
Abstract
Purpose:
To evaluate the influence of endovascular therapy of ruptured abdominal or iliac aneurysms on total mortality.
Materials and Methods:
We analyzed the mortality of 40 patients from 2005 to 2009, when only surgical treatment was available. These results were compared with the period 2010 to 2013, when endovascular aneurysm repair (EVAR) was assessed as the first option in selected patients.
Results:
During 2005 to 2009, the mortality was 37.5%. From 2010 to 2013, 45 patients were treated with mortality 28.9%. Open repair was performed in 35 (77.8%) patients and EVAR in 10 (22.2%) patients. The 30-day and 1-year mortality rates of the EVAR group were 0% and 20%, respectively, and the total mortality rate was 30% during follow-up (median 11 months, range 1-42 months). The 30-day mortality in the surgical group remained unchanged, at 37.1%, and 1-year and total mortality rates were 45.7% and 51.4%, respectively.
Conclusion:
Following integration in the treatment algorithm, EVAR decreased total mortality in our center by 8.6%.
Introduction
Rupture is a life-threatening complication of degenerative abdominal and iliac aneurysms. The standard treatment of a ruptured abdominal aortic aneurysm (rAAA) is surgical resection and replacement with an aortic prosthesis. This approach was initially performed in 1951; however, the mortality rate for this treatment has remained high (41%) during the last 20 years. 1 Endovascular aneurysm repair (EVAR) was introduced into clinical practice in the 1990s with the aim of decreasing the invasiveness and mortality associated with the surgical treatment of unruptured abdominal aneurysms. The principle of this technique is to eliminate the aneurysm via an endoluminal prosthesis (stent-graft), which is inserted transarterially from the femoral artery. Neither a laparotomy nor an interruption of the blood flow in the aorta via a clamp is necessary for this treatment, and therefore, significant hemodynamic changes, which are the main cause of mortality in open repair treatment, do not occur. The efficiency of EVAR as an elective treatment for AAAs was demonstrated in the EVAR I and Dutch Randomized Endovascular Aneurysm Management (DREAM) trials, which included the short-term and medium-term monitoring of patients. The 30-day mortality rate decreases to 1.7% when EVAR is used to treat unruptured aneurysms compared with a rate of 4.7% when they are treated surgically. 2 This difference is further increased in at-risk patients (American Society of Anesthesiologists-ASA III and IV) in whom the mortality rate of this elective surgical treatment increases to 19%. 3
Based on the positive results of its use as an elective therapy, EVAR was used for the treatment of ruptured aneurysms at selected centers, and the first experience was published in 1994. 4 Despite the increasing tendency to use EVAR in rAAA, this approach is not universally accepted by the vascular surgical society.
Less than half of patients with AAAs are suitable for EVAR according to the current instructions for use; therefore, surgical treatment remains the decisive approach. 5 In addition, specific EVAR complications (access vessel injury, type I, and type III endoleaks) or failure requires surgical resolution.
Our middle-volume vascular center annually performs 25 elective open-surgery repairs of AAAs and 15 elective EVARs. For elective EVAR, we use a commercially available stent-graft system that requires a well-defined neck and other morphological criteria.
From 1995 to 2011, we successfully used EVAR as an elective treatment in 158 patients with abdominal aneurysms and 25 patients with iliac aneurysms. The 30-day mortality rate of this cohort was 0.6%. 6 –8 Based on this positive experience, we began using EVAR to treat ruptured abdominal and iliac aneurysms. The objective of this study was to evaluate the feasibility and results of the emergent endovascular treatment of ruptured abdominal or iliac aneurysms at our center when only standard commercially available stent-graft and devices were used. We retrospectively compared overall mortality between 2 periods: (1) when only surgical treatment was available and (2) when an intention-to-treat EVAR protocol was applied.
Materials and Methods
Open Surgical Repair
Our middle-volume vascular center performs an average of 25 elective and 9 emergency repairs of AAAs annually. We retrospectively analyzed mortality among 40 patients with ruptured aneurysm during 2005 to 2009, when only surgical treatment was available. These results were compared with the period 2010 to 2013, when EVAR was assessed as a first option according to our intention-to-treat protocol. Both groups of patients were similar, due to age (median of age 74 years) and comorbidities. Indication for invasive treatment in both groups was the same, signs of ruptured aneurysms according computed tomography (CT) or ultrasound.
From February 2010 to September 2013, open repair was performed in 35 (77.8%) patients, and EVAR was performed in 10 (22.2%) patients. Patients who were not operated on, did not undergo EVAR, or received palliative therapy were excluded from our study.
Endovascular Treatment
Since February 2010, we have used the endovascular strategy as the first approach to treat ruptured abdominal or iliac aneu-rysms. We established a simple intention-to-treat EVAR protocol that meets the requirements of our center (Figure 1). Endovascular treatment of ruptured aneurysms was performed with the approval of the local ethics committee. The EVAR was applied in a selected group of patients with suitable anatomy for a standard commercially available stent-graft system. Aneurysm morphology was evaluated and determined according to preoperative CT angiography (CTA), which consisted of 3-mm slices (Somatom Definition AS+, Siemens, Forchheim, Germany). The presence of a hematoma in the retroperitoneum around the aneurysm was considered a rupture. The EVAR criteria for this study in accordance with the recommendations for the Endurant stent-graft system (Medtronic Vascular, Santa Rosa, California), are as described subsequently. 9
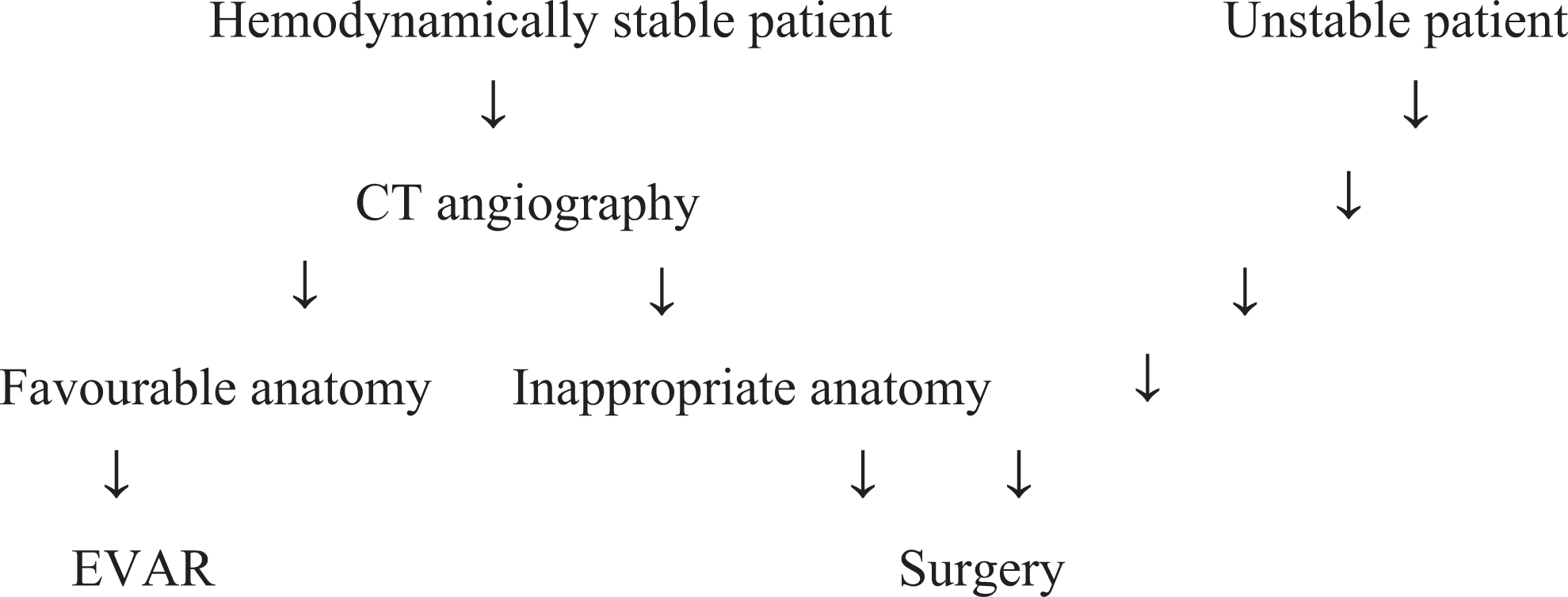
Our intention-to-treat EVAR protocol (since February 2010). EVAR indicates endovascular aneurysm repair.
Criteria for EVAR According to CT
Suitable proximal neck for stent-graft attachment (length ≥ 10 mm, width 19-32 mm, and infrarenal angulation ≤ 75°).
Suitable distal neck for stent-graft attachment in the aorta or iliac arteries (length ≥ 15 mm).
Accessible iliac arteries (width ≥ 7 mm). When CT showed unsuitable anatomy or in unstable clinical situation for CT scanning, surgical treatment was considered just according ultrasound.
Cohort of EVAR Patients
In total, we treated 10 patients (1 woman, 9 men, mean age 75.2 years) endovascularly. There were 7 cases of ruptured AAAs and 3 cases of ruptured internal iliac artery (IIA) aneurysm. At the time of treatment, 2 patients were moderately hemodynamically unstable with a systolic pressure below 80 mm Hg, which necessitated the administration of catecholamine. The remaining 8 patients had stable hemodynamic status.
Endovascular Procedure
The actual intervention was performed under fluoroscopic guidance in a standard angiography suite (Allura Xper FD20, Philips, the Netherlands). In total, we used a bifurcated abdominal stent graft in 6 patients and a tubular stent graft (Endurant, Medtronic Vascular) in 3 patients (Figure 2 and 5). One patient with a ruptured IIA aneurysm was treated only with embolization using an Amplatz vascular plug II (AGA Medical Golden Valley, Minnesota) and acrylate glue (Histoacryl, B. Braun, Melsungen, Germany; Figure 3). In 7 patients, we percutaneously implanted the stent-graft under local anesthesia using the preclose technique. 10 Before stent-graft implantation, 2 devices were inserted at the site of the femoral puncture using the ProGlide 6F system (Abbott Laboratories, Redwood City, California). Hemostasis was achieved by tightening the knots of the closure devices at the end of the procedure. In 2 patients, the stent-graft were implanted under general anesthesia via an arteriotomy of the femoral artery. The endovascular intervention was performed without the administration of heparin and with broad-spectrum antibiotic prophylaxis. After the intervention, the patients were monitored at an intensive care unit and their intra-abdominal pressure was monitored using a urethral catheter. The antibiotics were administered for 7 days following the procedure. The endovascular procedures were performed by 2 physicians (interventional radiologists) who have performed more than 50 elective EVARs.
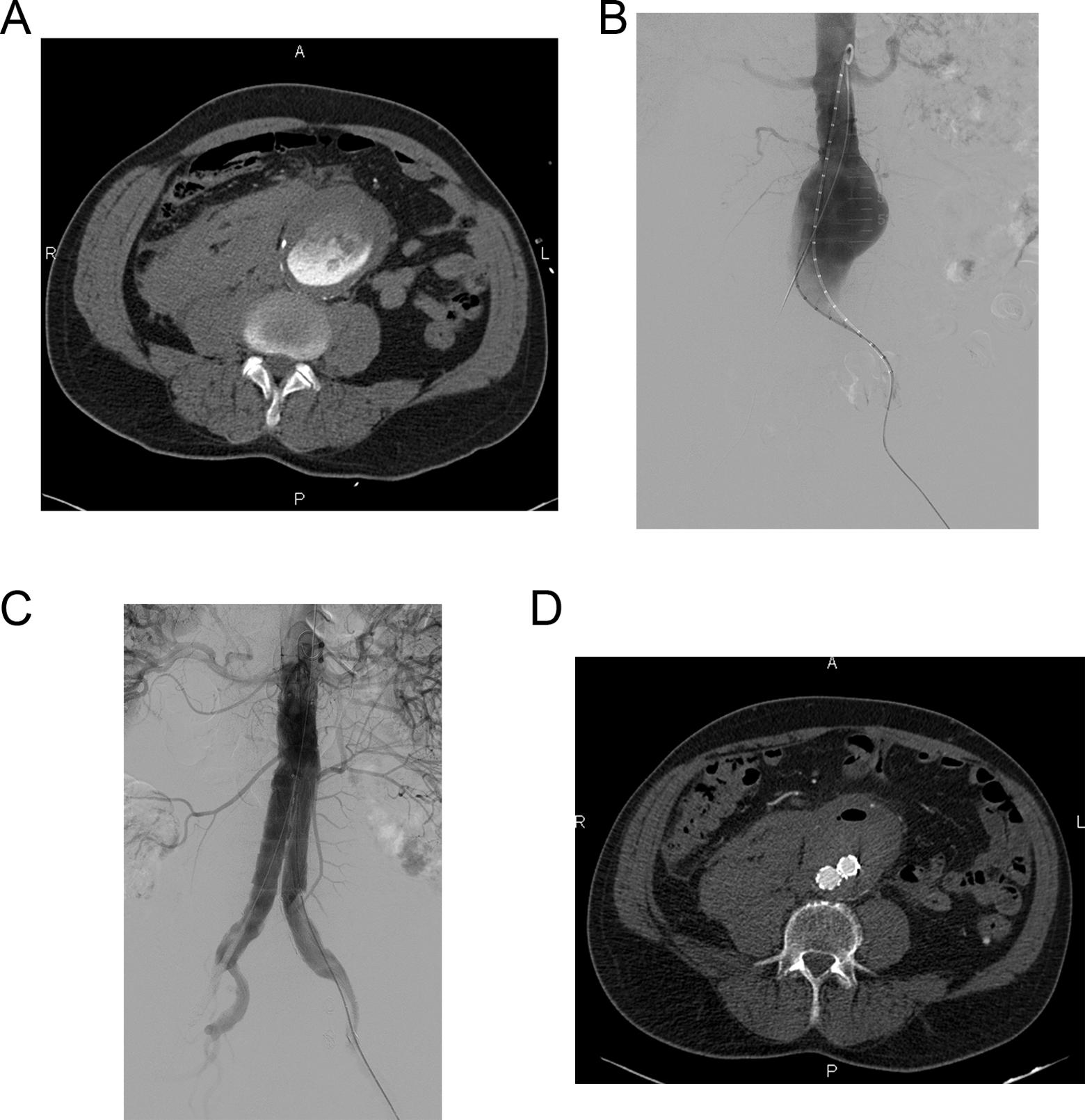
A 64-year-old man with abdominal pain that lasted 4 hours. At the time of hospital admission, he was hemodynamically stable. CTA revealed a ruptured AAA and a large right retroperitoneal hematoma (A). A bifurcated stent-graft was implanted with left iliac extension and embolization of the left IIA (B and C). Follow-up CT 5 days after the procedure confirmed the complete exclusion and thrombosis of the AAA sac and regression of the retroperitoneal hematoma (D). CTA indicates computed tomographic angiography; AAA, abdominal aortic aneurysm; CT, computed tomography.
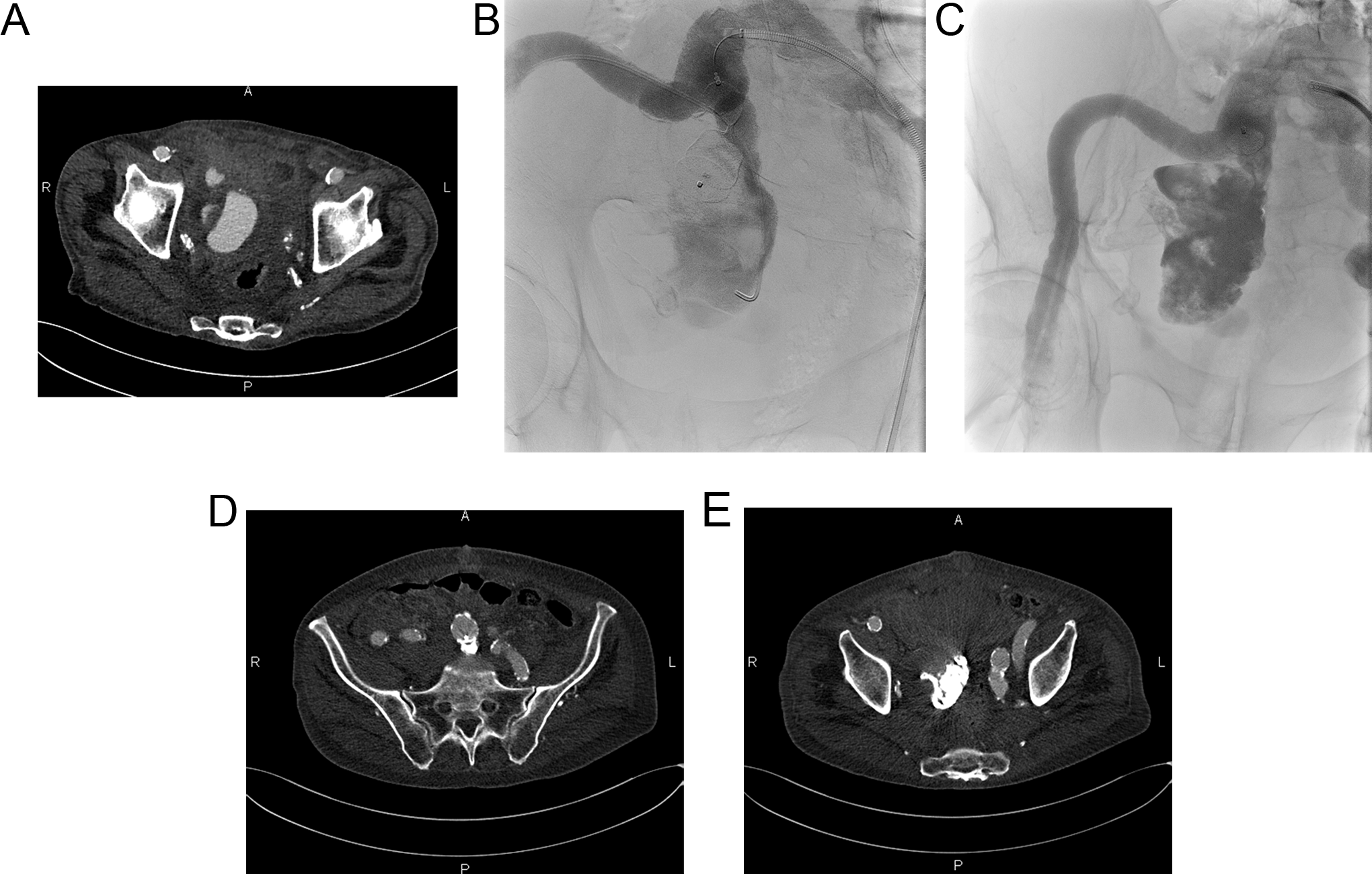
An 89-year-old man with severe abdominal pain that lasted 30 minutes. At the time of hospital admission, he was hypotensive (BP 80/40 mm Hg). CT revealed a 60-mm aneurysm of the IIA with signs of blood extravasation and a large pelvic hematoma (A). The simultaneous femoral access embolization of the aneurysm sac was performed using a vascular occluder, AVP II, and acrylic glue. Parallel positioning of the 4F catheter and occluder was used to reduce the risk of glue migration when the sac was filled (B). The occluder was detached after removal of the catheter when complete acrylic glue embolization was achieved (C). Follow-up CT 7 days after the procedure confirmed that the occluder and the acrylate glue were in a good position (D and E). BP indicates blood pressure; CT, computed tomography; AVP, Amplatz vascular plug.
Follow-up After EVAR
We performed a follow-up CT on the seventh day and at the third and 12th months following treatment. Annual follow-up CT was performed thereafter. In addition, the patients were examined at an outpatient vascular surgery practice.
Results
Open Surgical Repair of rAAAs and Iliac Aneurysms
During 2005 to 2009, 40 patients (9 women, 31 men, median age 74 years, range 57-89) were treated with open repair due to ruptured abdominal or iliac aneurysms. The 30-day mortality rate of this surgical cohort was 37.5%.
During 2010 to 2013, a total of 45 patients with ruptured abdominal or iliac aneurysms were treated in our center. Open repair was performed in 35 patients (6 women, 29 men, median age 74 years, range 48-89) with a 30-day mortality rate of 37.1%. One-year and total mortality in the surgical group in this period was 45.7% and 51.4%, respectively.
Ten patients (1 woman, 9 men, median age 77 years, range 58-89) underwent EVAR for ruptured aneurysm. The overall 30-day mortality rate in the period of the EVAR intention-to-treat protocol was 28.9%. This represents a 8.6% mortality reduction after EVAR implementation.
Endovascular Therapy of rAAAs and Iliac Aneurysms
The mean time from admission to our center until the completion of the endovascular treatment was 73 minutes (range 45-180 minutes). The mean fluoroscopy time was 22 minutes (range 10-35 minutes). The mean aortic diameter of treated ruptured AAAs was 76 mm, whereas it was 55 mm for iliac aneurysms. Two patients developed abdominal compartment syndrome after treatment, which required surgical intervention. In one case, the surgical evacuation of a hematoma from the AAA and the retroperitoneum was performed while the stent-graft was left in position (Figure 4). Drainage of a retroperitoneal hematoma in a ruptured IIA aneurysm was sufficient. In this cohort, the 30-day mortality rate was 0%, the 1-year mortality rate was 20% (2 of 10), and the total mortality rate was 30% (3 of 10). Table 1 shows the detailed characteristics of this cohort. During the follow-up period, there were no complications or deaths due to the intervention or the primary disease (mean follow-up period 11 months, range 1-42 months).
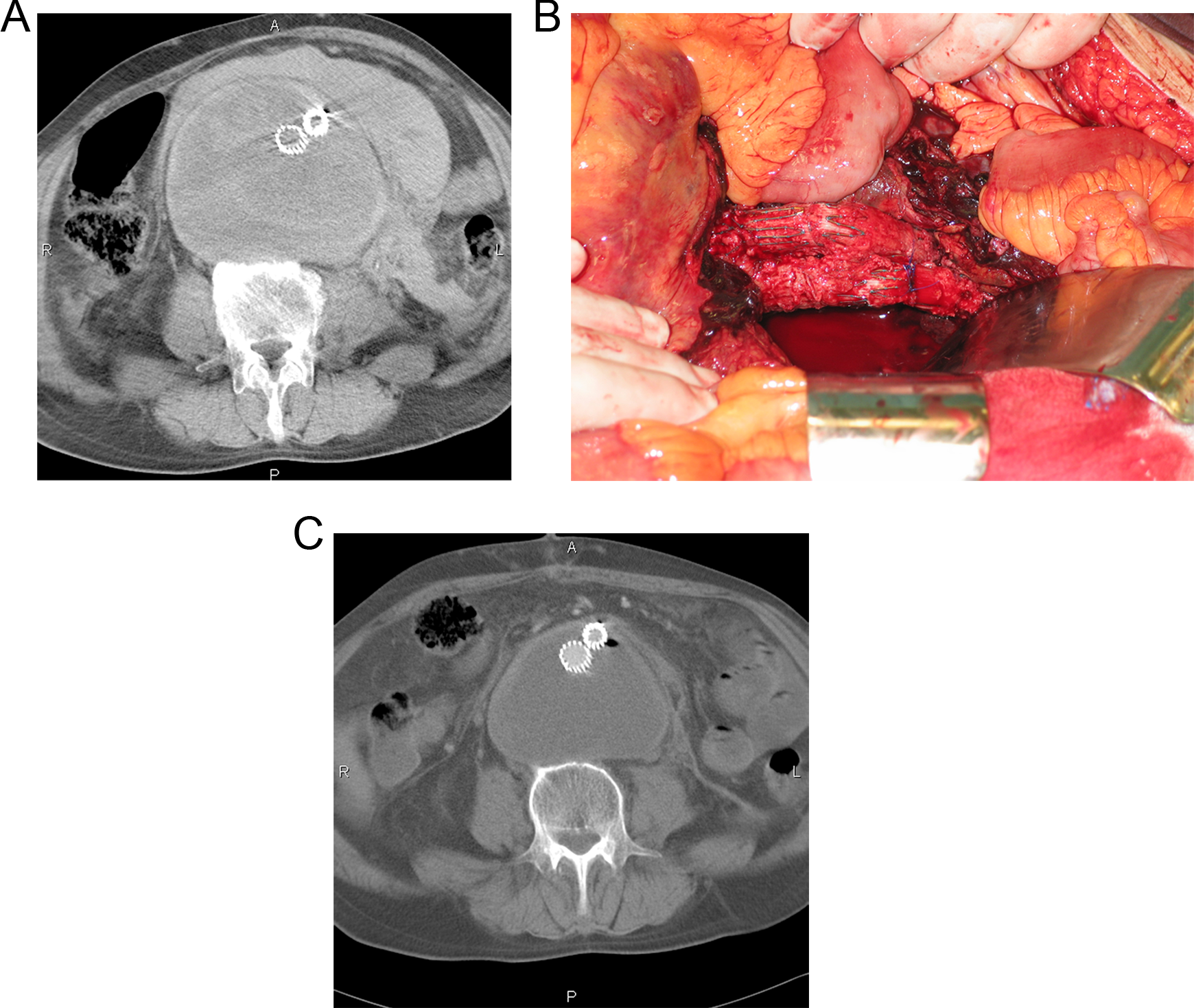
A 58-year-old man who developed abdominal compartment syndrome after EVAR due to an rAAA. An initial CT image shows acute thrombus in the sac of the AAA and the surrounding hematoma (A). Open decompression of the sac was performed with evacuation of the hematoma from the abdominal aneurysm and the retroperitoneum while the stent-graft remained in position (B). Follow-up CT confirmed the reduced size of the AAA and the absence of the retroperitoneal hematoma after surgical decompression. EVAR indicates endovascular aneurysm repair; rAAA, ruptured abdominal aortic aneurysm; CT, computed tomography.
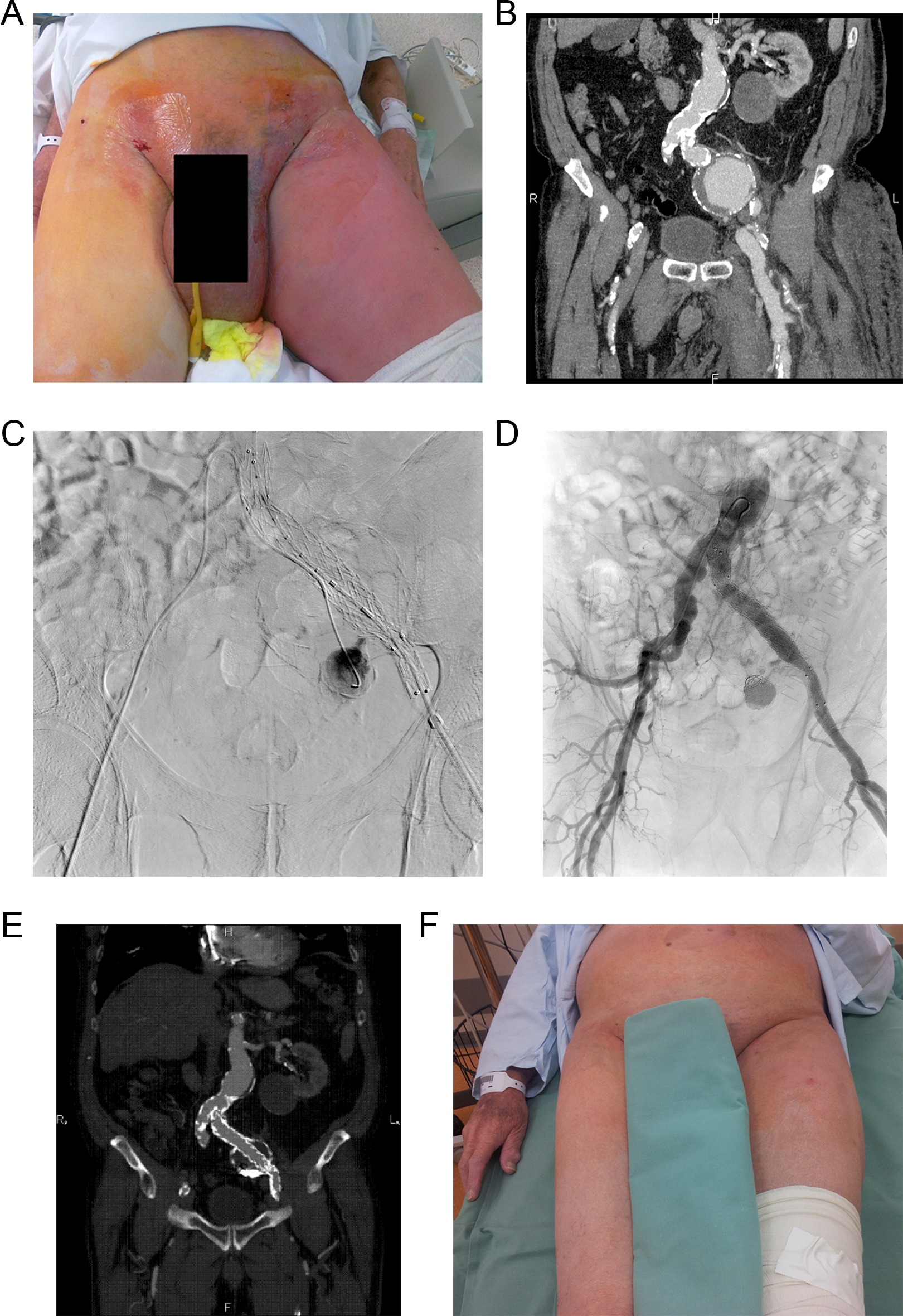
A 77-year-old man with significant edema of the left lower leg and incipient heart failure (A). Contrast-enhanced CT discovered a left common and internal iliac artery aneurysm (60 mm) and early filling of the dilated left common iliac vein. A diagnosis of an ilioiliac arteriovenous fistula was established (B). A diagnostic 5F catheter was introduced from the right side into the internal iliac aneurysm, and a tubular stent-graft was implanted from the left side (C). The tubular stent-graft reduced the filling of the fistula and facilitated embolization of the IIA aneurysm with coils and acrylate glue (D). The clinical status of the patient immediately improved after EVAR, and follow-up CT confirmed a reduction in the aneurysm size and occlusion of the fistula (E and F). CT indicates computed tomography; EVAR, endovascular aneurysm repair; IIA, internal iliac artery.
Patients With Ruptured Aortoiliac Aneurysms.
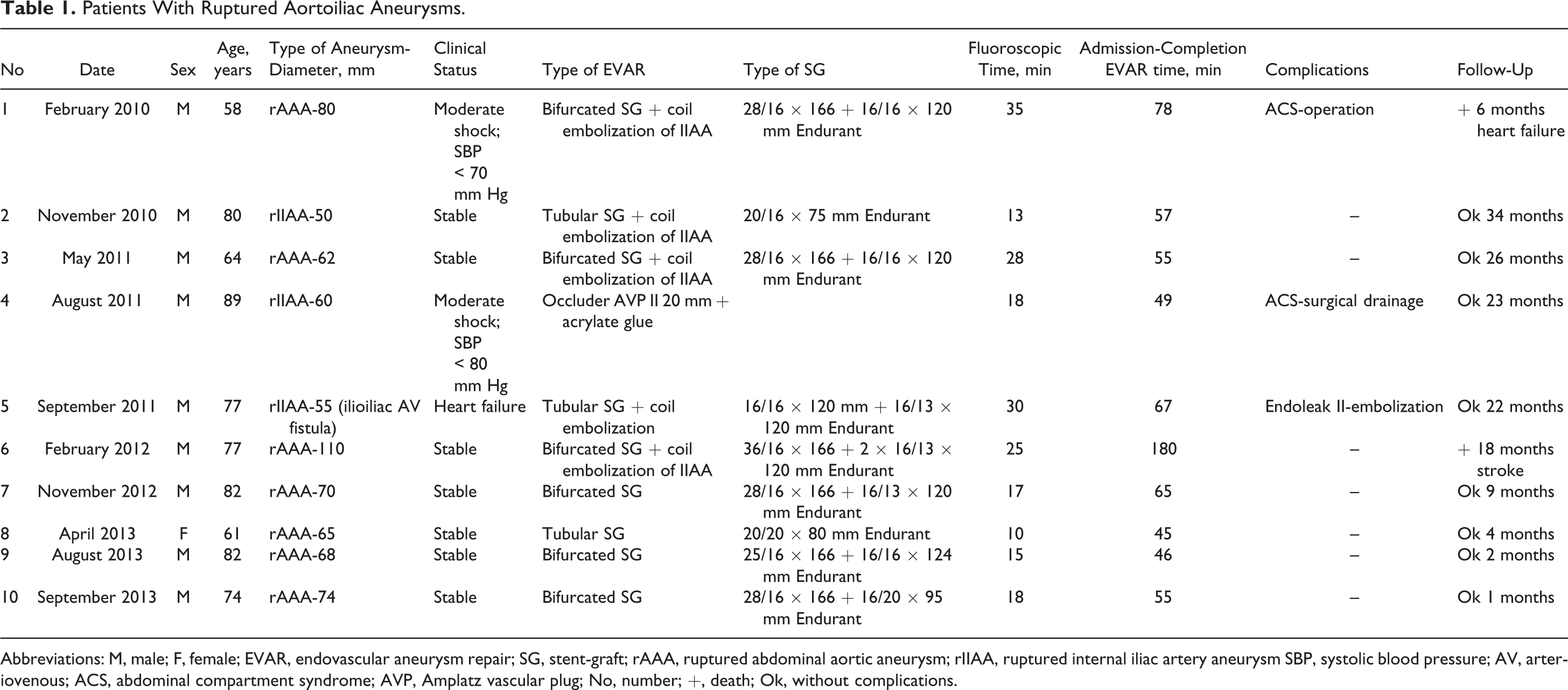
Abbreviations: M, male; F, female; EVAR, endovascular aneurysm repair; SG, stent-graft; rAAA, ruptured abdominal aortic aneurysm; rIIAA, ruptured internal iliac artery aneurysm SBP, systolic blood pressure; AV, arteriovenous; ACS, abdominal compartment syndrome; AVP, Amplatz vascular plug; No, number; +, death; Ok, without complications.
Discussion
The benefits and effectiveness of acute endovascular treatment were first demonstrated in our center in thoracic emergencies such as blunt aortic injury or ruptured aortic dissection type B. The logistic problems that arose during the transportation of such patients under life-threatening conditions provided a basic lesson in creating the organizational readiness of our center. 11,12
The basic prerequisite for initiating an EVAR program for the treatment of rAAAs is an experienced vascular center that can utilize the classic open-repair approach and offer elective EVAR treatment for AAAs. Other requirements include the 24/7 availability of a CT scanner, an angiographic theater, and a team that is trained in EVAR. In addition, various sizes of stent grafts must be available in the ward. Many reports have described the feasibility and efficiency of EVAR for rAAA. Some centers have even suggested a paradigm change and prefer EVAR as a first-line therapy. 13
The centers that implemented a specific intention-to-treat EVAR protocol for ruptured aneurysms demonstrated a decrease of approximately 50% in overall mortality compared to only surgical treatment before the protocol (19.7% vs 36.3%). 14 –16
Our study confirmed a positive role of EVAR in the complex treatment of rAAAs, with a 8.6% reduction in overall mortality. The small reduction in mortality can be explained by the low prevalence of EVAR (22.2%) in our study. This likely corresponds to strict compliance with the indication criteria for commercial stent-grafts, where a well-defined infrarenal neck of at least 10 mm should be present. To date, we have no experience with the treatment of juxtarenal aneurysms using fenestrated or branched stent-grafts. 17 Additionally, we have not yet applied parallel techniques, such as chimney or snorkel grafts. 18 Some of the centers that apply these adjunctive techniques can offer the complete replacement of open repair for rAAAs by EVAR, with low 30-day mortality (24%) and a minimal exclusion rate (4%). 19
Although the use of endovascular treatment for rAAAs is increasing, 20 recently published randomized trials have not shown a clear benefit of EVAR.
A pilot randomized trial conducted from 2003 to 2006 compared surgical treatment with endovascular treatment in patients with rAAAs in Nottingham, England. The results of this trial did not confirm this difference and revealed that the 30-day mortality rate for both the treatments was 53%. 21
This trial demonstrated the logistical and organizational demands of treating rAAAs. The benefit of EVAR has also not been shown in a randomized Amsterdam Acute Aneurysm (AJAX) trial. The mortality rate of the EVAR group was 21% whereas that in the open repair group was 25%. The low mortality associated with surgery can be explained by the centralization of care in centers of expertise and by the optimization of logistics. 22 Two other randomized trials are underway: the French Endovascular versus Conventional Aneurysm Repair Trial (ECAR) and the Immediate Management of the Patient with Rupture: Open Versus Endovascular Repair Trial (IMPROVE). The aim of these trials is to determine the optimum treatment of ruptured aneurysms. 23,24
Centers where EVAR is applied as a first-line treatment of rAAAs used the following guidelines to increase the effectiveness of the endovascular approach. The creation of a specific protocol by a vascular center to standardize the treatment of patients with rAAAs.
25
According to the capabilities of our center, we have defined a specific protocol for treating rAAAs using both endovascular and surgical approaches (Figure 1). Stratification of patients for EVAR or open repair is performed according to CTA. Whenever optimal anatomy was confirmed by CTA, EVAR was used as a first-line treatment. Patients with inappropriate anatomy for EVAR or cases in which CTA could not be performed were treated surgically.
Restriction of fluids (permissive hypotension): The restricted administration of fluids and the maintenance of systolic pressure at 70 mm Hg are tolerated by patients and reduce internal bleeding and the loss of platelets and coagulation parameters.
26
Local anesthesia and percutaneous access in EVAR keeps the abdominal wall tense and limits internal and retroperitoneal bleeding, which is preferred to general anesthesia.
27
In addition to percutaneous access, which uses closure devices (the preclose technique), the fascia-suture technique can be used. This technique is performed at the end of the intervention after extracting the delivery sheath of the stent graft and is based on injecting soft tissue and fascia above the common femoral artery without the need for a direct suture of the artery.
28
The use of endovascular occlusion of the aorta using a balloon delivered via femoral access above the location of the perforation in patients who are in hemorrhagic shock with collapsed circulation.
29
Early diagnosis and the treatment of abdominal compartment syndrome, which is the most frequent cause of post-EVAR mortality.
30
This EVAR-specific complication occurs primarily in patients with a large retroperitoneal hematoma. The hematoma and diffuse visceral edema lead to an increase in intra-abdominal pressure and, subsequently, to multiorgan failure (intestinal passage disorder and diuresis disorder). Generally, intra-abdominal pressure is monitored via a urethral catheter, and when the pressure increases above 30 cm of water, surgical decompression and revision is performed.
The main limitations of our study include the small number of patients and their selection. We applied EVAR after CTA stratification and in cases with a relatively stable hemodynamic condition. So the EVAR patients were most likely in better clinical condition (shape) than the surgical group. All EVAR patients underwent CT, but in the surgical group, only 28 patients had CT and 7 were operated just according to ultrasound. These 7 patients were hemodynamically unstable. The small number of patients was due to our being a medium-volume vascular center, where less than 50 AAA repairs are performed annually. Our standard EVAR technique, which is performed in an angiosuite without equipment for open repair, cannot be offered for patients who were severely hemodynamically unstable. A hybrid operating room that enables the performance of both treatments in one location without increasing time in transport is an ideal solution for treating ruptured aneurysm. When a hybrid theater is available, the center will perform endovascular treatment in unstable patients without a preprocedural CT examination. 31
Conclusion
Endovascular treatment of ruptured abdominal and iliac aneu-rysms is technically feasible, with very promising early results in this medium-volume vascular center. After integration, EVAR decreased total mortality by 8.6%. Strict use of the recommended indications for commercially available stent grafts led to the low prevalence of EVAR in our study and only a slight reduction in overall mortality.
Footnotes
Acknowledgments
We thank all colleagues and medical staff from various specialties who participated in the organization of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Work was supported by internal grant of our center and with the approval of the local ethics committee.