
Abstract
Extracranial carotid artery aneurysms located in the cervical region in close proximity to the skull are difficult to access using open surgical methods. Endovascular treatment has emerged as an alternative option for anatomically challenging internal carotid artery aneurysms. However, data comparing various endovascular techniques including stent grafting, coil embolization, double stenting, and stent-assisted coil embolization are lacking, making it difficult to determine the optimal treatment. We present a case of a patient with 2 fusiform extracranial carotid artery aneurysms treated successfully with a combination of double stenting and stent-assisted coil embolization. We also discuss technical considerations for selecting the appropriate endovascular intervention.
Introduction
Extracranial carotid artery aneurysms (ECCAs) are rare, comprising only 0.4% to 4% of all peripheral artery aneurysms and 0.1% to 2% of all carotid artery procedures performed. 1 -4 Carotid artery aneurysms are most often caused by atherosclerotic disease (40%) but can also be secondary to trauma (14%), dissection (12%), fibromuscular dysplasia (8%), and infection (2%). Pseudoaneurysms account for 21% of all ECCAs. 4 If left untreated, the aneurysm can progress to rupture, distal embolization, and thrombosis causing devastating neurologic sequelae. 2,5 Open surgical treatment to achieve aneurysm obliteration with carotid reconstruction has been the gold standard for accessible lesions. However, with recent advancements and increasing experience, endovascular treatment is emerging as an alternative treatment, particularly anatomically challenging lesions or inaccessible. 6
We report a case of a patient who presented with 2 fusiform distal ECCAs that were treated successfully with stent-assisted coil embolization and double bare-metal stenting.
Case Report
A 74-year-old male presented with worsening left neck pain and an enlarging pulsatile neck mass over 2 weeks. He did not have a history of previous neck surgery, signs of infection, or other constitutional symptoms but did report a history of fall to the left side of the body approximately 1 year ago with no apparent sequelae at the time. The patient’s past medical and surgical history included atrial fibrillation, anxiety disorder, gastroesophageal reflux disease, hyperlipidemia, biliary sepsis 2 years prior, and cholecystectomy. His medications included aspirin, pantoprazole, simvastatin, and citalopram. He did not smoke or drink alcohol. Physical examination revealed a soft, 2-cm pulsatile left neck mass. No bruits were auscultated. Cranial nerves II through XII were intact. Neurological examination revealed normal motor and sensory functions throughout. The remainder of the physical examination was unremarkable with normal pulse examination and no other palpable pulsatile masses. The patient’s blood work, including ESR and CRP, were within normal limits. Blood cultures showed no growth. Computed tomography angiography (CTA) demonstrated a 2-cm distal left internal carotid artery (ICA) aneurysm at the level of C1 vertebrae and a second 8-mm ICA aneurysm at the skull base (Figure 1).
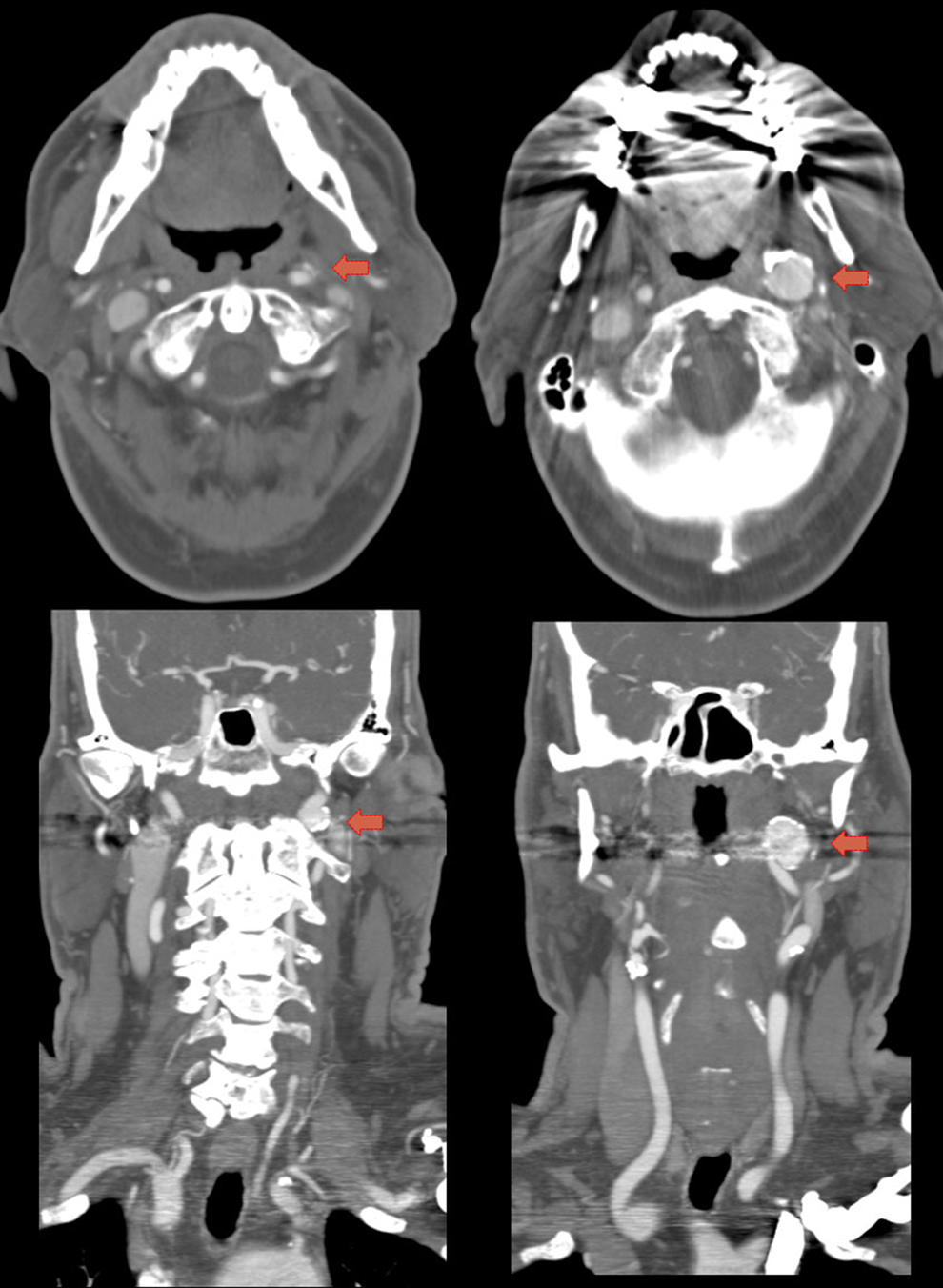
Computed tomography (CT) angiography demonstrating a (left top and bottom arrows) 8 mm aneurysm and a (right top and bottom arrows) 2 cm internal carotid artery aneurysm in axial and coronal views.
Diagnostic angiogram with selective 4-vessel cannulation of cerebral vessels demonstrated widely patent right carotid and bilateral vertebral arteries without significant disease. Two fusiform aneurysms were demonstrated in the left ICA (Figure 2). An intraprocedural balloon occlusion test was performed revealing no neurologic deficits after 30 minutes of occlusion and 5 minutes of induced hypotension. After discussing the risks and benefits of his therapeutic options, the patient and the surgical team agreed to proceed with stent-assisted coil embolization of the larger aneurysm and double stenting of the smaller aneurysm.
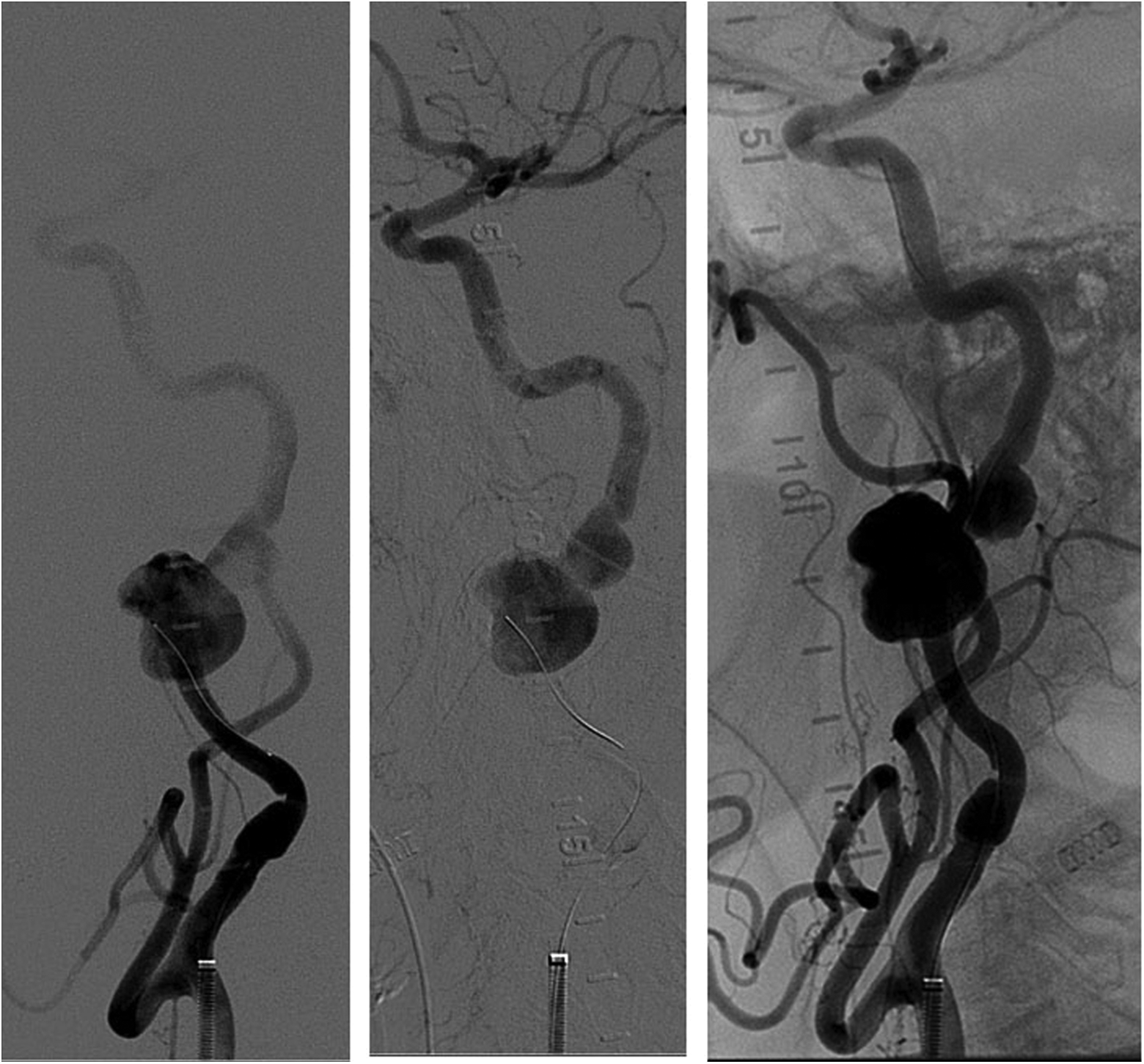
Selective left internal carotid angiogram demonstrating 2 distal internal carotid artery aneurysms close to the base of the skull.
A 7 × 30 mm Cordis PRECISE (Bridgewater, New Jersey) bare-metal stent was placed across the smaller distal aneurysm while also partially covering the proximal aneurysm. A second 8 × 40 mm Cordis PRECISE stent was deployed completely covering both the distal and the proximal aneurysms (Figure 3A). Angiogram following stent deployment demonstrated stagnant flow across the smaller distal aneurysm and continued flow through the larger proximal aneurysm. A Synchro-2 microwire and Penumbra PX400 microcatheter were used to gain access through the stent lattices into the larger aneurysm sac. Penumbra 400 standard coils of 14 mm × 50 cm and 13 mm × 48 cm were sequentially placed (Figure 3B). A completion angiogram demonstrated stagnant flow in both aneurysm sacs and intact cerebral circulation without evidence of thromboembolism (Figure 3C). The patient tolerated the procedure well without any complications and was discharged home on postoperative day 1.
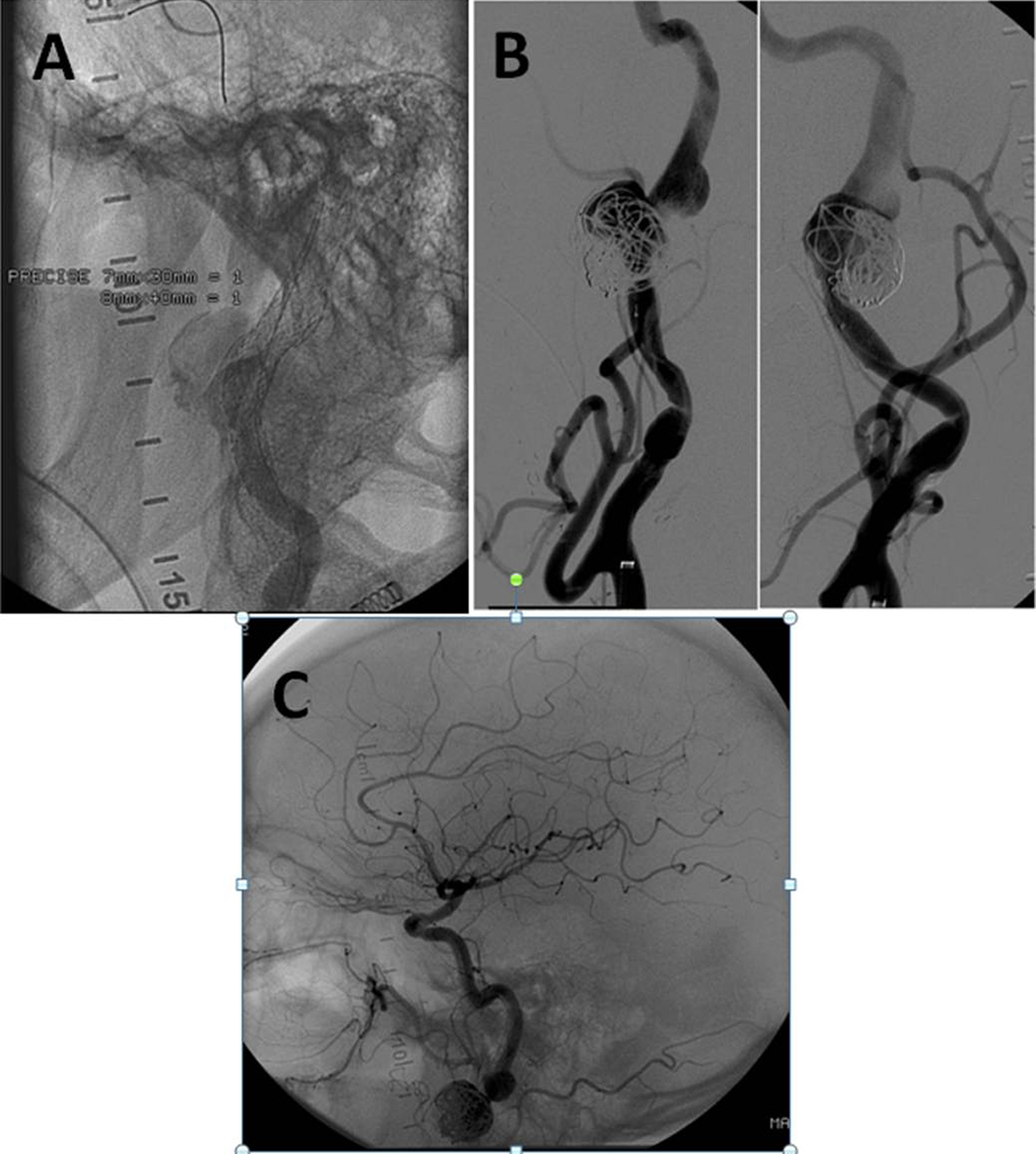
A, 7 ° 30 mm Cordis PRECISE stent was placed covering the distal 8 mm aneurysm, then a 8 × 40 mm stent placed over both the distal and the proximal aneurysm. B, The aneurysm sac was accessed through the bare-metal stent lattices with a microwire and microcatheter. 14 mm × 50 cm and 13 mm × 48 cm Penumbra 400 standard coils were deployed into the sac. C, Completion angiography demonstrates uncompromised cerebral blood flow and stagnant flow in the 2 aneurysm sacs.
The patient was seen for follow-up at 1, 3, and 6 months. The patient continued to do well without any neurologic deficits. The patient no longer complained of left neck pain. On physical examination, the pulsatile mass was no longer present. Duplex ultrasound demonstrated complete thrombosis of both aneurysms and widely patent carotid artery stents (Figure 4).
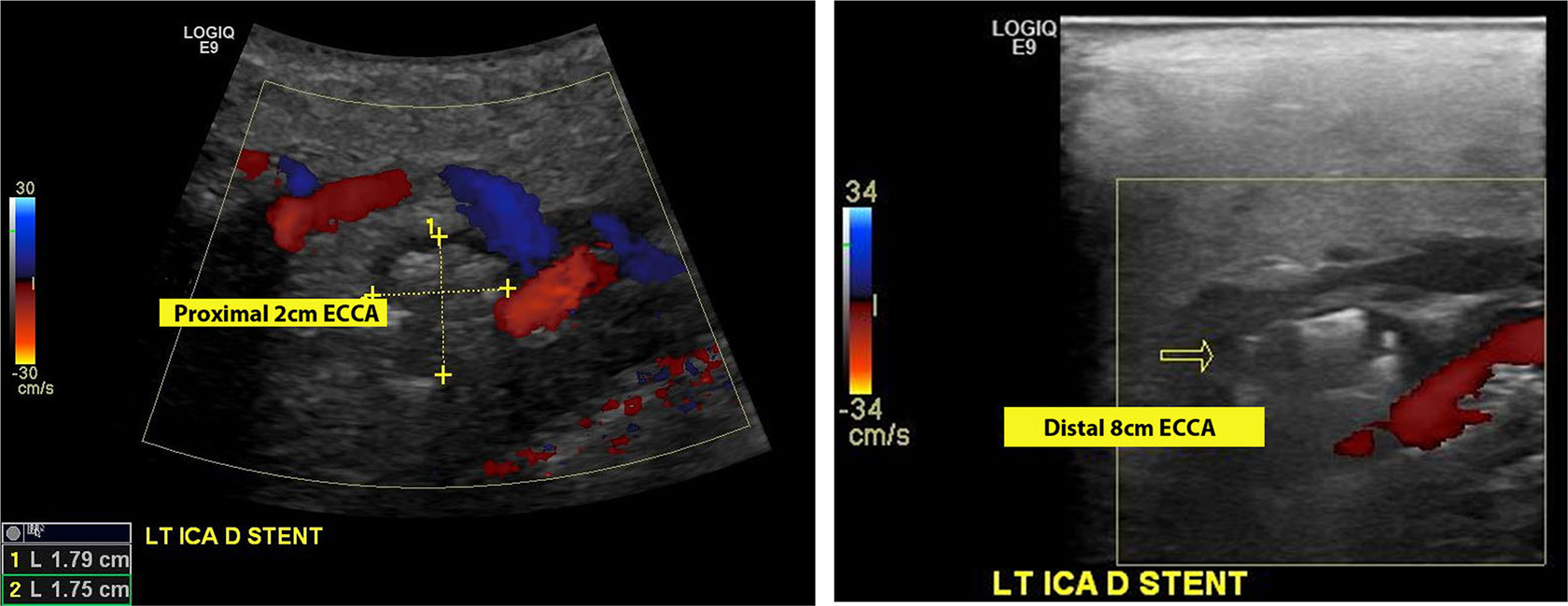
Duplex ultrasound at 1 month demonstrates complete thrombosis of both aneurysms and patent stents.
Discussion
The ECCAs can initially present with a variety of symptoms. A pulsatile mass is the most common finding seen in 93% of patients. 6 The percentage of patients presented with ischemic neurologic symptoms, including amaurosis fugax, transient ischemic attacks, and stroke, was 14% to 43%. 4,6 Larger ECCAs can present with mass effect including Horner syndrome, cranial nerve dysfunction, and dysphagia as a result of external compression of surrounding structures. Finally, patients, particularly those who have undergone extensive treatment of head and neck cancer, can present with hemorrhage or rupture of the aneurysm.
Atherosclerotic disease is the most common cause of ECCAs, responsible for 40% to 70% of all cases. 4 However, with advances in technology and higher rates of patients being imaged, ECCAs are increasingly identified as a result of other causes including dissection, fibromuscular dysplasia, and pseudoaneurysms following carotid interventions and trauma. 7 The location of the ECCAs can vary based on the etiology. Atherosclerosis will often cause aneurysms at the carotid bifurcation, penetrating trauma is typically associated with common carotid aneurysms, and blunt trauma will often lead to distal carotid artery aneurysms.
Early results of several studies have demonstrated favorable outcomes of ECCA repair with endovascular techniques. 8,9 In addition to providing equivalent, if not significantly improved, postoperative stroke and death rates, endovascular treatment also eliminates cranial nerve injuries that may be seen with open surgical repair. 6 In our patient, the balloon occlusion test revealed no neurologic abnormalities, illustrating that the patient could theoretically tolerate open surgical ligation of internal carotid artery if necessary. However, given the 15% failure rate of the balloon occlusion test to accurately predict postprocedural neurologic sequelae 10 and increased rates of cranial nerve injury during open surgical dissection, the patient elected to proceed with an endovascular treatment. The patient’s history, normal white blood cell count, normal inflammatory markers, and negative blood cultures lowered our suspicion for infected aneurysms, a general contraindication to endovascular repair for fear of placing a foreign body in a contaminated field.
For the treatment of ECCAs, a variety of endovascular techniques have been reported in the literature including placement of double stents, 11 coil or balloon embolization, 12 covered stent grafting, 9 and stent-assisted coil embolization. 13 Endovascular balloon occlusion with percutaneous thrombin injection has been described for the treatment of pseudoaneurysms. 14 However, there is a paucity of data on long-term outcomes comparing these techniques and a lack of consensus for the indication for each intervention.
Primary coil embolization risks nontarget embolization due to the fusiform nature of this patient’s aneurysms. In comparing covered stent grafts versus bare-metal stents, we considered the following. The tortuosity of our patient’s carotid artery may result in arterial kinking if a relatively rigid stent graft is used, compromising cerebral blood flow. The presence of 2 simultaneous ECCAs would require a longer area of coverage. In general, covered stent grafts have a higher risk of thrombosis than bare-metal stents. As a result, we selected bare-metal stents for use in our patient. For the proximal 2 cm ECCA, we used the Cordis PRECISE nitinol bare-metal stents with free cell area of 5.9 mm2 which allows passage of microcatheters for placement of coils. We used detachable Penumbra 400 coils for accurate deployment. The Penumbra coils have larger filling volumes compared to other coils and are also covered with Dacron, allowing increased thrombosis in the aneurysm sac. The distal 8 mm ECCA was considered too small for coil deployment, and a double stenting strategy was selected. The double layer of stent lattices reduces flow within the aneurysm sac. This stasis induces thrombosis of the aneurysm while maintaining luminal patency.
Conclusion
Endovascular treatment is an effective alternative to open surgery for ECCA repair. Smaller aneurysms can successfully be treated with double bare-metal stenting while larger aneurysms can be treated with bare-metal stent-assisted coil embolization. These techniques lead to complete thrombosis of the aneurysm sac while maintaining good cerebral blood flow.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.