
Abstract
Background:
Lymphaticovenular anastomosis (LVA) is becoming a treatment option for lymphedema. It is challenging to perform LVA when a lymphatic vessel is too far from a vein to anastomose directly.
Methods:
We applied vein grafting for simultaneous multisite LVA (SM-LVA), when there was a considerable distance between a lymphatic vessel and a vein. Five patients with lower extremity lymphedema (LEL) who underwent SM-LVA were included in this study. Feasibility and treatment effect of the method were evaluated.
Results:
Simultaneous multisite LVA resulted in 35 anastomoses. Vein grafting was performed in 5 of 35 anastomoses with 100% technical success. All LVAs showed good intraoperative anastomosis patency. At 6 months postoperatively, LEL index was significantly lower than preoperative LEL index (251.0 ± 33.0 vs 271.0 ± 38.5, P < .001).
Conclusion:
In SM-LVA surgery, a vein can be harvested from another surgical field without additional invasiveness and is useful for bridging a lymphatic vessel and a distant vein.
Keywords
Introduction
Treatment of lymphedema is challenging, especially when the disease is refractory to conservative therapies. Several surgical treatments are reported for refractory lymphedema, which are largely classified into debulking surgery and physiological surgery. Debulking surgery directly reduces lymphedematous volume by resection or liposuction but does not address the underlying pathophysiology of lymphedema, lymphatic obstruction. 1,2 Thus, recurrence or re-exacerbation of lymphedema is not uncommon. Procedures whose goal is to restore lymphatic function or reduce lymphatic obstruction can be thought of as physiologic surgeries. Lymphatic supermicrosurgery or supermicrosurgical lymphaticovenular anastomosis (LVA) is the least invasive surgery, in which lymph flow is diverted into venous circulation. 3 -5 In lymphatic supermicrosurgery, one must identify a lymphatic vessel and a vein suitable for LVA. Suitable vessels, however, cannot always be found, and sometimes the initial 2-cm skin incision must be elongated. When a lymphatic vessel is too far from a vein to anastomose directly, vein grafting can serve as a useful method for bridging the vessels.
We have previously demonstrated that treatment efficacy of LVA correlates with the number of bypasses performed. 4 -9 In this study, we employ simultaneous multisite LVA (SM-LVA) in lymphatic supermicrosurgery to increase the number of bypasses. To achieve this most efficiently, multiple operators perform LVA simultaneously at multiple sites using multiple operating microscopes. 4 -6,9 -11 In conventional vein-grafting method, one has to make a new incision to harvest a vein, which results in an additional scar. Unlike conventional vein grafting, SM-LVA utilizes a vein procured from other surgical fields without the need for an additional incision; a vein can be harvested from a vein-redundant region such as the groin where another surgeon performs LVA. The purpose of this study is to evaluate the feasibility of vein grafting in SM-LVA and short-term outcomes.
Materials and Methods
The SM-LVA operations were performed on 5 patients with secondary lower extremity lymphedema (LEL) refractory to conservative treatments including skin care, elastic stockings, and manual lymph drainage. All patients had undergone radical hysterectomy and pelvic lymphadenectomy for uterine carcinoma treatment and suffered from progressive lymphedema due to obstruction of lymph flow at the pelvic region. Patients’ age ranged from 53 to 68 years (average, 61.0 years), body mass index ranged from 19 to 25 (average, 22.4), and leg dermal backflow stage determined by indocyanine green (ICG) lymphography ranged from stage I to stage IV (Table 1 and Figure 1). 12,13
LDB Stage Based on ICG Lymphography Findings.
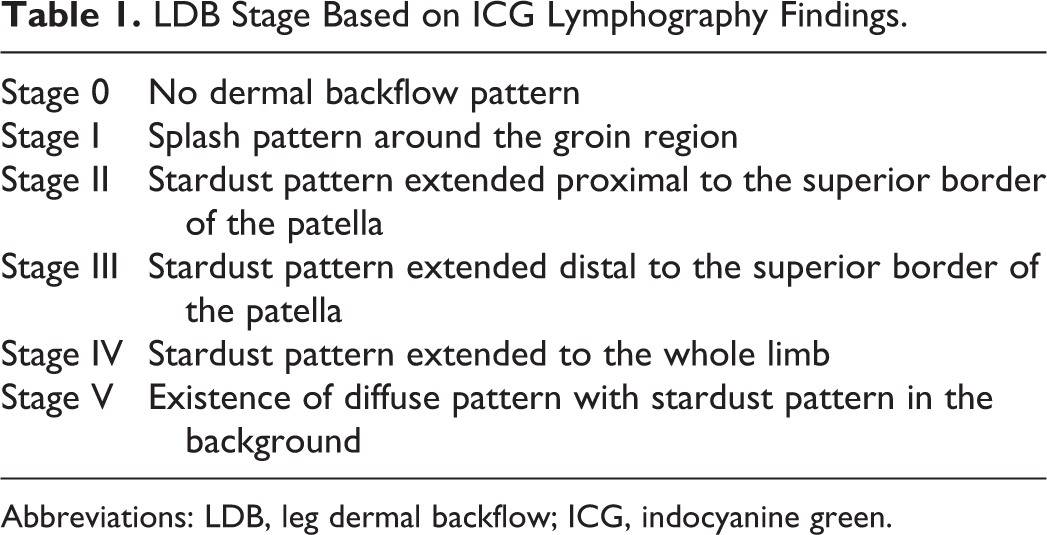
Abbreviations: LDB, leg dermal backflow; ICG, indocyanine green.
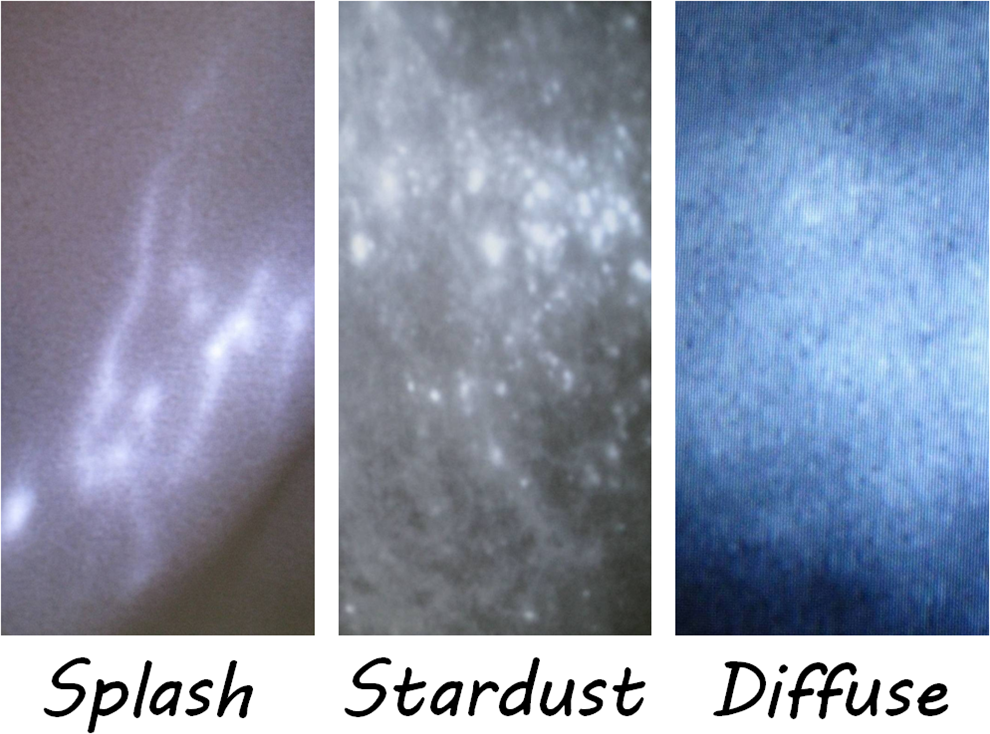
Indocyanine green lymphography (ICG) patterns and progression of lymphedema. ICG lymphography pattern changes from normal linear pattern to abnormal dermal backflow patterns (splash, left; stardust, center; diffuse, right).
In SM-LVA, LVAs were performed simultaneously at multiple sites by multiple surgeons. Skin incision sites were determined based on preoperative ICG lymphography findings and were usually made along the greater saphenous vein. 2,4 -11 Veins were harvested from a surgical field with redundant veins and utilized in a surgical field where a lymphatic vessel was too far from a vein to anastomose directly (Figure 2A–C). Harvested veins were used to bridge a lymphatic vessel and a vein, and microsurgical anastomoses were performed in an intima-to-intima coaptation manner using 11-0 or 12-0 nylon microsutures (Figure 2D). Lymphaticovenular anastomosis was performed preferably in a side-to-end fashion, whenever a lymphatic vessel was not too sclerotic to create a lateral window for a side-to-end anastomosis. 4 -11 Patency of the anastomosis was confirmed by lymph fluid washout into the vein by visual inspection under an operating microscope. Seven days postoperatively, patients resumed using daily 30 to 46 mm Hg elastic stockings. This ensured that lymphatic pressure remained higher than venous pressure so as to keep lymphatic flowing toward the lower pressure venous system.

Vein grafting from a different surgical field in simultaneous multisite lymphaticovenular anastomosis (LVA), “the right vein in the right place” method. There are a lymphatic vessel (arrow) and a vein (arrowhead) in a surgical field, but the vessels are too distant to be anastomosed directly in a side-to-end fashion (A). In a different surgical field, there are redundant veins more than enough for lymphaticovenular anastomosis there (B). A vein graft (asterisk) is harvested from the surgical field mentioned in B (C). The vein graft is used to bridge the lymphatic vessels and the vein in the surgical field mentioned in Figure 1A (D).
Feasibility and intraoperative patency of the method were evaluated. Lymphedematous volume was evaluated preoperatively and 6 months after the operations using LEL index (Figure 3). 14 Subjective symptoms such as sensation of tension and hardness of skin were assessed. Student paired t test was used to compare differences between pre- and postoperative LEL index. A statistical significance was defined as P value < .05. This retrospective observational study was performed in accordance with the ethical guidelines for clinical studies at the University of Tokyo Hospital. All patients gave written consent to this study.
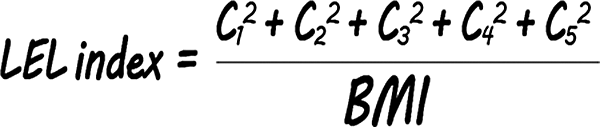
Calculation of lower extremity lymphedema (LEL) index. A summation of squares of circumferences C1, C2, C3, C4, and C5 (cm) divided by body mass index (BMI, kg/m2) is defined as the LEL index. C1 denotes circumference at 10 cm above the superior border of the patella, C2 circumference at the superior border of the patella, C3 circumference at 10 cm below the superior border of the patella, C4 circumference at the lateral malleolus, and C5 circumference at the dorsum of the foot. The LEL index <250 indicates mild edema, the LEL index of 250 to 300 moderate edema, and the LEL index >300 severe edema.
Results
Thirty-five LVAs were performed on 7 lymphedematous limbs of 5 patients. Vein grafting was performed to bridge a lymphatic vessel and a vein in 5 of 35 anastomoses (Table 2). All veins were grafted from a different surgical field in SM-LVAs, where LVA was successfully performed; and there was no adverse effect due to harvesting a vein graft. Length of veins used as interpositional grafts ranged from 8 to 15 mm (average, 11.0 mm). All vein graft-bridged LVAs were performed by 1 surgeon (TY). Time required for LVA using a vein graft (lymphatic-to-graft and graft-to-venous anastomoses) ranged from 13 to 23 minutes (average, 17.2 minutes). All anastomoses including the recipient and the donor sites of the vein grafts were successfully performed with good intraoperative patency, and no revision for anastomosis was needed. All patients reported improvement in sensation of tension and skin hardness. The LEL indices 6 months after LVA ranged from 207 to 286 and were significantly lower than preoperative LEL indices (251.0 ± 33.0 vs 271.0 ± 38.5, P < .001), consistent with postoperative lymphedematous volume reduction.
Multiple LVAs With Vein Grafting on 7 Limbs of Patients With Secondary LEL.
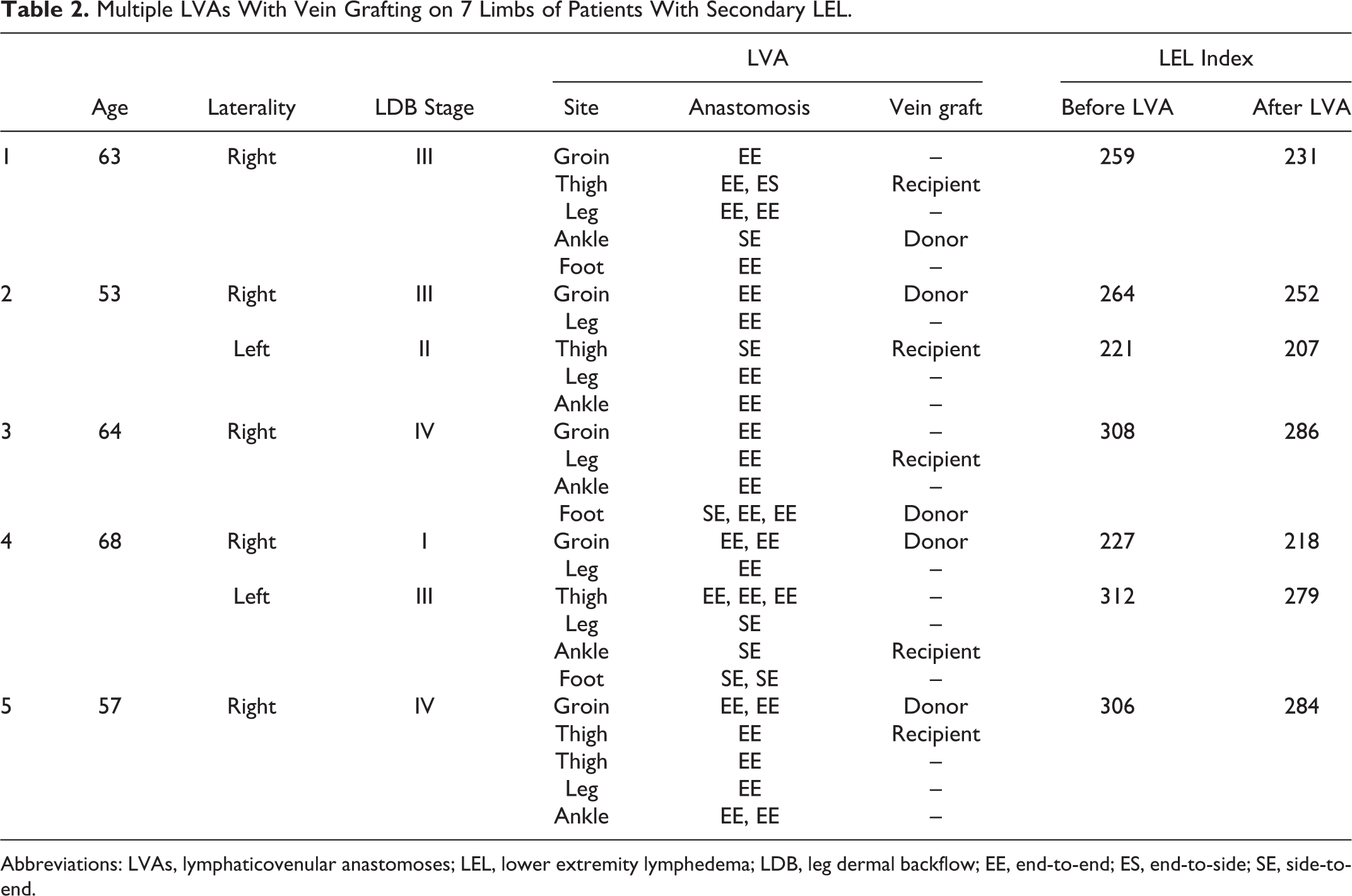
Abbreviations: LVAs, lymphaticovenular anastomoses; LEL, lower extremity lymphedema; LDB, leg dermal backflow; EE, end-to-end; ES, end-to-side; SE, side-to-end.
Discussion
Obstruction of lymph flow secondary to cancer treatments such as lymph node dissection and radiotherapy leads to lymphatic hypertension, dilatation of lymphatic vessels, extravasation of lymph fluid, and chronic progressive lymphedema. 2,12,15 In physiological lymphovenous shunt surgeries, congested lymph flows are diverted into venous circulation distal to obstruction sites. 1,16 -19 Since lymph originally flows into venous circulation at the venous angle, lymphovenous shunts are considered physiological and address pathophysiology of obstructive lymphedema. Regardless of primary cancer pathology, lymphovenous shunt can be used to treat lymphedema secondary to lymph flow obstruction in the pelvic region due to pelvic lymphadenectomy or irradiation. Although widely used as in the management of lymphedema, compression treatment does not address the pathophysiology of lymphedema. Some believe that physiological surgery may help prevent lymphedema progression when conservative treatments fail to control the disease. In this study, all patients had progressive lymphedema; lymphedematous volume increased in spite of long-term conservative treatments including skin care, elastic stockings, and manual lymph drainage. Lymphovenous shunt operation can be considered for any patients with progressive lymphedema refractory to conservative treatments.
Supermicrosurgical LVA is a lymphovenous shunt operation which has become more popular with advent of supermicrosurgical instruments and refinement of technique. 2 -11 In lymphatic supermicrosurgery, a lymphatic vessel is anastomosed to a small vein or a venule in an intima-to-intima coaptation manne. Unlike classical lymphovenous shunt operations, only endothelium tissues are exposed to fluids flowing inside the lumen. 1 -11,16,17,19 -21 Thus, anastomosis site obstruction would be lower in LVA than in classical lymphovenous shunt operations. Furthermore, LVA can be performed under local infiltration anesthesia via a 2-cm skin incision, and LVA is the least invasive among physiological surgeries and considered a method of choice for the treatment of refractory lymphedema.
A minimum requirement for lymphatic supermicrosurgery is finding a lymphatic vessel and a vein suitable for anastomosis. Finding lymphatic vessels suitable for anastomosis is facilitated by ICG lymphography but is sometimes difficult and requires elongation of the skin incision to procure suitable vessels. 12,13,22 -28 As demonstrated in this study, vein grafting can be helpful in bridging a lymphatic vessel to a draining vein when the distance between 2 or discrepancy of vessels’ diameter is prohibitive. A vein graft can be used not only to connect a lymphatic vessel to a distant vein but also to prevent venous backflow by providing an intact valve within the grafted vein. 29,30 In SM-LVA, multiple lymphatic supermicrosurgeons simultaneously perform LVAs at different sites, one operating at the level of the groin and another at the thigh, and so on. 5,6 Usually, there are multiple veins at the groin and at the foot, whereas there are not as many suitable veins available for harvest at the thigh and at the leg. 31 -35 Furthermore, lymphatic vessels are deep and distant from veins at the thigh and the leg. A vein graft harvested in the groin or the foot can often be used at the thigh and the leg. Unlike vein grafting in a conventional situation, our approach, vein-grafting form another surgical field in SM-LVA, can harvest a vein without an additional donor scar; a vein is harvested from a vein-redundant region such as the groin and the foot where another surgeon performs LVA.
Major drawbacks of the present technique are that it is necessary to perform 2 anastomoses per 1 LVA and that multiple microscopes and lymphatic supermicrosurgeons are required. Although vein graft-bridged LVA requires 2 anastomoses per 1 LVA, our approach can bypass a distant lymphatic vessel without extending the skin incision or creating a new scar at the donor site.
Vein grafting is not always indicated in LVA surgery. It is best employed when vessels are too distant to anastomose directly and when there are multiple microscopes and surgeons available. If a surgeon is performing LVA by himself or herself and finds a lymphatic vessel is too distant to anastomose to a vein directly, a vein graft can be harvested from the new surgical field before elongating the original skin incision and then utilized as to perform a vein graft-bridged LVA.
The greatest limitation of this study is the small sample size, only 5 patients and 7 limbs. Moreover, it is difficult to confirm the direct treatment efficacy of the method, since LVAs using the present technique were only employed in a fraction of cases, whereas the conventional direct LVAs were performed on majority of the limbs. However, this study supports previous reports suggesting that treatment efficacy of LVA surgery positively correlates with the number of anastomoses. We propose that the multisite LVA using vein grafts can improve overall results of LVA surgery by maximizing the number of anastomoses. 4 -11 In addition, SM-LVA maybe avoid the need for longer incisions, otherwise necessary for exposing and identifying adequate veins for direct LVA. Furthermore, in some cases, this technique can allow for treatment otherwise not possible due to anatomic distances between vein and lymphatic precluding conventional LVA. Although the number of patients included in this study was small, the present technique allowed successful LVAs at the all surgical fields where a lymphatic vessel was too distant from a recipient vein, which resulted in increased number of anastomoses.
In addition, we are only able to note intraoperative patencies and are unable to determine the postoperative patency of our anastomoses (regardless of technique). Thus, we cannot comment on the long-term effectiveness of the adjunctive vein-grafting technique. The improvement in LEL indicates successful LVA but we are unable to comment on the 5 vein grafts and their direct impact on the LEL improvement. Future studies, exclusively utilizing the vein-graft technique would be better suited to determine the efficacy of this technique. Our study simply proposes an adjunctive technique for increasing total number of anastomoses, which has been shown to correlate with improved outcomes.
Finally, our study is further limited as it only included only uterine cancer-related lymphedema after pelvic lymphadenectomy, and other patients with secondary LEL were not included. Pathophysiology of LEL secondary to pelvic cancers other than uterine cancer is basically the same as that of uterine cancer-related LEL, lymph flow obstruction in the pelvic region. Our technique may not be useful for LEL secondary to inguinal lymphadenectomy, because the inguinal region where there are many veins available for our technique is already damaged during the previous operation.
Although further investigations are needed to clarify its efficacy and indications, vein grafting from another surgical field in SM-LVA is a useful method to bypass a lymphatic vessel distant from a vein, requiring no additional scar.
Conclusion
Vein grafting in SM-LVA is a feasible technique for bypassing a lymphatic vessel to a distant vein without additional incision in patients with uterine cancer with LEL. Although indications are limited, the described approach is useful in performing vein graft-bridged LVA, providing there are multiple microscopes and multiple lymphatic supermicrosurgeons available. Finally, this technique, when used adjunctively during conventional LVA, can result in increased number of anastomoses which has been previously shown to improve outcomes in patients with lymphedema.
Footnotes
Acknowledgments
We would like to thank Rico and all members in our department for their kind support to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported, in part, by Takeda Science Foundation (to T.Y.).