resuscitation, use of adjuvant hemostatic products combined with active interventional modalities using percutaneous thrombin injection, endovascular embolization, or a combination of both are vital. Given its high success rate, endovascular embolization should be considered the gold standard when available. Unfortunately, despite successful hemostasis, patients often succumb to complications relating to their primary liver disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.