
Abstract
Background:
This was the first prospective study to assess the safety and efficiency of MynxGrip vascular closure device (VCD) in peripheral interventions with antegrade access.
Methods and Results:
We enrolled 66 consecutive patients from 1 center. All patients were discharged home on the day of procedure and were observed for adverse events at 1 and 30 days of follow-up. No major complications were observed. The rate of minor complications (conversion to manual or mechanical compression) was 7.6%. Postdischarge, 3% of patients experienced minor complications—small abscess, ipsilateral deep vein thrombosis. In 1 patient, a second VCD was deployed after device failure. The derived device failure rate was 5.9%. No patients required hospitalization. No late bleeding and no hematomas >6 cm were noted. The mean time to discharge was 4 hours and 5 minutes.
Conclusion:
The MynxGrip was safe and effective in sealing access sites after antegrade femoral artery puncture with same-day discharge.
Introduction
Peripheral artery disease (PAD) is a circulatory problem affecting 8 to 12 million people in the United States. 1 Percutaneous revascularization is the first-line therapy in a majority of patients with chronic lower extremity ischemia. 2 Bleeding from the puncture site and local vascular complications significantly contribute to morbidity 3 and may affect mortality. 4 A recent large randomized trial comparing vascular closure devices (VCDs) to manual compression showed that VCDs were noninferior to manual compression in terms of vascular access site complications and reduced the time to hemostasis. 5 They were also shown to reduce time to ambulation, time to hemostasis, and patient comfort compared to manual compression. 6
There are several techniques for vascular access. 7 In the antegrade femoral technique, the needle is aimed distally for the puncture and the guidewire is passed down in an antegrade fashion. It is widely used 8 and is the standard technique at our institution. This approach provides the ability to use longer sheaths, better catheter support, and easier manipulation of the guidewire. The drawback of this technique is the difficulty to achieve hemostasis using manual compression (especially with puncture of the superficial femoral artery) and possibly a higher complication rate than retrograde puncture. 9,10 It is contraindicated when there is ipsilateral occlusion near the puncture site and when anatomy near the puncture site is unknown. In addition, there are technical factors during antegrade puncture that may affect the use of VCDs such as steep angles of the arteriotomy (especially in obese patients), kinking of the procedural sheath, and vessel calcification. Because of this, the safety and efficiency of VCDs should be established for antegrade puncture before they are routinely used for this indication.
The MynxGrip VCD (Access Closure, Santa Clara, California) is an approved VCD that provides a polyethylene glycol-mediated, extravascular sealing of the puncture site (Figure 1). 11 The MynxGrip delivery catheters utilize a balloon as backstop to locate the arteriotomy and create a temporary hemostasis; subsequently, a telescoping sheath delivers the sealant on top of the arteriotomy in the extravascular space. After sealant deployment, the balloon is deflated and removed through the sealant.

MynxGrip sealant adhering to the vessel wall.
The MynxGrip VCD has not been studied in antegrade puncture. The current study was the first prospective study to assess the safety and efficiency of the MynxGrip VCD after antegrade puncture during diagnostic and interventional procedures utilizing 5F, 6F, and 7F procedural sheaths.
Methods
The MAP trial (MynxGrip for closure of antegrade puncture after peripheral interventions with same-day discharge) was a prospective, single-center, single-arm registry conducted in an outpatient-based facility. Patients undergoing 66 consecutive procedures were enrolled. The follow-up contact was done by phone call or during office visit at 1 day (+3 days) and 30 days (±7 days). The study protocol was approved by Fox Commercial Institutional Review Board, Ltd. (ethics committee reference number: 120605-001), and before enrollment, the patients signed an institutional review board–approved informed consent form (ICF). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
The inclusion criteria for the study were at least 18 years of age, ability to ambulate, and planned peripheral interventional procedure with antegrade puncture technique using a 5F, 6F, or 7F procedural sheath. General exclusion criteria were prior surgical procedure; percutaneous transluminal angioplasty or stent placement in the common femoral artery (CFA); a documented bleeding disorder such as thrombocytopenia (platelet count <100 000/mm3), hemophilia, von Willebrand disease, or anemia (Hemoglobin <10 g/dL, Hematocrit <30%); uncontrolled hypertension (systolic blood pressure >180 mm Hg); body mass index >40 kg/m2; pregnancy or lactation; documented international normalized ratio >1.5 (or receiving glycoprotein IIb/IIIa platelet inhibitors); and known severe allergy to contrast medium or known allergy to polyethylene glycol. Intraprocedural exclusion criteria were diameter of the CFA <5 mm, significant peripheral vascular disease in the vicinity of the puncture site, puncture located above the most inferior border of the inferior epigastric artery or above the inguinal ligament, a posterior puncture or multiple puncture attempts, an ipsilateral venous sheath, preexisting hematoma, brisk oozing, pseudoaneurysm or arteriovenous (AV) fistula, or other intraprocedural findings that in the opinion of the investigator would preclude participation such as difficulty inserting the procedural sheath or very long procedural sheath.
Consecutive patients eligible for peripheral intervention with antegrade puncture between July 2012 and January 2014 were asked to participate in the study. Seventy-four patients have signed the ICF. One patient was excluded due to uncontrolled hypertension and anemia (n = 1). Seven (n = 7) patients were excluded in the periprocedural period for the following reasons—entrapment of the interventional device before closure (n = 2), sheath size other than protocol specified (n = 4), and no intervention attempted (n = 1). No other patients were excluded from the study. Sixty-six patients were included in the final analysis.
The primary safety end point was the occurrence of major complications at 30-day (±7 days) follow-up: access site–related surgical or vascular repair, permanent access site–related nerve injury, access site–related bleeding requiring transfusion, new ipsilateral lower extremity ischemia requiring surgical intervention, access site–related infection requiring hospitalization and/or intravenous (IV) antibiotics, and access site–related inflammatory reaction requiring hospitalization and/or IV antibiotics.
A minor complication was defined as access site hematoma ≥6 cm, pseudoaneurysm resolved with thrombin injection or not requiring treatment, ipsilateral AV fistula, ipsilateral deep vein thrombosis (DVT), ipsilateral lower extremity arterial emboli, late access site–related bleeding (following hospital discharge), transient loss of ipsilateral lower extremity pulse, transient access site–related nerve injury, access site–related vessel laceration, access site wound dehiscence, access site–related infection requiring treatment with oral antibiotics, and local access site inflammatory reaction.
Definitions of major and minor complications followed FDA guidelines and Mynx instructions for use (IFU); these were published by Scheinert et al. 12
Procedure success was defined as successful deployment of the MynxGrip VCD and hemostasis achieved without conversion to manual compression (>10 minutes). The above criteria were used to derive device failure rates (%).
All patients received anticoagulation with bivalirudin per standard protocol at our institution. Because the anatomy of the puncture site was known from previous diagnostic angiography, antegrade puncture was performed without ultrasound guidance. The range of procedures performed were balloon angioplasty, atherectomy, and stenting. Before closure, final angiography of the puncture site was performed to assess suitability for closure. The MynxGrip sealant deployment was used according to the closure protocol provided by the manufacturers. After sealant deployment, operators laid the device down for 60 seconds, then the balloon was deflated, and the device was removed followed by 10 minutes of mild fingertip compression to stabilize the puncture site before transferring the patient to the ward (standard safety protocol in our institution). In situations when a long sheath was used for procedure, the sheath was exchanged before VCD deployment. During follow-up visits, the groin site was assessed and patients were screened for adverse events. The study did not use routine venous and arterial Doppler ultrasound examinations in all patients. Ultrasound and other appropriate studies were performed if the patients presented with symptoms during follow-up visits.
Results
Patient demographics are shown in Table 1. We closed a total of 66 antegrade puncture sites with the MynxGrip VCD. A 6F sheath was used in 53 (80%) of the 66 cases, and a 7F sheath in 13 (20%) of the 66. All patients were discharged home on the day of procedure. No major complications were noted during the follow-up period.
Baseline Characteristics.
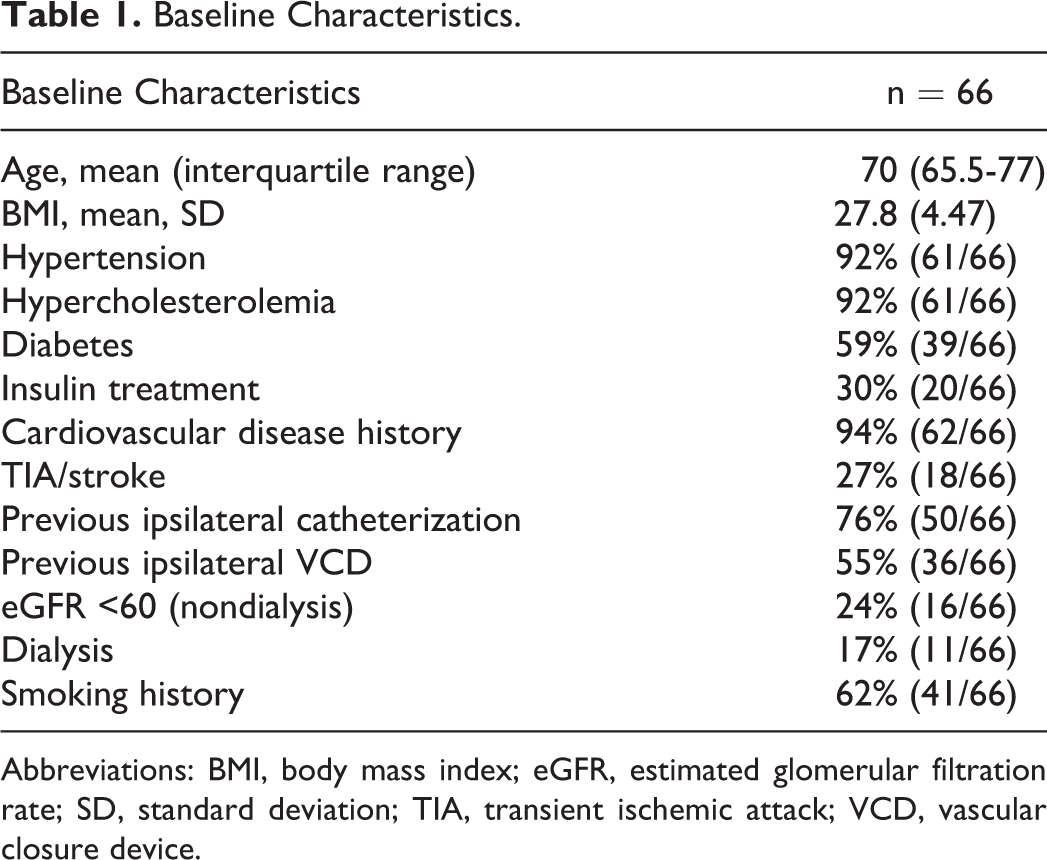
Abbreviations: BMI, body mass index; eGFR, estimated glomerular filtration rate; SD, standard deviation; TIA, transient ischemic attack; VCD, vascular closure device.
The overall procedure success rates were 95% (63 of the 66). In-hospital minor complications were mainly due to device failure leading to conversion to manual compression (30 minutes, n = 1) or mechanical compression (n = 2). In 1 (n = 1) patient, device failure was managed by a successful reattempt to close with a second MynxGrip device. The derived device failure rate was 5.9% (4 of 67 devices). Postdischarge, 2 (3%) of the 66 patients experienced minor complications: 1 patient had a small abscess in the vicinity of the puncture site that was treated with incision and oral antibiotics. Another patient had ipsilateral DVT that was treated with oral anticoagulants. No patients required hospitalization. No late bleeding and no hematomas larger than 6 cm were noted. The mean time to discharge was 4 hours and 54 minutes (range: 1 hour 41 minutes to 7 hours).
Discussion
Most of the data about the safety of VCDs come from studies in coronary procedures and retrograde puncture in case of PAD. Relatively, fewer studies examined the utility of VCDs in the setting of antegrade puncture.
The present study is the first to assess the safety and efficiency of the MynxGrip extra VCD in femoral artery closure after antegrade puncture. The device failure rates were 5.9%, comparable to previous reports. 13
Interestingly, the most widely studied VCD in antegrade puncture is also another extravascular VCD, namely Exoseal (Cordis Corporation, Fremont, California). In a prospective study, Schmelter et al 14 showed a success rate of 96%, pseudoaneurysm in 4% of cases, and recurrent bleeding in 3% of cases. Another prospective study of 59 patients by Maxien et al 15 found a success rate of 98.3%, pseudoaneurysm in 1.7%, and hematoma or secondary bleeding in 5.1%. And finally, a retrospective analysis showed a success rate of 98.8% and 7.2% minor complications. 16
The utility of sandwich-type closure device (Angio-Seal; St Jude Medical, Saint Paul, Minnesota) was assessed in 120 consecutive patients undergoing antegrade puncture in a prospective study. 17 Success rate was 81%, with no minor or major complications. However, this study enrolled every patient eligible for antegrade puncture with no exclusion criteria. In another retrospective series of 58 patients with antegrade puncture, the Angio-Seal VCD was successfully used in 46 of 58 patients, failed in 4, and was not used in 8 due to vessel calcification or other reasons. 18 Three patients in the Angio-Seal group had hematomas and one of them required blood transfusion.
Gutzeit et al reviewed outcomes of femoral closure (antegrade puncture) with suture-mediated (Perclose; Abbott, North Chicago, Illinois) and extravascular clip (StarClose; Abbott) closure devices in a retrospective study (n = 178). The study used ultrasound guidance for the puncture and a pressure dressing for 6 hours postprocedure, and there was no follow-up available after discharge. 19 Success rate was 91%. Vascular complications included hematoma (6.2%), pseudoaneurysm (2.2%), and vascular occlusion (0.5%).
The observed complication rate in this study is relatively low. This might be attributed to the fact that all patients were in stable condition despite having comorbidities and prevalent risk factors (treated in outpatient settings). Also, the use of bivalirudin in all the studied patients would have been a factor as well. 20 Furthermore, the use of additional 10 minutes of fingertip compression after MynxGrip deployment (which is longer than specified by manufacturer’s IFU) may have favorably contributed to closure outcome. Finally, our preexisting experience with the Mynx and new generation MynxGrip with enhanced sealant characteristics 11 may have mitigated additional risks.
There were 2 unusual complications in the current study: 1 DVT and 1 abscess at the puncture site. DVT has been described in association with prolonged compression of the groin following percutaneous catheterization. 21 Furthermore, the IFU or most VCDs state DVT as a potential risk associated with the use of VCDs. Infectious events have been reported to be associated with the use of VCDs. 22
The main limitations of the study are sample size and lack of randomization. Confounders such as operator skill, experience with the device, and choice of anticoagulation therapy were not avoidable. Because the study was conducted in a single outpatient facility and several exclusion criteria were used, the results apply to selected patients undergoing elective procedures and qualified for early discharge. Routine arterial and venous ultrasound examinations were not performed in all patients during follow-up; therefore, some asymptomatic complications may have been missed. However, the current study offered longer follow-up than the majority of other studies of VCDs in antegrade femoral puncture. The value of the present study lies in its novelty of providing a first insight into the utility of the MynxGrip in sealing antegrade femoral artery punctures in the outpatient settings.
Conclusion
We conclude that the use of MynxGrip in sealing antegrade femoral artery punctures appears to be feasible and safe in selected patients undergoing elective peripheral endovascular interventions with same-day discharge.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Access Closure, Inc, Mountain View, CA, USA.