
Abstract
Immunoglobulin (Ig) G4-related disease is reportedly among the various causes of inflammatory abdominal aortic aneurysm (IAAA). Many IgG4-related diseases are closely related to allergic constitution and autoimmune disease. We report a case of a 72-year-old man with IgG4-related IAAA associated with myasthenia gravis, with contained rupture.
Introduction
Since Hamano et al reported immunoglobulin (Ig) G4-related autoimmune pancreatitis 1 in 2001, interest in IgG4-related disease has increased. Moreover, interest in IgG4-related periaortitis has been ongoing since idiopathic retroperitoneal fibrosis was studied in detail. Recently, IgG4-related inflammatory abdominal aortic aneurysm (IAAA) was reported to be one of the IgG4-related diseases; it can be grouped with IgG4-related periaortitis and retroperitoneal fibrosis. 2 Many IgG4-related diseases are closely related to allergic constitution and autoimmune diseases. We recently reported IgG4-related IAAA associated with myasthenia gravis (MG), with contained rupture.
Case Report
Consent was obtained from the family of the patient. A 72-year-old man with a history of hypertension and MG was referred to the emergency department, complaining of flank pain. He had been diagnosed with generalized MG 7 months before, with muscle fatigue and ptosis. He was followed by the neurology clinic and took oral prednisolone 20 mg, pyridostigmine 180 mg, and tacrolimus 3 mg daily for 6 months, with general symptom improvement.
A retroperitoneal inflammation was found with suspicion of retroperitoneal abscess on the basis of computed tomography (CT), and antibiotic treatment was started (Figure 1A). Despite intravenous ciprofloxacin and ceftriaxone for 3 weeks, symptoms were unimproved. In the third week of hospitalization, abdominal pain worsened and follow-up CT showed an IAAA with contained rupture (Figure 1B) with hydroureter due to adjacent adhesion (Figure 1C). He was in a shock state with systolic blood pressure of about 80 mm Hg. He was referred to the vascular surgery department and was diagnosed with a symptomatic aneurysm with contained rupture, requiring emergency surgery. Preoperative laboratory tests showed a white blood cell count of 13 140/µL, C-reactive protein (CRP) of 16.83 mg/L (reference range <5 mg/L), and erythrocyte sedimentation rate (ESR) of 15 mm/h (reference range <15 mm/h). The IgG level was 1612 mg/dL (reference range 700-1600 mg/dL). Immunoglobulin subclass testing revealed elevated IgG4 at 160 mg/dL (reference range 3.9-86 mg/dL). Test results for antinuclear antibody were positive and for antineutrophil cytoplasmic antibody and syphilis antibody cascades were negative.
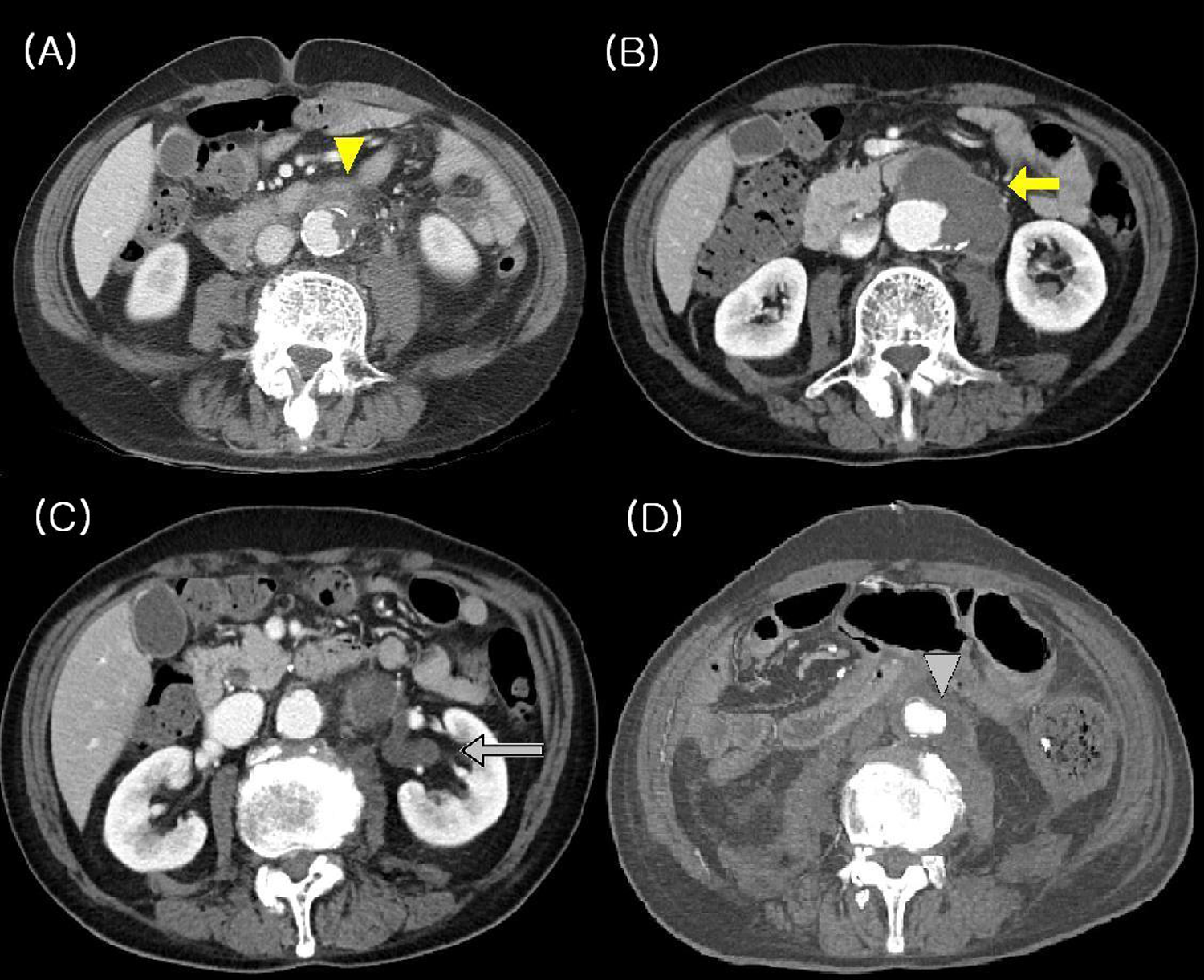
Computed tomography scans on admission, at operation, and after operation. A, Periaortic inflammation (yellow triangle) on admission. B, Aortic aneurysm with contained rupture (yellow arrow) at operation after 3 weeks. C, Hydroureter due to adjacent adhesion (gray arrow) at operation. D, Decreased periaortic inflammation (gray triangle) after operation.
Abdominal laparotomy with transperitoneal approach revealed a huge aortic aneurysm with periaortic fibrosis and hematoma near the left periaortic space and left iliac artery (Figure 2A). The proximal aortic clamping was done below the renal arteries and the left renal vein was ligated for exposure of aortic aneurysm. The left common iliac artery could not be dissected free because of severe fibrosis (Figure 2B). Aneurysmal resection and Y-graft interposition were performed, with a total blood loss of 1000 mL and blood transfusion of 800 mL. Limb anastomoses with a Y-graft were performed in the right common iliac artery for the right limb and in the left common femoral artery for the left limb. The operative time was 420 minutes. The results of culture from aneurysmal tissue and perianeurysmal fibrosis were negative. The postoperative CT scan showed decreased retroperitoneal fibrosis (Figure 2D). Two days postoperatively, critical right limb ischemia due to thrombotic occlusion of the right limb graft was noted. A new bypass from the right limb graft to the right common femoral artery was performed, with thrombectomy of the limb graft.
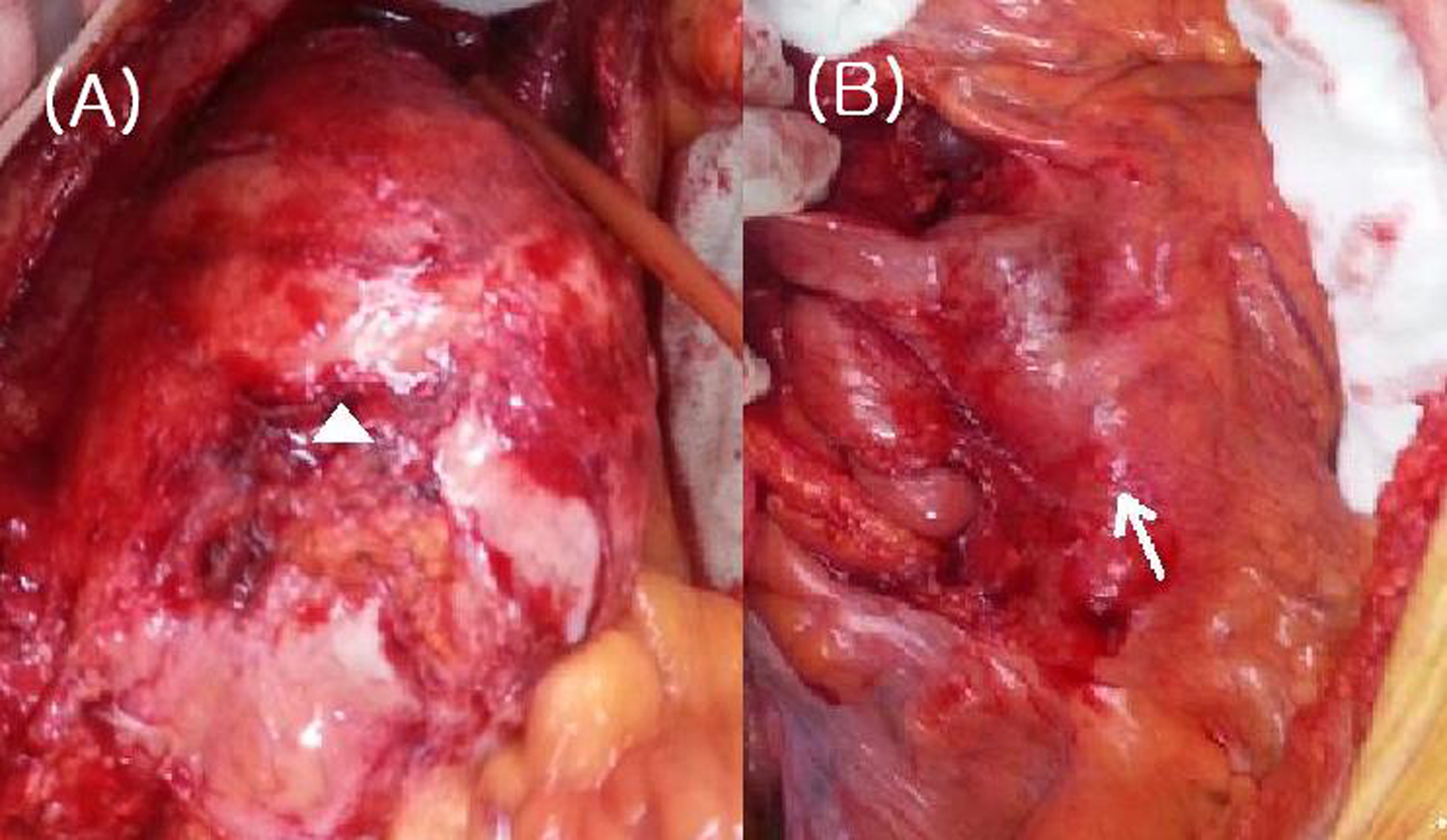
Operative finding of aortic aneurysm. A, Huge aortic aneurysm with periaortic inflammation (white arrow) and contained rupture. B, Fibrosis around the left iliac artery (white arrow).
Over the next 3 months, the patient had recurrent pneumonia and acute renal failure. Peripheral arterial circulation was maintained relatively well. The patient died 3 months after surgery due to adult respiratory distress syndrome with pneumonia.
Discussion
Inflammatory abdominal aortic aneurysm reportedly accounts for 2% to 10% of all cases of AAA. 3 Some reports suggested that IAAA represents secondary change in an atherosclerotic aneurysm. 4 Other reports suggested a relationship between IAAA and autoimmune diseases. 5 Recently, Kasashima et al reported that IAAA is partly related to IgG4-related diseases. 6 Immunoglobulin G4-related IAAA could be grouped with IgG4-related periaortitis and retroperitoneal fibrosis. 2
Clinical Characteristics of IgG4-Related IAAA
Compared to non-IgG4-related IAAA, IgG4-related IAAA frequently shows inflammatory clinical findings, such as fever, high CRP, and leukocytosis. However, the incidence of aneurysm rupture in IgG4-related IAAA is reportedly low because of wall thickening and adhesion to the surrounding tissue. 6 The IAAA makes operative dissection difficult, and this difficult operation may lead to fatal complications. 7 Similarly, in this case, left iliac artery dissections were impossible because of inflammation and fibrosis (Figure 2B). A high serum IgG4 level is the most important factor in the diagnosis of IgG4-related IAAA, and serum IgE elevation is characteristic of IgG4-related IAAA. 6
In this case, unlike infected aneurysm, negative blood culture result, mild elevated CRP, normal ESR, no fever, and no periaortic fluid collection shown on CT scan can be seen as characteristics of IAAA. However, it was not easy to perform endovascular repair with suspected infected AAA. Because operation was started in a shock state and continued to show shock condition during operation, native conduits including a homograft and a neoaortoiliac system could not be used and instead artificial graft was used. Recently, there are reports showing satisfactory results in performing EVAR as a bridge or as a definitive procedure in infected AAA. 8 In this case also, although suspected of infected AAA, considering the patient’s state of shock, performing EVAR first, then considering anatomical bypass with native conduit or extra-anatomical bypass might have been a good strategy.
There are few reports on ruptured IgG4-related IAAA. One case was recently reported by Qian et al. 9 Preoperative steroid therapy might be useful to reduce retroperitoneal fibrous adhesions, but Satomi et al stated that the risk of aneurysmal rupture might be elevated by thinning of the adventitia during steroid therapy. 6 In this case, IgG4 periaortitis progressed to IAAA, despite long-term steroid therapy.
Association Between IgG4-Related IAAA and Allergic Constitution
Interestingly, patients with IgG4-related IAAA frequently have an allergic constitution, with drug allergy, bronchial asthma history, and autoimmune diseases, including rheumatoid arthritis, idiopathic thrombocytopenic purpura, Sjögren disease, and antiphospholipid antibody syndrome. 6 Kasashima et al reported that more than 30% of patients with IgG4-related IAAA have bronchial asthma. 6 Other reports showed that IgG4-related IAAA was related to autoimmune pancreatitis 10 and lymphadenitis. 11
Myasthenia Gravis
Myasthenia gravis is an autoimmune disease characterized by muscle weakness due to neuromuscular junction damage by antiacetylcholine receptor autoantibodies and complement activation. 12 This is the first report of IgG4-related IAAA associated with MG. In experimental models of MG, complement activation by isotypes such as IgG2 played a crucial role. 13 In a mouse study on MG, disease severity was related to the levels of IgG4 against postsynaptic transmembrane proteins. 14 The role of MG in aortic disease should be studied further.
Conclusion
Immunoglobulin G4-related IAAA is one of the IgG4-related diseases. With steroid therapy, IgG4-related IAAA could progress to contained rupture in a short time. We reported IgG4-related IAAA associated with MG, with contained rupture. For selected patients affected by IgG4-related IAAA with impending rupture, an endovascular approach can be considered as a bridge or as a definitive therapy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.