
Abstract
Recently, reports have described successful endovascular stent graft (ESG) treatment of patients with acute type A aortic dissection. We report 1 ESG treatment for this condition and the complication of a new aneurysm formation during a 6-month follow-up.
Introduction
Acute type A aortic dissections are life-threatening, and until now, the standard treatment is emergency surgical correction. Although a well-established procedure, it has considerable mortality and complications. Also, conventional surgical procedures may not be indicated in high-risk patients of advanced age, presenting with neurological deficits and multiple comorbidities. Although endovascular stent graft (ESG) repair of descending aortic pathology has promising early and midterm results, similar endovascular repair of the ascending aorta remains a significant challenge due to the anatomical characteristics of this segment of aorta as well as the proximity of coronary ostia and arch branches. Recently, case reports have described successful ESG repair for patients with acute type A aortic dissection, but short and midterm efficacies are unclear. We present a case of ESG treatment of acute type A dissection complicated by new ventricular aneurysm formation at 6-month follow-up.
Case Report
A 73-year-old female was admitted after 10 hours of acute-onset severe chest and back pain. A spiral computed tomography (CT) angiogram confirmed an extensive aortic dissection from the aortic root to the iliac artery. A primary intimal tear in the mid-ascending aorta was evident, and CT revealed a small pleural and pericardial effusion (Figure 1).

Computed tomography (CT) angiography before treatment. Oblique sagittal image (A and B) shows intimal tear (arrow) in the ascending aorta. Three-dimensional (3D) volume-rendered reformatted image (C) shows intimal tear (arrow) at the undersurface of the distal ascending aorta.
Due to the surgical risk of conventional approaches and the patient’s multiple comorbidities (chronic obstructive pulmonary disease, hypertension, and diabetes), the patient refused conventional surgical procedure. The patient had favorable anatomy for an endovascular repair and remained hemodynamically stable and thus was offered treatment with an ESG.
A custom-made stent graft fitting the dimension of the ascending aorta was requested, and the patient was closely monitored for 1 week while the graft was manufactured. Endovascular treatment was performed under general anesthesia. The stent (TBE 38/77 mm; Cook Bjaeverskovk, Denmark) was positioned in the ascending aorta via the right common femoral artery. Before deploying the stent graft, the patient was paced to 180 beats per minute with a temporary ventricular pacemaker placed in the left femoral vein in order to decrease cardiac output and minimize the risk of dislodging the stent graft during surgery.
Completion angiography following stent graft deployment revealed regular perfusion of the coronary arteries, complete exclusion of the dissection, as well as regular perfusion of the supra-aortic vessels and no aortic valve regurgitation (Figure 2). The patient recovered and was discharged 1 week after surgery.
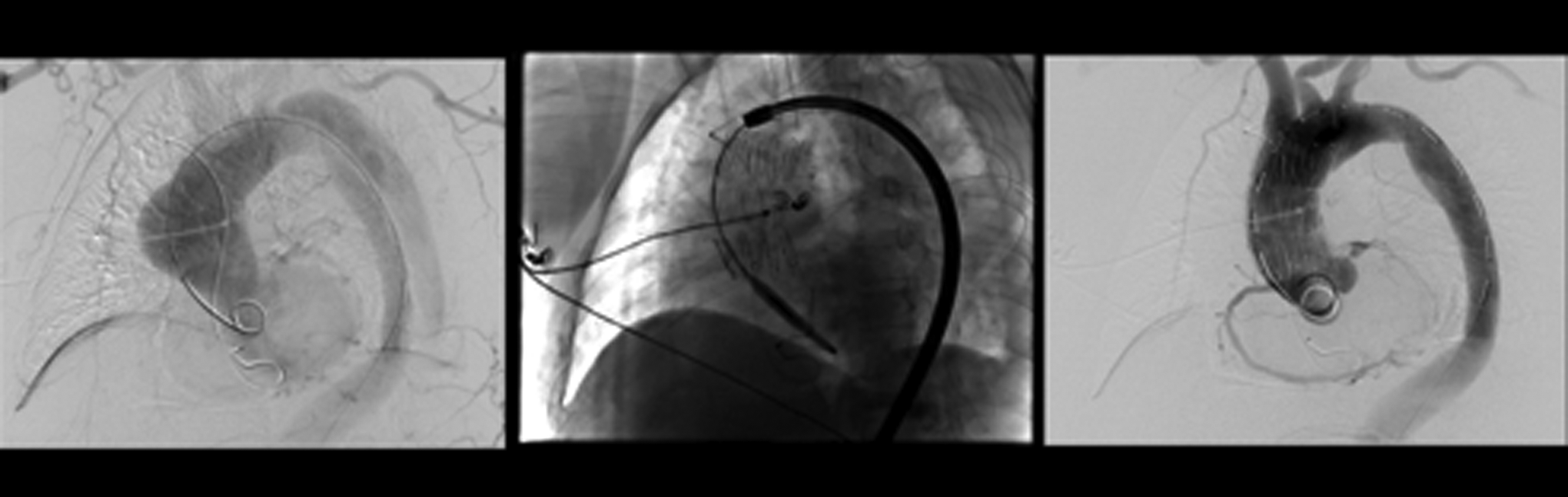
Angiography reveals regular perfusion of the coronary arteries, complete exclusion of the dissection, and regular perfusion of the supra-aortic vessels and aortic valve regurgitation.
One month after stent graft placement, the patient was asymptomatic. Aortic valve competence was confirmed by echocardiography. Computed tomography revealed good position of the graft in the ascending aorta, with regular perfusion of the true lumen and complete thrombosis of the false lumen. Computed tomography angiography also showed an apical left ventricular false aneurysm resembling a long-necked diverticulum (Figure 3).
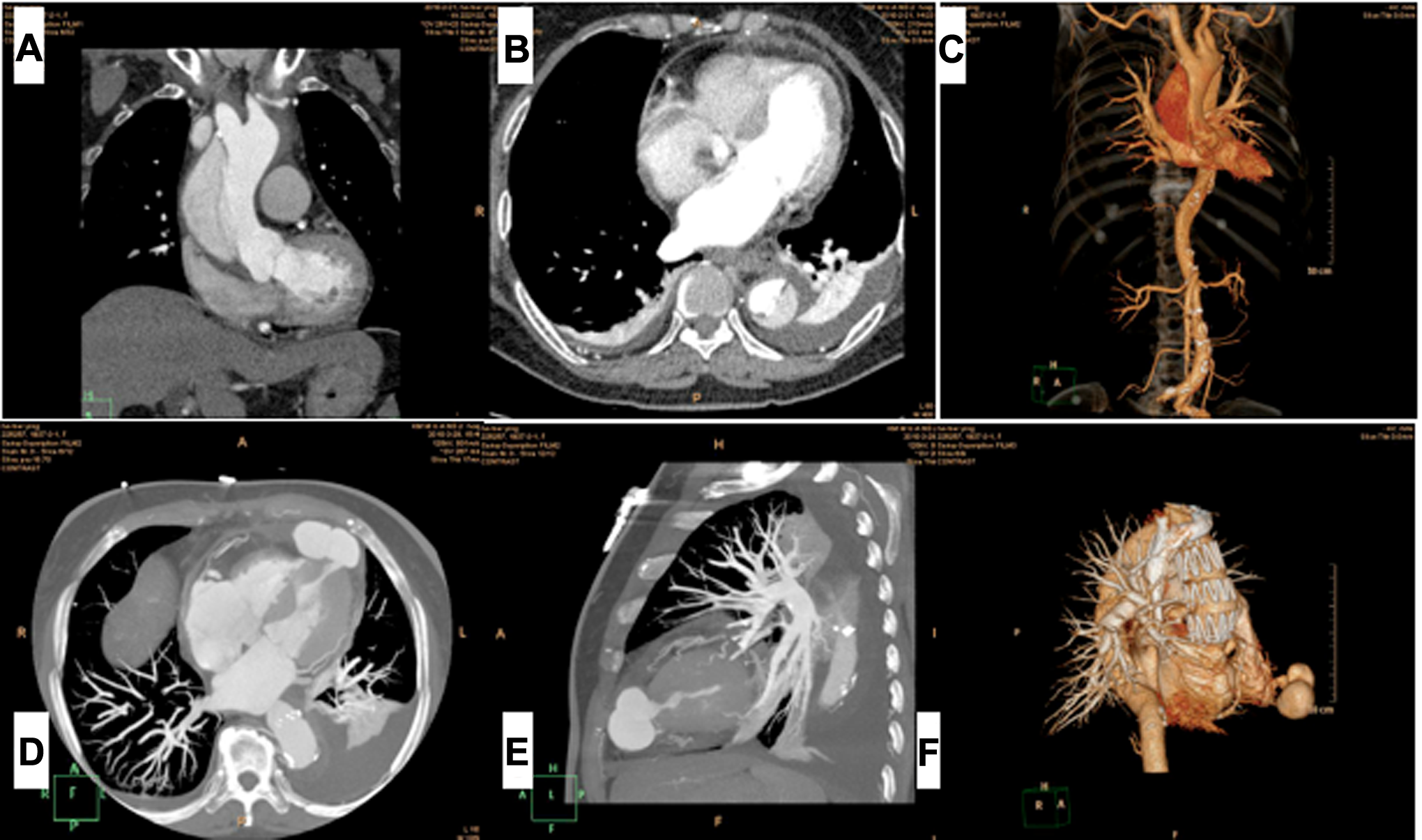
A-C, Preoperative computed tomography (CT) scan shows normal left ventricular false aneurysm. D-F, Postoperative CT scan shows an apical left ventricular false aneurysm.
Six months after the surgery, patient had some occasional chest pain, and transthoracic echocardiography and electrocardiography excluded aortic valve insufficiency and myocardial ischemia. Computed tomography angiography confirmed the same size of the left ventricular false aneurysm as well as a new aneurysm formation at the sinotubular junction (Figure 4). The patient is presently receiving antihypertensive drugs, and aneurysm progression is being closely monitored.
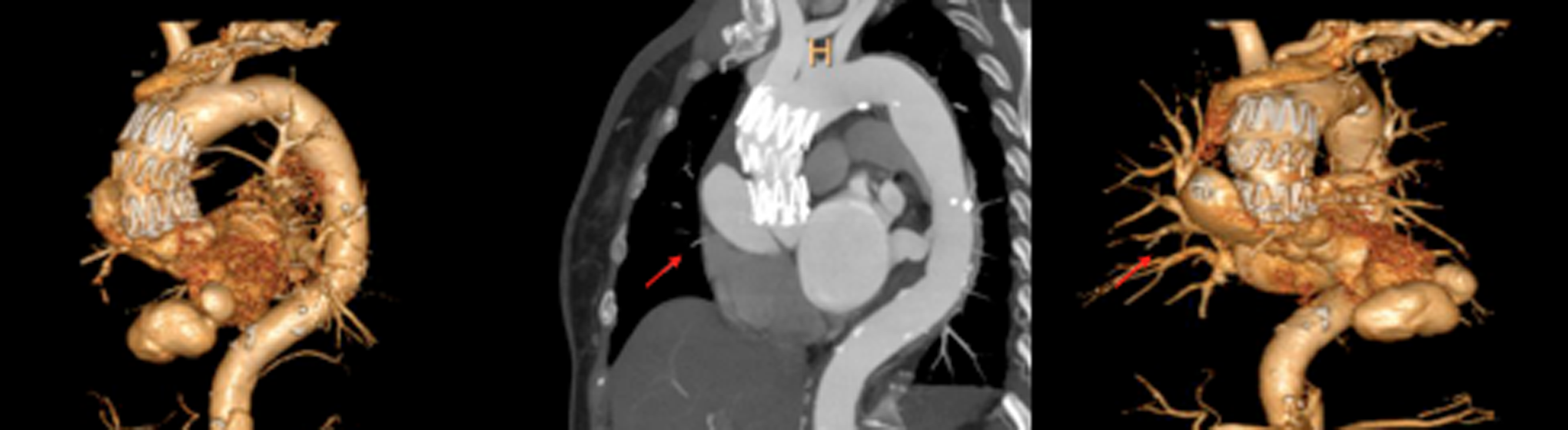
Computed tomography angiography (CTA) shows (arrow) a new aneurysm appeared at the sinotubular junction.
Comments
Acute type A dissection is a life-threatening emergency with high mortality if left untreated. Nevertheless, in high-risk patients (elderly, those with comorbidities, etc), conventional surgery carries a high perioperative mortality. 1 An endovascular approach would appear to be an attractive alternative to open surgery in select high-risk patients who may benefit from a less invasive approach.
In the last decade, ESGs have been increasingly used to treat complicated type B aortic dissections, and intermediate results have been favorable. 2 In addition, ESG has been reported for the treatment of acute type A dissection, 3 –5 although broader application of this technique and the durability of stent graft repair remain to be proven.
Endovascular stent graft of the ascending aorta is technically challenging due to the unique anatomy of the ascending aorta, the proximity of critical structures such as coronary ostia, the brachiocephalic trunk, and the aortic valve. Thus, ESG is limited to patients with uncompromised aortic valve function or an entry tear well above the coronary ostia, sufficiently far from the supra-aortic vessels. Moreover, advanced technical skill is needed to correctly place the stent.
Here, we report successful technical result using ESG to treat an acute type A dissection. Completion angiography demonstrated complete coverage of the primary tear, patent coronary arteries, and great vessels, as well as preservation of normal aortic valve function. Computed tomography imaging obtained at 1 month showed the stent graft in excellent position with no migration and complete false lumen thrombosis. Unfortunately, despite an excellent result, the patient developed pseudoaneurysms of the apical left ventricular at 1 month and a second pseudoaneurysm at the sinotubular junction above the right coronary sinus at 6-month postprocedure.
Currently available ESG devices are designed for use in the descending aorta. When delivering these devices to the ascending aorta, the stiff guide wire must be pushed into the left ventricle with force in order to stabilize it. The nose cone of the delivery system will also be pushed into the left ventricle during deployment. This can result in left ventricular iatrogenic injuries and lead to left ventricular false aneurysm formation after ESG procedure as evident in our case. In particular, the greater hydraulic shear stress in the right lateral wall of the ascending aorta 6 may predispose this section of the aorta to new aneurysm formation just above the right coronary sinus.
In conclusion, the use of currently available endovascular aortic stent grafts designed for treating descending aortic pathology may not be applicable to the treatment of ascending aortic disease in all cases and should be used with caution. Further study and new device designs are needed specific to the ascending aorta.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.