
Abstract
Aortic graft infections are a rare occurrence, most commonly secondary to gram-positive organisms (Staphylococcus and Streptococcus species). We present 2 cases of thoracic aortic graft infections secondary to anaerobic bacteria, Propionibacterium species. The first case, a 40-year-old male, was found to have an anastomotic aneurysm at the distal anastomosis of a previous thoracoabdominal aneurysm repair. During the open repair of his anastomotic aneurysm, the original graft was not incorporated and cultures later speciated Propionibacterium acnes. The second case is a 44-year-old male with a history of abdominal aortic coarctation that was repaired with a thoracic aorta to aortic bifurcation graft as a child who presented with flank pain and was found on imaging to have fluid around his bypass graft. His operating room (OR) cultures also grew out Propionibacterium species. Both patients were treated with graft excision, revascularization, and long-term antibiotics. Anaerobic bacteria are a rare cause of aortic graft infections. Upon review of the literature, these are the first 2 cases of thoracic aortic graft infections secondary to Propionibacterium species. The cultures for both patients took almost a week to speciate, highlighting the importance of following cultures long term. Anaerobic bacteria should be recognized as a cause of latent graft infections.
Introduction
The lifetime incidence of aortic graft infections is approximately 1% to 3%. 1,2 Graft infections are most commonly secondary to gram-positive organisms such as Staphylococcus and Streptococcus species. Rarely, they are secondary to anaerobic bacteria. The Propionibacterium species are gram-positive anaerobes that live in skin follicles and to our knowledge have never been reported to be responsible for graft infection after open aortic repair. We present 2 cases of thoracic aortic graft infections that were secondary solely to Propionibacterium species.
Case 1
A 40-year-old male with no significant medical history presented to a local emergency department with acute-onset of interscapular back pain. A computed tomography angiogram (CTA) demonstrated a thoracoabdominal aortic aneurysm with marked fusiform dilation of the mid- to lower descending thoracic aorta that ended just distal to the celiac artery with a focal saccular component (9 × 8.1 cm) and a contained perforation (Figure 1). In addition, there was a soft tissue density within the mediastinum with an inflammatory reaction surrounding the aneurysm suggestive of a mycotic etiology. The patient had no marfanoid features nor any familial history of connective tissue disorders or aneurysmal disease. The patient was emergently transferred to Pennsylvania Hospital where he underwent thoracoabdominal aortic aneurysm repair with atrioaortic bypass. No compelling evidence of infection was found. A woven Dacron graft was sewn to the mid-thoracic aorta at the T5 level, with the distal anastomosis constructed in a beveled fashion incorporating the celiac, superior mesenteric artery (SMA), and renal arteries. Two pairs of intercostal arteries were reimplanted with the Crawford technique. Operative cultures were negative. Postoperatively, the patient did well and was discharged home without any complications on day 5. Because there was no definitive evidence of mycotic aneurysm, he was not discharged home on any antibiotics and did well for a period.
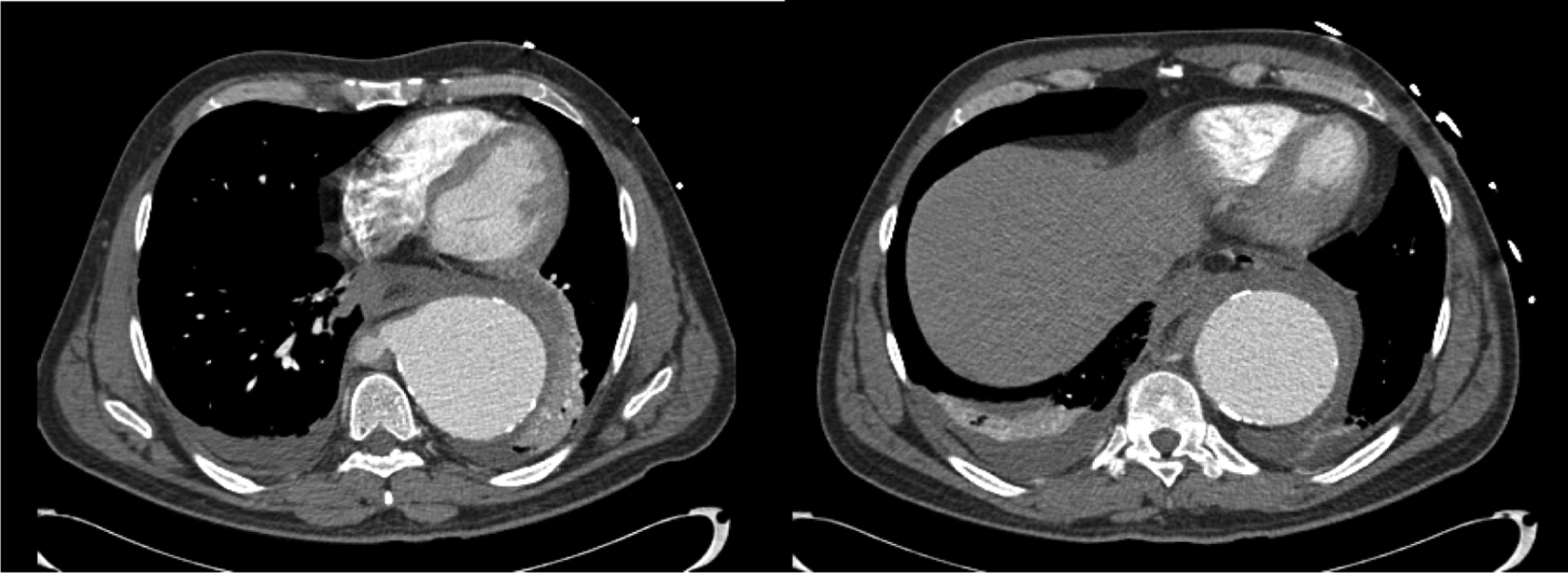
Computed tomography angiogram (CTA) of contained rupture of thoracoabdominal aortic aneurysm.
The patient was followed periodically with CTA by his local vascular surgeon and referred back to our clinic 8 years later with a recurrent thoracoabdominal aortic aneurysm at the distal anastomosis. In the intervening 8 years, he had no new medical problems or hospitalizations. The patient gave no history of pain, fevers, chills, or malaise. Computed tomography angiogram demonstrated an eccentric aneurysmal dilation proximal to the celiac trunk measuring 5.5 × 5.4 involving the ostium of the left renal artery, which represented a marked change compared with the prior study (Figure 2).

Computed tomography angiogram (CTA) of recurrent thoracoabdominal aortic aneurysm (TAA) 8 years after original TAA repair.
Thoracoabdominal aortic aneurysm repair was again performed with left heart bypass. At the time of operative exploration, the previous graft was found to be completely unincorporated into the surrounding tissue. The aortic tissue around the prior distal anastomosis was friable. Cultures were taken from the graft and aneurysm cavity. The celiac, superior mesenteric, and right renal arteries were reimplanted as a patch onto a new rifampin-soaked Dacron graft. The left renal artery was extremely friable to the hilum and could not tolerate suturing; an attempt at hybrid stent-graft deployment failed and a left nephrectomy was necessary. The proximal anastomosis to the aorta was performed at the T5 level, and previously reimplanted intercostals were oversewn.
Postoperatively, operative cultures grew Propionibacterium acnes only after 6 days in culture. The patient was treated with intravenous (IV) ceftriaxone. He recovered uneventfully without fevers, leukocytosis, or other evidence of sepsis and was discharged on postoperative day 7. He was treated with IV ceftriaxone for 6 weeks and then transitioned to oral doxycycline for long-term suppression therapy.
Case 2
A 44-year-old male with an extensive vascular history was referred to us with a chief complaint of left flank pain and an associated psoas muscle collection. He was diagnosed with abdominal aortic coarctation as a child. He had a history of a distal aorta-to-right renal bypass using the right internal iliac artery and a left splenorenal bypass when 6 years old, reimplantation of his celiac artery when 9 years old, and end-to-side distal thoracic aorta to abdominal aortic bifurcation bypass using a Dacron graft when 13 years old. His right renal bypass and aortoaortic bypass subsequently occluded. He did well with moderate lower extremity claudication symptoms until 2 months prior to being referred, when he developed flank pain and a psoas muscle collection. A percutaneous drain was placed; cultures of the fluid were negative, and the drain was removed. The flank pain recurred, and CTA demonstrated left psoas fluid collection near the occluded aortoaortic graft (Figure 3). He had a solitary functioning left kidney with a slightly elevated serum creatinine level (1.5 ng/dL).
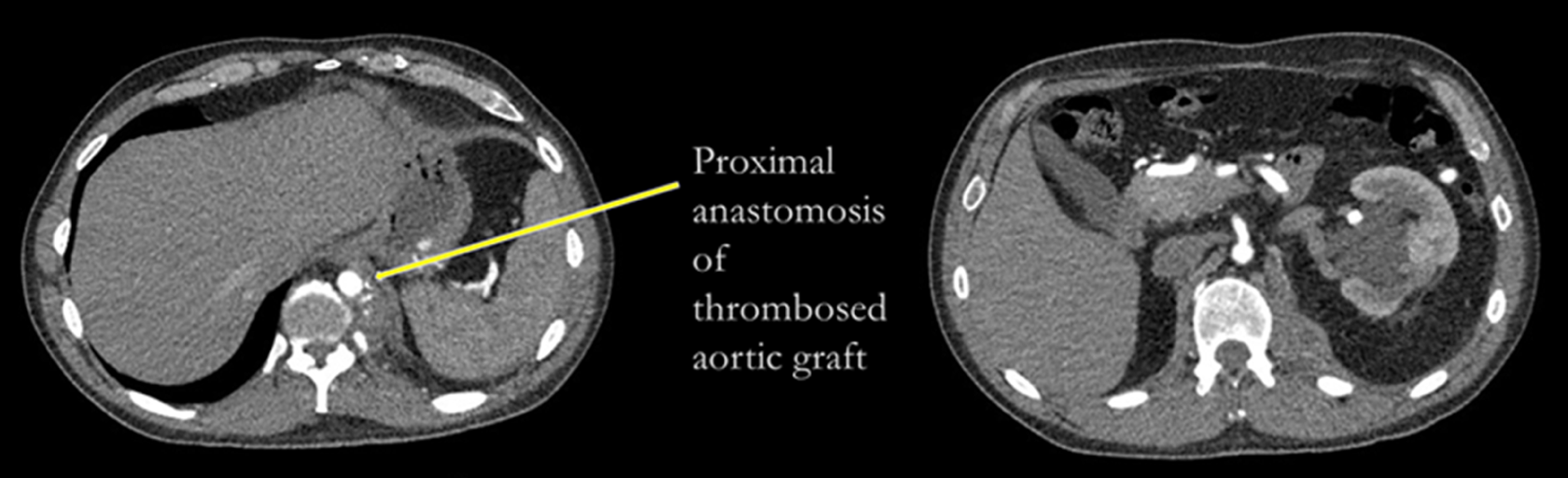
Computed tomography angiogram (CTA) of fluid surrounding occluded aorta–aorta graft.
The patient underwent bypass from his thoracic aorta proximal to the previous graft to the left common iliac artery with arterial cryopreserved allograft. This strategy allowed backperfusion up the stenotic distal aorta to potentially perfuse the mesenteric and left renal arteries, while the aorta was clamped to excise the infected end-to-side graft from the distal thoracic aorta. At the time of exploration, a large amount of purulent drainage was encountered in the psoas muscle and around the old aortic graft as well as within the graft. The aortic defect was closed with a cryoartery patch. Cultures were taken from this graft and grew Propionibacterium propionicum only after a week of incubation. The patient was discharged home without complication on postoperative day 9 and was treated with IV vancomycin for 6 weeks and then transitioned to oral doxycycline. A follow-up CTA prior to discharge and duplex ultrasound of the graft in our office 2 weeks later showed a patent aortic cryograft without fluid.
Discussion
Complications of abdominal aortic grafts are well documented. Anastomotic pseudoaneurysm is the most common complication of abdominal aortic aneurysm repair, with an estimated lifetime incidence of 3%. Graft infections are less common at 1%. 3 Even thoracic aortic graft infections have been reported, well under 1% lifetime incidence 4 ; mortality though for these rare cases can range from 25% to 80%. 5 –7 The bacteria isolated in these cases were similar to those for abdominal aortic graft infections: Staphylococcus or Streptococcus species. The largest institutional series was reported by Kieffer et al with 11 thoracoabdominal/thoracic aortic graft infections, most commonly growing Staphylococcus or Streptococcus species. 8 Our 2 cases appear to be the only reports from open aortic repair.
Propionibacterium species are anaerobic, gram-positive bacteria that live in skin follicles. It is transmitted in a similar method as other skin flora, but there are generally no specific skin-related symptoms. Anaerobic bacteria are rarely isolated from vascular graft infections. Propionibacterium acnes have been identified as a rare cause of other implants including breast, neurosurgical, spine, and cardiac valves. 9 In the vascular specific literature, Harlock et al published a report of an infrarenal aortic endograft infected with P acnes. 10 This was managed with graft explantation and the femoral vein in situ repair. This is the only reported case of an aortic graft infection secondary to P acnes.
In our first case, it is possible that the original aneurysm treated was a mycotic aneurysm. Mycotic aneurysms are rare; studies have shown them to be only 1.3% of all aneurysms. 11 The patient’s first aneurysm did present with rupture, which is a common presentation for mycotic aneurysms, and he had no risk factors for aneurysm at his young age. However, he did not have bacteria isolated at the time of the first operation nor did he have a history of any other infection at the time. The previous literature has demonstrated that a lack of bacteria isolated does not rule out a mycotic aneurysm. 12 However, it is possible that standard culture techniques may miss an anaerobic infection in these culture-negative aneurysms. Propionibacterium acnes have a characteristically slow growth and do not frequently grow on routine aerobic cultures. 13 In a study of aortic aneurysm wall culture using electron microscopy, the authors were able to identify anaerobes in 10 of 53 aneurysm samples, including P acnes. 14 This study, however, did not examine the impact of these positive cultures on long-term outcomes of the repair. Another report did describe a 75-year-old male who was found to have a mycotic aneurysm of an aortic stump secondary to P acnes. 15
The treatment of infected thoracoabdominal aortic aneurysm graft infections is difficult. Although infrarenal aortic aneurysms can be treated with extra-anatomic bypass, revascularization of abdominal viscera is best accomplished with in-line flow. In situ repair with a rifampin-soaked gelatin-coated Dacron is an accepted technique for this entity, usually in conjunction with long-term antibiotic therapy. Cryopreserved allograft revascularization is another accepted technique for revascularization in the setting of infection. In both patients, CT surveillance will be paramount to ensure no recurrent infection occurs with these indolent bacteria.
Conclusion
Thoracoabdominal aortic graft infections are rare. The source is generally gram-positive bacteria but very uncommonly secondary to an anaerobic source. Here, we report the only cases in the literature of thoracic/thoracoabdominal graft infections secondary to Propionibacterium species.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.