
Abstract
Objective:
We describe a novel approach for the endovascular treatment of femoral artery occlusion as a result of Angio-Seal closure device deployment.
Background:
Angio-Seal is the most commonly used vascular closure device following percutaneous coronary and peripheral catheterizations worldwide. A rare complication of Angio-Seal deployment is an occlusion of the femoral artery leading to limb ischemia requiring revascularization. Given its unique ability to cut both atherosclerotic plaque and the Angio-Seal anchor with a collagen plug at operator-directed planes, TurboHawk/HawkOne atherectomy device can be a fast and effective approach to treat Angio-Seal-associated femoral artery occlusions.
Methods:
We studied 13 consecutive patients who developed Angio-Seal-associated femoral artery occlusions that occurred from 3 hours to several weeks after catheterization. These patients were successfully treated with TurboHawk/HawkOne directional atherectomy followed by balloon angioplasty with no complications. During a mean follow-up period of 20.4 ± 17.3 months, 12 patients remained claudication free with no evidence of obstructive arterial disease of the treated segment on imaging studies. One patient developed restenosis that was treated with repeat atherectomy and balloon angioplasty following which he was asymptomatic at follow-up.
Conclusion:
The use of directional atherectomy followed by balloon angioplasty is a quick, safe, and effective endovascular approach to treating Angio-Seal-associated femoral artery occlusions. It is associated with an excellent success rate, no complications, and good midterm outcomes.
Introduction
The femoral artery remains the most widely used vascular access site for coronary and peripheral interventions with hemostasis achieved using manual compression or closure devices. In the current interventional era, vascular closure devices (VCDs) have become very popular because of their faster rate of hemostasis, leading to a shorter duration of hospital stay and earlier ambulation compared to manual compression alone. 1 –3 However, it is well known that, in rare cases, VCDs may lead to serious vascular complications such as total femoral artery occlusion and acute limb ischemia. Angio-Seal (St Jude Medical, St Paul, Minnesota) is one of the most widely used collagen-plug VCDs for closure of the femoral artery. 1,3 The reported incidence of significant femoral artery stenosis or occlusion with the Angio-Seal device is up to 0.6%. 4 –7 These patients often present with acute severe limb ischemia in the immediate postprocedure period requiring urgent revascularization. However, some patients may present later with evidence of significant lifestyle-limiting claudication.
Traditional approaches to treating this rare but serious complication have involved surgical exploration and resection, but this approach has an associated increased morbidity. 8,9
Directional atherectomy using TurboHawk/HawkOne (Medtronic, Minneapolis, Minnesota) has been successfully used for endovascular excision and removal of atherosclerotic plaque in peripheral arteries for many years. This device can cut plaque in planes dictated by the operator, making it an effective modality to excise and remove large amounts of plaque. Given these unique properties of the device, we hypothesized that it could be used successfully in the removal of the Angio-Seal plug that is obstructing the arterial lumen. We previously reported 4 cases of this treatment approach for Angio-Seal-associated femoral artery occlusion showing good acute result and midterm patency. 10 We adopted this approach in our laboratory as a treatment option for this complication and now present the results of our procedural success rate and prolonged follow-up.
Materials and Methods
In our database, between 2010 and 2015, we identified 13 consecutive patients who presented with acute limb ischemia immediately postprocedure or later with symptoms of claudication of the Angio-Seal-treated limb. In all cases, prior to Angio-Seal deployment, angiography of the puncture site was performed and the device was used only when there were no contraindications present for its use. When symptoms occurred, a significant obstruction of the common femoral artery (CFA) at the Angio-Seal site was confirmed prior to revascularization either by angiography or by arterial Duplex. Endovascular treatment of Angio-Seal-related femoral artery obstruction was performed using the following protocol—contralateral access was used in all patients, 7F 45 cm sheath was advanced with the tip positioned in the external iliac artery of the affected limb. The lesion was crossed and an embolic protection device (usually SpiderFX filter; Covidien, Plymouth, Minnesota) was deployed for distal protection. Directional atherectomy with the TurboHawk/Hawk One device was then performed, with the goal of maximal debulking of the obstructive lesion. After atherectomy, an angiogram was performed to evaluate the effect of treatment and possible complications. If no complications noted, the lesion was then dilated with the balloon using the 1:1 balloon to artery ratio and kept inflated for at least 1 minute at nominal pressure. A treatment goal was to achieve <30% of residual stenosis at the treated segment. The usual follow-up schedule for treated patients was as follows: within 2 weeks, 3 months, 6 months, and 1 year postprocedure and then, if asymptomatic, every 6 months. During every visit, clinical evaluation (Rutherford clinical category) and physical examination were performed. In addition, ankle–brachial index (ABI)/pulse volume recording (PVR) or arterial Duplex was performed to evaluate the patency of the treated artery. Representative case studies are described below:
Case 1
A 53-year-old female with a history of hypertension, hyperlipidemia, coronary artery disease, diabetes, and peripheral vascular disease underwent lower extremity angiography via right CFA access and was found to have chronic total occlusion (CTO) of bilateral superficial femoral arteries (SFAs). She then underwent successful percutaneous angioplasty and stenting of the left SFAs total occlusion. The right CFA vascular access site had no angiographically significant disease prior to Angio-Seal deployment (Figure 1A). Hemostasis of the right femoral arteriotomy site was obtained with Angio-Seal. Four hours following the procedure, she developed right leg numbness and tingling. Physical examination revealed nonpalpable right pedal pulses and weak Doppler signal. The patient was taken back to the catheterization laboratory. Left CFA access was obtained and iliofemoral angiogram was performed via a pigtail catheter positioned in the distal aorta. It revealed a hazy lesion in the right CFA. A 7F, 45 cm sheath was advanced into the right CFA. Selective angiography of the right leg revealed a new severe and hazy occlusion at the prior access site in the right CFA (Figure 1B). Since she had a right mid-SFAs CTO, we advanced a SpiderFX filter (Covidien) into the profunda for embolic protection. Then a TurboHawk LSM atherectomy catheter (Covidien) was advanced to the proximal edge of the lesion and directional atherectomy was performed with 12 passes at operator-directed planes. Finally, the lesion was treated with a 6.0 × 40 mm2 balloon that was inflated to 4 atm. There was a minimal residual haziness, with no significant stenosis at the end of procedure (Figure 1C). Her numbness and tingling resolved at the end of the case. Examination of the atherectomy debris from TurboHawk nosecone and SpiderFX revealed pieces of Angio-Seal collagen plug, suture material, and atherosclerotic plaque (Figure 1E). Specifically, the suture material was found in the SpiderFX, which we assume was introduced into the artery during Angio-Seal deployment and was cut off from the arterial wall by TurboHawk. Nine months later, when she presented for treatment of left SFAs restenosis, repeat angiography revealed a patent right CFA with mild stenosis at the site of the previously treated segment (Figure 1D). Thirty-six months later, she had a patent right CFA on repeated angiography.
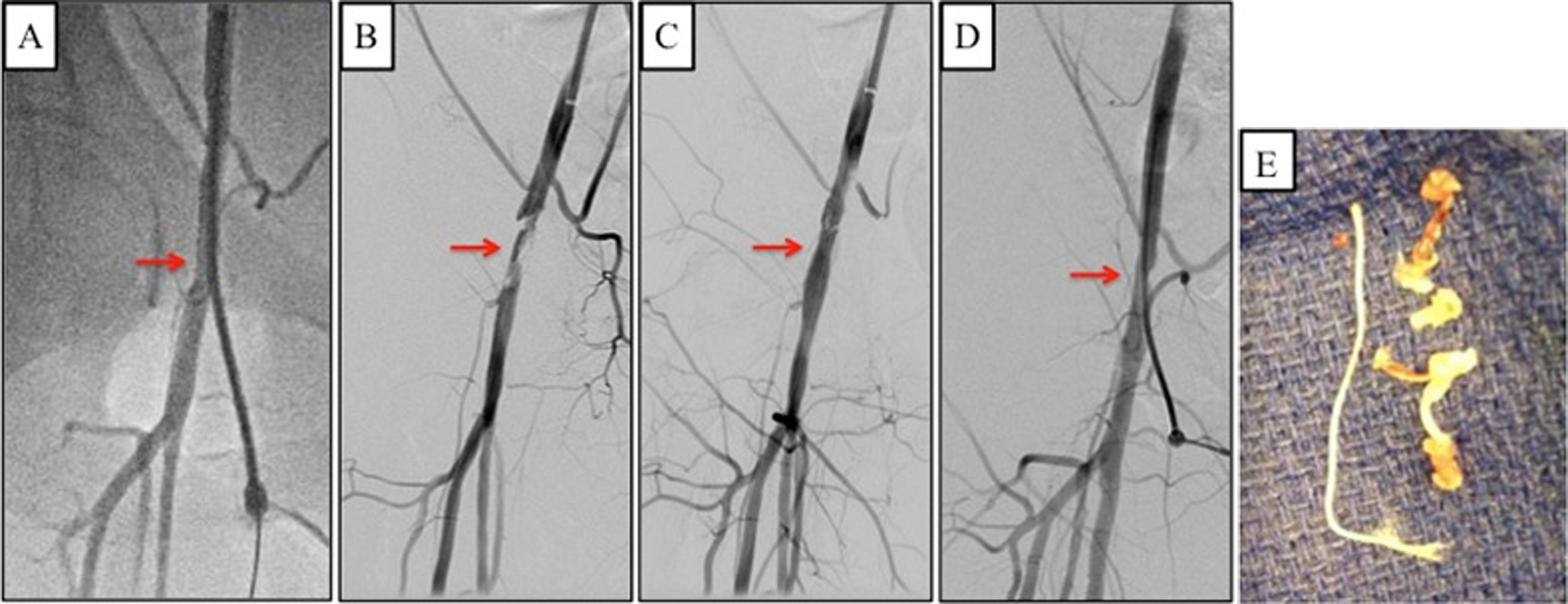
A, Patent sheath insertion site (red arrow), prior to Angio-Seal deployment. B, A new occlusion at the prior sheath insertion site (red arrow), several hours later. C, Minimal residual stenosis following treatment with directional atherectomy and angioplasty. D, Treated area remains patent several months later on repeat angiography. E, Angio-Seal collagen plug, suture material, and atherosclerotic plaque retrieved from the atherectomy device.
Case 2
An 83-year-old male with a history of hypertension, hyperlipidemia, and peripheral vascular disease underwent percutaneous laser atherectomy and angioplasty of a right SFA in-stent restenosis via left CFA access which was angiographically normal prior to Angio-Seal deployment (Figure 2A). Hemostasis was obtained with Angio-Seal. Twelve days following the procedure, he developed severe left leg claudication. Ankle–brachial index and PVR testing showed left leg obstructive peripheral artery disease. He was taken to the catheterization laboratory. Nonselective angiography revealed a total occlusion of the left CFA at the site of previous access (Figure 2B). A 7F sheath was then advanced with the tip positioned in the left external iliac artery, and a 7 mm SpiderFX filter was placed in the distal left SFAs for distal protection. Angiography of the left CFA after that showed a small channel through the lesion (Figure 2C). A TurboHawk atherectomy catheter was advanced over a wire (Figure 2D) and atherectomy was performed. Then a 7.0 × 40 mm balloon was advanced across the lesion and inflated to 3 atm. There was an excellent angiographic result (Figure 2E) at the conclusion of procedure. When the SpiderFX was removed, there was macro debris in the filter (Figure 3A). After the procedure, the patient’s claudication symptoms resolved completely. At 6-month follow-up, the patient presented with symptoms of intermittent claudication and abnormal ABI/PVR. Repeat intervention with atherectomy and balloon angioplasty was performed. Twenty-four months post reintervention, he was symptom free with a normal ABI and PVR.
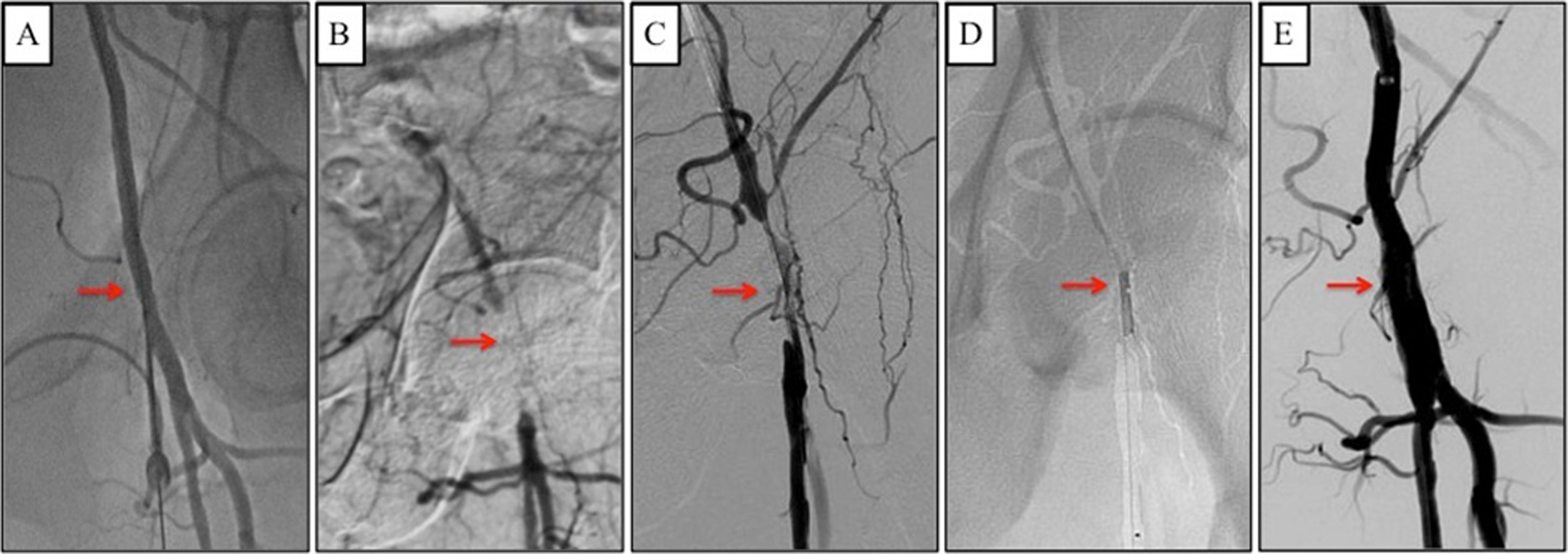
A, Patent sheath insertion site (red arrow), prior to Angio-Seal deployment. B, New chronic total occlusion at the prior sheath insertion site (red arrow). C, Lesion crossed by a guidewire. D, Treatment of occlusion with a TurboHawk directional atherectomy catheter. E, Treated area at the conclusion of the procedure

A, SpiderFX filter with macro debris.
Case 3
A 70-year-old female with a history of hypertension, hyperlipidemia, coronary artery disease, stable angina, and evidence of ischemia on a stress test underwent percutaneous coronary intervention via right femoral access. Prior to Angio-Seal deployment, the right CFA was angiographically normal (Figure 4A). Hemostasis was obtained with Angio-Seal. One week following the procedure, she developed right lower extremity claudication but did not seek medical attention. Seven weeks later, she presented to her cardiologist with chest pain and was referred for urgent coronary angiography to rule out potential stent thrombosis. When she presented to the catheterization laboratory, she reported “new” right leg claudication symptoms.
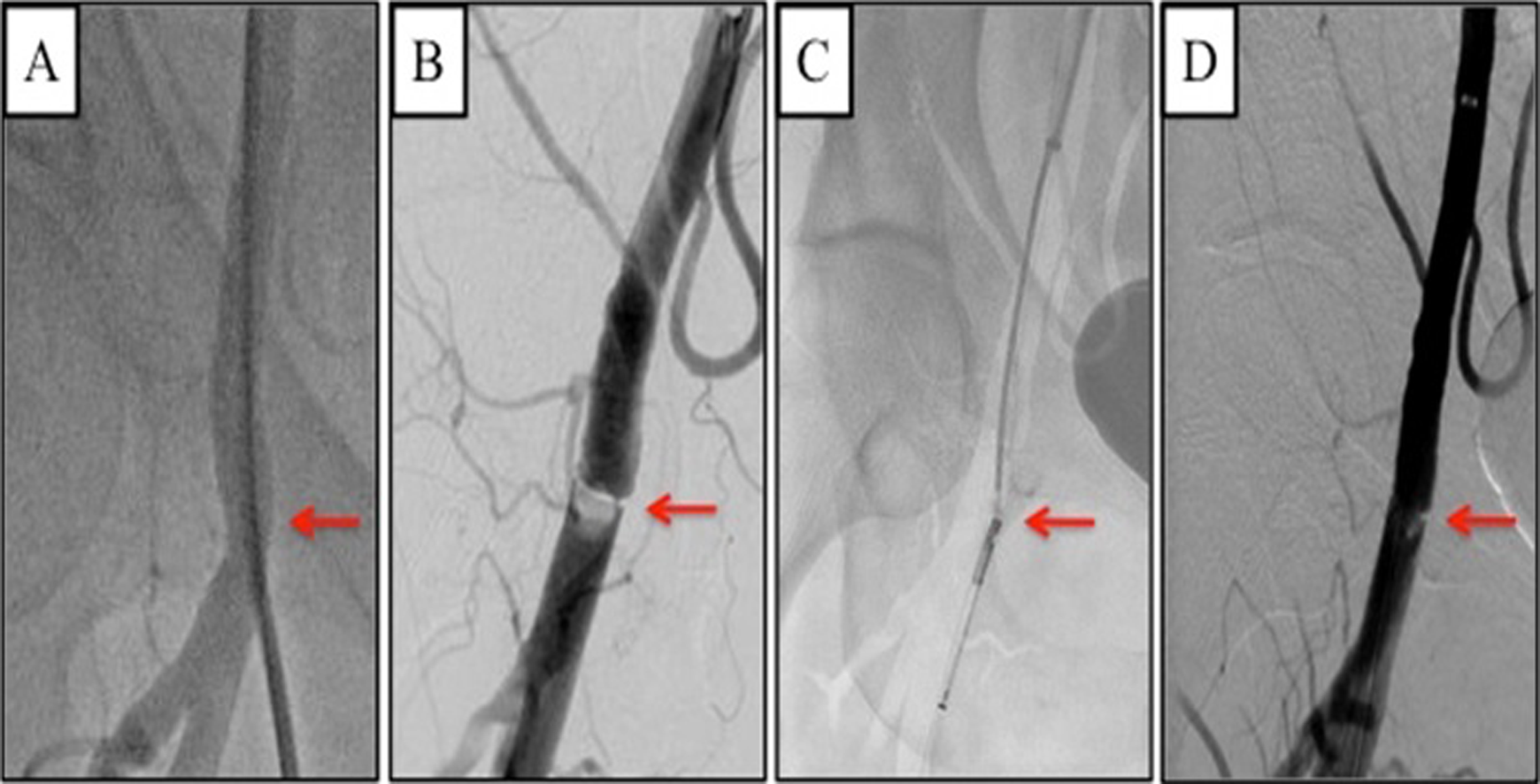
A, Patent sheath insertion site (red arrow), prior to Angio-Seal deployment. B, A new occlusion at the prior sheath insertion site (red arrow). C, Treatment of occlusion with directional atherectomy catheter. D, Minimal residual stenosis following treatment with directional atherectomy and angioplasty.
Left CFA access was obtained, and cardiac catheterization was performed, which revealed patent stents with no significant change compared to her prior angiography. Then right lower extremity angiography was performed, which demonstrated a focal obstructive linear lesion at the prior access site (Figure 4B). A 7 mm SpiderFX filter was advanced to the right SFAs for embolic protection. A TurboHawk atherectomy catheter was advanced to the proximal edge of the right CFA lesion (Figure 4C). The lesion was initially treated with 5 passes of the atherectomy device. Then a 6.0 × 20 mm balloon was advanced across the lesion and inflated to 8 atm. There was a good angiographic result with small residual plaque remaining at the treatment site (Figure 4D). Her claudication symptoms completely resolved, and she was asymptomatic at follow-up in 32 months.
In addition, we had 10 similar cases that were successfully treated using the same protocol as described in the cases above.
Results
During the study period of 5 years (2010-2015), 13 860 Angio-Seal devices were used in our cardiac catheterization laboratory and only 13 patients developed significant Angio-Seal-related femoral artery obstruction requiring revascularization, yielding an incidence of 0.09%, which is lower than 0.6% reported by Steinkamp et al. 6 These 13 patients underwent percutaneous peripheral or coronary angiography/interventions via femoral access followed by deployment of an Angio-Seal device for hemostasis. None of them had contraindications for Angio-Seal use. The baseline characteristics are as outlined in Table 1. Three (23%) patients developed symptoms of acute limb ischemia within 1 day of the index procedure, 5 (38.5%) developed severe claudication within 1 month, and another 5 (38.5%) between 1 and 3 months postprocedure.
Demographic and Clinical Characteristics.
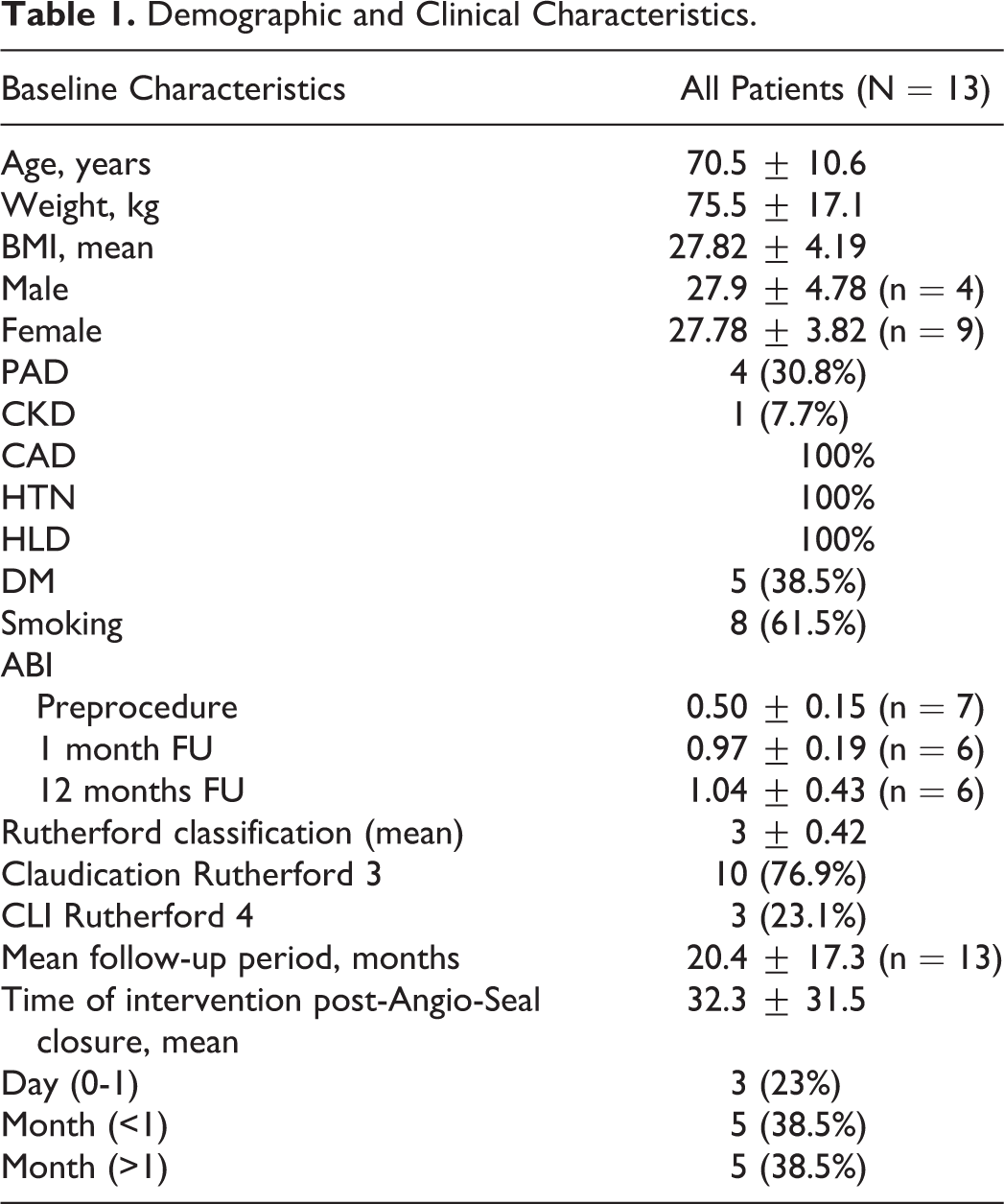
In all patients, selective femoral angiography was performed that revealed severe stenosis in 7 patients (53.8%) and total occlusion in 6 (46.2%) at the prior Angio-Seal deployment site. All lesions were successfully treated with TurboHawk/HawkOne directional atherectomy per the protocol described above with no complications. Macroembolic debris in the filter was seen in 3 (23%) patients. The mean procedure time was 59.7 ± 21.4 minutes. All patients were discharged within 24 hours and followed up closely in our clinic. During a mean follow-up period of 20.4 ± 17.3 months, 12 patients remained free from claudication with no evidence of obstructive arterial disease of the treated arterial segment on vascular imaging studies. One patient presented with symptoms of intermittent claudication and abnormal ABI/PVR at 6 months follow-up. Reintervention with atherectomy and balloon angioplasty was performed successfully. This patient remained asymptomatic after the procedure with normal ABI and PVR at 12 and 24 months follow-up. Therefore, in our cohort the restenosis rate was 7.7%, with excellent secondary patency of 100%.
Discussion
The Angio-Seal device is widely used for hemostasis with a favorable safety profile in the indicated common femoral arteriotomy sites compared to a variety of VCDs in contemporary practice. 11 Rarely despite precautions, there is a possibility for serious vascular complications even in “healthy” femoral arteries, given the structure of the Angio-Seal device that consists of endovascular and extravascular components. The structure consists of a suture that connects a bovine collagen plug and a polymer anchor made of polylactic and polyglycolic acid. 1,8 During Angio-Seal deployment, the polymer anchor is positioned in the intravascular space, and the collagen plug is positioned in the extravascular space. After Angio-Seal deployment, femoral artery occlusion can occur as a result of anchor deployment into a small vessel, anchor deployment into a diseased vessel, or inadvertent collagen plug deployment into the intravascular space. 1,11,12 Femoral artery occlusion may potentially lead to severe limb ischemia and, if not addressed urgently, limb amputation. 12 To minimize vascular complications, the American Heart Association (AHA) provides a class I recommendation on obtaining a femoral angiogram, identifying the sheath insertion site and any vessel disease prior to VCD deployment. 2
Historically, this complication was treated using a variety of surgical and percutaneous techniques, including balloon angioplasty, thrombectomy with AngioJet system, laser-assisted angioplasty, extraction with a snare catheter or even with the endomyocardial biopsy device and angioplasty followed by stenting. 5,6,10
We hypothesized that given the unique properties of the TurboHawk/Hawk One atherectomy device, combination of directional atherectomy with balloon angioplasty could be a new paradigm for the treatment of Angio-Seal-related femoral artery obstruction. The debulking ability of the TurboHawk and HawkOne devices, allowing for the removal of the Angio-Seal structure and possible overlaying thrombus, can help restore luminal patency without the need for stenting in the CFA. The TurboHawk and HawkOne devices contain a rotating cutter that can be directed at different planes dictated by the operator. It gives clear visualization of the cutter position during the procedure and enables preferential excision in the direction of the lesion, thus sparing the normal portion of the arterial wall. 10
A nosecone reservoir collects debris distal to the cutter but distal embolization can still occur. Although there is no general consensus on the deployment of an embolic protection device distally prior to atherectomy, we felt that this might be a reasonable approach in the scenario of Angio-Seal-associated occlusion that most likely consists of large burden of thrombus, Angio-Seal anchor, and plug material. All these components increase the likelihood of macroembolization. In all our patients, a SpiderFX filter device was always deployed distally for embolic protection prior to TurboHawk/Hawk One atherectomy. In 3 (23%) of the cases, we observed macrodebris in the filter.
Our study is the first report on acute and midterm (up to 3 years) outcomes of endovascular treatment of Angio-Seal-related vascular complications with directional atherectomy and balloon angioplasty. Previously Thalhammer et al 5 have reported the use of angioplasty with bailout stenting as a modality of endovascular therapy for this complication. However, in their study, 27% of the patients ended up receiving stents in the CFA, which in itself is not an ideal scenario. Our approach is unique in that, there is no stenting required, thereby avoiding the risk of stent fractures (known to occur in the CFA) and preserving future arterial access. A similar approach albeit with laser atherectomy has been demonstrated by Steinkamp et al, 6 where laser-assisted recanalization was performed in 13 of 16 patients but surgical intervention was required in 3 of 16 patients. The durability of this treatment is also uncertain since no long-term follow-up data was reported.
Based on the evidence of Thalhammer et al, 5 Steinkamp et al, 6 and our experience, it can be postulated that surgical intervention for this complication could be avoided, given the excellent results that can be obtained with endovascular therapy. Open vascular surgery is associated with higher morbidity than the endovascular approach for leg ischemia, 13 especially with regard to bleeding complications, since a majority of patients are treated with dual antiplatelet therapy. Additionally, complications of surgery in the groin area such as lymphatic fistulas, infections, and delayed wound healing might also occur.
Although Angio-Seal complications most commonly occur within a few hours postprocedure, it may occur as late as 3 months after device deployment. 14 Five of our patients developed symptoms of intermittent claudication more than 1 month following the index procedure. In a case report, Wille et al describe a patient who developed leg ischemia 37 days after Angio-Seal deployment 15 and underwent surgical exploration which revealed an excessive fibrotic reaction from the anchor absorption that lead to obstruction of the femoral artery. This mechanism of stenosis is probably applicable to the 5 cases in our cohort presenting later than 1 month after index procedure. Despite the potentially different mechanism of CFA obstruction in cases with late presentation, our approach was still very successful in restoring and maintaining short-term and midterm vessel patency. All our patients were successfully treated and discharged within 24 hours. During a mean follow-up period of 20.4 ± 17.3 months, 12 patients (92.3%) remained free from claudication with no evidence of obstructive arterial disease of the treated segment on vascular imaging studies. One patient (7.7%) presented with symptoms of intermittent claudication and abnormal ABI/PVR at 6 months follow-up. Reintervention with directional atherectomy and angioplasty was performed again successfully. Twenty-four months post reintervention the patient remained symptom free with a normal ABI and PVR.
A limitation of our study is the small number of patients. It is possible that not all patients with Angio-Seal-related complications were identified, especially those with mild symptoms and not reporting them to their physicians.
Conclusion
Angio-Seal-related complications may present immediately after the procedure or even several weeks later. Given the nature of the Angio-Seal anchor and plug, we propose that TurboHawk/HawkOne directional atherectomy with balloon angioplasty and distal embolic protection is a safe and effective approach to treat Angio-Seal-associated femoral artery occlusions. In our patients, this approach has shown to be associated with high primary and secondary patency rates with no complications. Given these findings, we recommend this approach as a primary therapy for Angio-Seal-related CFA obstruction. In the laboratories with insufficient expertise of directional atherectomy use, other treatment options should be considered.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Authors Dr Babaev and Dr Attubato have received honoraria for physician training courses and consultant fees from Medtronic.