
Abstract
Purpose:
To evaluate the impact of a new angiographic imaging technology on radiation dose during visceral embolization procedures involving both fluoroscopy and digital subtraction angiography.
Material and Methods:
A retrospective analysis from a single-center consecutive series of patients was performed comparing 2 angiographic imaging systems. The AlluraClarity (CIQ; Philips Healthcare, Best, the Netherlands) was used in 100 patients (n = 59 male, mean age: 70.6 years) from July 2013 to April 2014 and compared to the former AlluraXper (AX) technology used in 139 patients (n = 71 male, mean age: 70.1 years) from May 2011 to June 2013. Patients were categorized according to body mass index (BMI [kg/m2])—group 1: BMI <25, group 2: BMI ≥25 and <30, and group 3: BMI ≥30. Fluoroscopy time, the total dose of iodinated contrast administered, and procedural AirKerma (Ka, r [mGy]) were obtained.
Results:
Mean BMI was 26.4 ± 5.0 kg/m2 in the CIQ and 26.4 ± 7.1 kg/m2 in the AX group (P = .93). Fluoroscopy time and the amount of contrast media were equally distributed. Ka, r was 1342.9 mGy versus 2214.8 mGy (P < .001, t test) when comparing CIQ to AX. Comparing CIQ to AX, BMI subgroup analysis revealed a mean Ka, r of 970.1 to 1586.1 mGy (P = .003, t test), 1484.7 to 2170.1 mGy (P = .02, t test), and 1848.8 to 3348.9 mGy (P = .001, t test) in BMI groups 1, 2, and 3, respectively.
Conclusion:
The CIQ technology significantly reduced mean radiation dose by 39.4% for visceral embolization procedures when compared to fluoroscopy time and contrast media dose. This dose relationship was consistent across all BMI groups.
Introduction
A significant number of patients with significant gastrointestinal bleeding can be treated by angiography with selective embolization of the visceral artery branches. However, arterial embolization of visceral arteries requires sophisticated imaging, exposing both operators and patients to high radiation dose. 1 Moreover, in obese patients, an exponential increase in ionizing radiation is required to assure proper image quality. 2 -4 In consequence, concerns have been raised on the radiation exposure of patients and operators, and investigations have been prompted evaluating radiation dose amounts and strategies for possible dose reduction. 5 -8
To address this major concern of radiation exposure, further developments from the imaging technology are required. AlluraClarity (CIQ; Philips Healthcare, Best, the Netherlands) is intended to acquire equivalent image quality as the former AlluraXper system (AX; Philips Healthcare, Best, the Netherlands) but for less radiation. The CIQ has previously shown to significantly reduce radiation dose for various interventional cardiology, interventional (neuro) radiology, and endovascular surgery procedures. 9 -16 Despite the challenges of comparing different imaging technologies within different settings, a direct comparison of CIQ and AX was performed in several studies, showing no significant loss of image quality. 9,13,15,16 However, the CIQ technology is optimized for each specific acquisition protocol. Therefore, the promising results are not necessarily negotiable for all types of procedures and body locations. Inherently, achievable dose reduction for each type of procedure will be different as each requires a specific acquisition protocol.
The purpose of the present study was to evaluate the potential benefit of CIQ toward dose reduction and its impact on the physician working habits in patients undergoing visceral embolization therapy, since this is a subset of procedures known to necessitate high radiation doses. 1,2
Materials and Methods
Patients and Methods
This study evaluated a consecutive series of 239 patients (CIQ: n = 100 [n = 59 male, mean age: 70.6 years], AX: n = 139 [n = 71 male, mean age: 70.1 years]) undergoing visceral embolization therapy at a tertiary referral center. The indication for visceral embolization was related to gastrointestinal bleeding in all patients. Information on patients’ demographics characteristics including weight and height (cm) and differentiated for CIQ and AX is provided in Table 1. Since physical conditions were shown to affect image acquisition and quality, 2 -4 body mass index (BMI [kg/m2]) was evaluated. According to the BMI values, patients were categorized into 3 groups: group 1: BMI <25 kg/m2, group 2: BMI ≥25 to <30 kg/m2, and group 3: BMI ≥30 kg/m2. As outlined in Table 1, there was a homogenous BMI distribution when comparing the CIQ and AX groups.
Patients’ Characteristics and Demographics of 239 Patients Undergoing Visceral Embolization.a
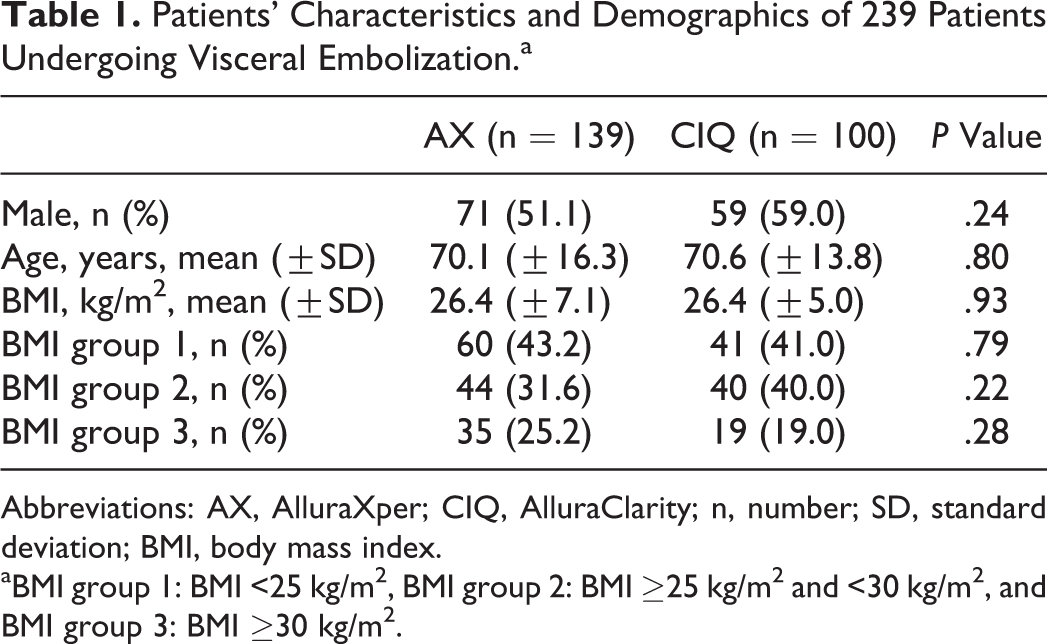
Abbreviations: AX, AlluraXper; CIQ, AlluraClarity; n, number; SD, standard deviation; BMI, body mass index.
aBMI group 1: BMI <25 kg/m2, BMI group 2: BMI ≥25 kg/m2 and <30 kg/m2, and BMI group 3: BMI ≥30 kg/m2.
To estimate the benefit of the novel CIQ technology, radiation dose recordings using CIQ were compared to radiation dose recordings using the former AX technology (control group). The AX measurements were obtained from May 2011 to June 2013 and CIQ measurements after installation in July 2013 from July 2013 until April 2014, respectively. All procedures were performed following the radiation safety principle of As Low As Reasonably Achievable for both imaging technologies. Data collection and analysis were performed retrospectively. In line, the interventionists were not aware that these data are going to be evaluated at the time of procedure. Approval from our institutional review board was obtained including a waiver of informed consent due to the retrospective nature of the evaluation. All data were collected in a Health Insurance Portability and Accountability Act compliant manner.
AlluraClarity Technology and Measurements Obtained
AlluraClarity is intended to acquire the equivalent image quality as AX but for less radiation. This is achieved by an improved real-time image noise reduction algorithm as well as hardware optimization. The algorithm utilizes real-time automatic pixel shift, motion compensation, temporal, and spatial noise reduction to preserve image quality, while associated hardware reconfiguration is intended to reduce the entrance dose by adjusting and optimizing the full acquisition chain for different anatomic regions. 9
For the purpose of comparing the performance of the former AX with the novel CIQ technology, information on fluoroscopy time (minutes), total dose of iodinated contrast, and AirKerma (Ka, r [mGy]) were evaluated. The Ka, r was calculated for the patient entrance reference point which was considered the approximation of the patient’s skin, located in the central X-ray beam and 15 cm from the isocenter toward the focal spot. 17 Fluoroscopy time and contrast usage served as indirect parameters for image quality. Similar amounts of contrast and fluoroscopy time were considered to indicate equivalent image quality when comparing AX and CIQ. However, no direct comparison of image quality was performed.
Statistical Analysis
Categorical variables are presented as number and percentage and are compared using the Fisher exact test. Continuous variables are presented as means ± standard deviation and 95% confidence interval (CI) where appropriate and are compared using an independent t test after checking for homogeneous distribution. This was done for the comparison of the total study and control groups as well as for BMI subgroup analysis. A P value <.05 was considered statistically significant. Statistical calculations were performed using STATA software (STATA Statistics version 14.0, StataCorp, College Station, Texas).
Results
A total of 239 patients were undergoing visceral embolization procedures. As outlined in Table 1, patients did not differ by age, gender distribution, and BMI when comparing the CIQ and AX cohorts. Procedural details are listed in Table 2 showing longer procedure times in CIQ patients (108.3 ± 45.3 minutes vs 91.4 ± 44.0 minute, P = .004, t test). Figure 1 illustrates BMI subgroup analysis showing a difference in the BMI group 2 (117.0 ± 7.1 minutes vs 86.8 ± 5.0 minutes, P < .001, t test).
Procedural Details of 239 Patients Undergoing Visceral Embolization.
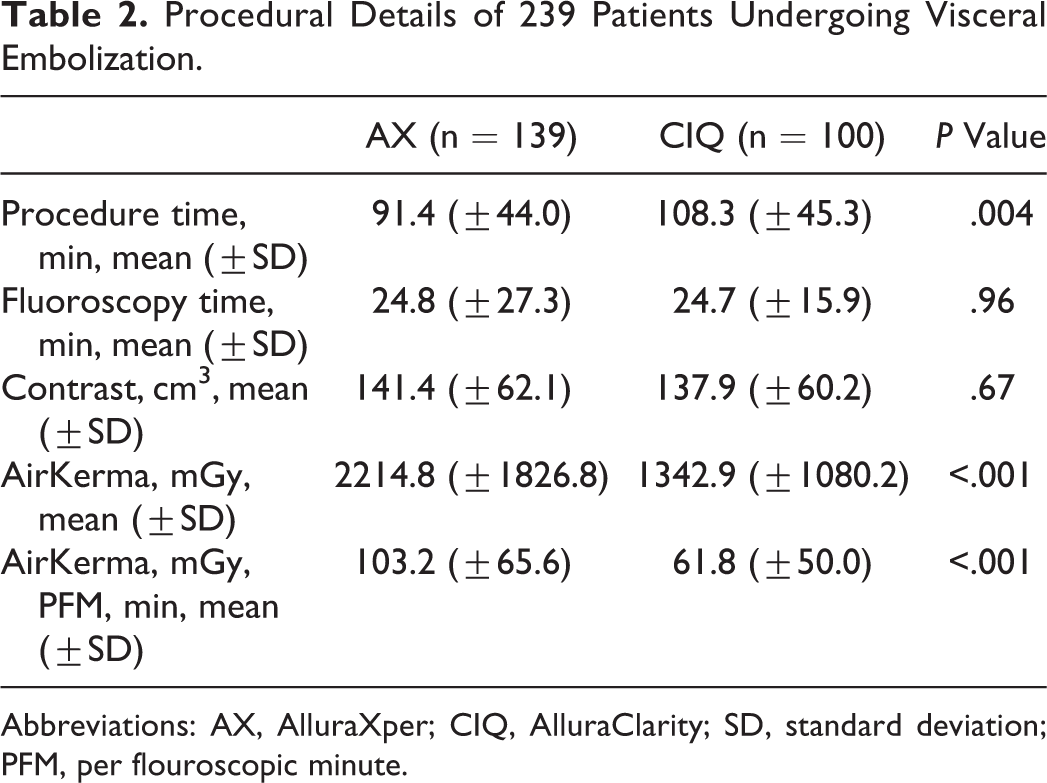
Abbreviations: AX, AlluraXper; CIQ, AlluraClarity; SD, standard deviation; PFM, per flouroscopic minute.
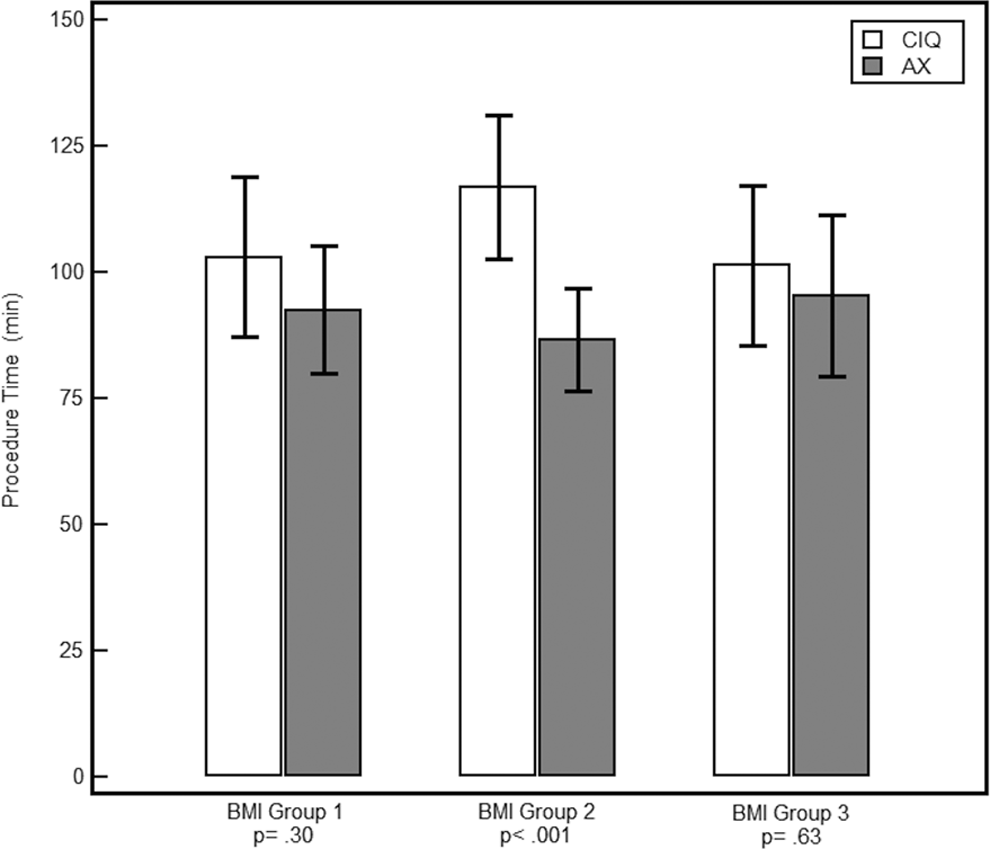
Depiction of procedure and fluoroscopy times according to BMI categories. BMI indicates body mass index.
Fluoroscopy time (24.7 ± 15.9 minutes vs 24.8 ± 27.3 minutes, P = .96, t test) and the use of contrast media volume (137.9 ± 60.2 vs 141.4 ± 62.1, P = .67, t test) were similar when comparing the CIQ and AX groups and showed no significant differences in BMI subgroup analysis.
The overall Ka, r was lower in the CIQ group compared to the AX group: 1342.9 ± 1080.1 mGy (95% CI: 1128.6-1557.2) versus 2214.8 ± 1826.8 mGy (95% CI: 1908.4-2421.2, P < .001, t test).
Accordingly, mean Ka, r was 970.1 ± 847.2 mGy (95% CI: 702.7-1237.5) versus 1586.1 ± 1335.0 mGy (95% CI: 1241.2-1930.9) when comparing CIQ and AX (P = .003, t test) in BMI group 1, 1484.7 ± 1160.6 mGy (95% CI: 1113.5-1855.9) versus 2170.1 ± 1458.2 mGy (95% CI: 1726.7-2613.4) in BMI group 2 (P = .02, t test) and 1848.8 ± 1128.0 mGy (95% CI: 1305.1-2392.5) versus 3348.9 ± 2395.7 mGy (95% CI: 2526.0-4171.9) in BMI group 3 (P = .001, t test), respectively (Figure 2).
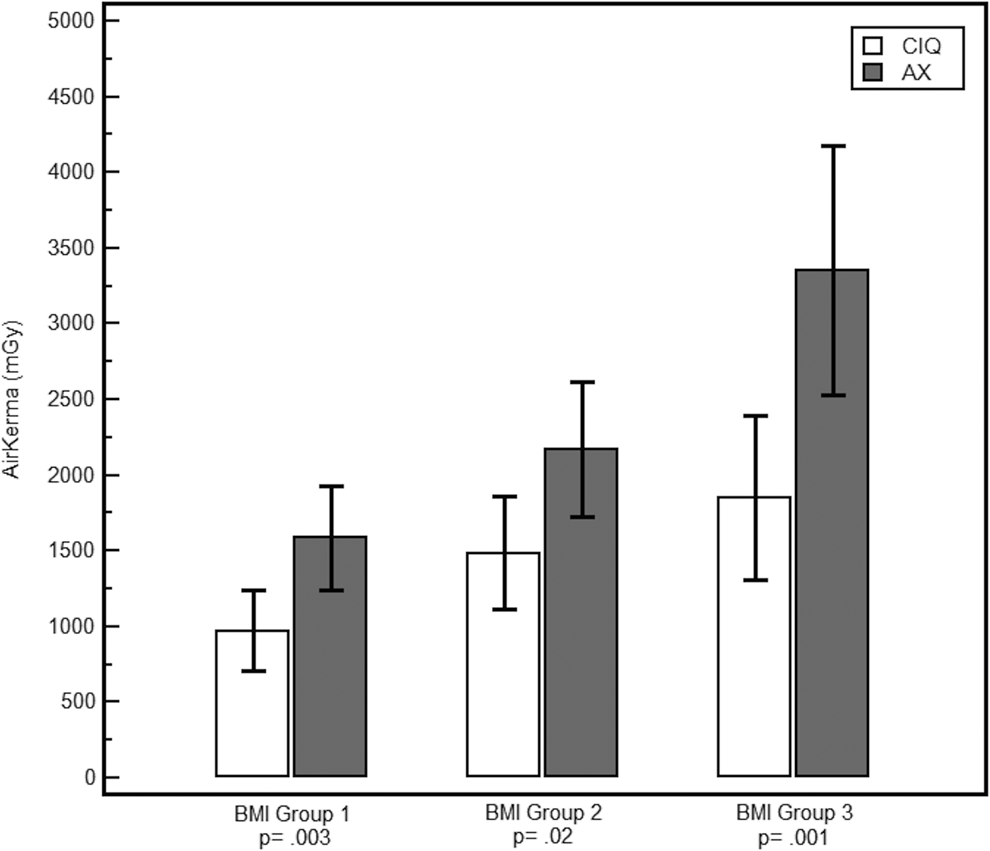
Ka, r values for the 3 different BMI groups. Ka, r indicates AirKerma; BMI, body mass index.
Discussion
There has been a rapid growth of endovascular therapies necessitating radiation within the last decades. 18,19 In line, operators have been faced with continued exposure and increasing cumulative radiation dose exposure. 18,19 This development and its consequences are a major concern not only for patients but also for the operators involved in angiographic interventional settings. 5,7,8,20,21 As a result, efforts to effectively reduce radiation dose while maintaining the necessary level of image quality have become paramount. 22 However, specific procedures such as visceral interventions as well as patients with higher body weight and BMI require more radiation to maintain image quality. 2 Therefore, technical advancements are necessitated to reduce radiation for these patients and procedures. The present study showed an average-dose reduction of 39.4% in patients treated with CIQ when compared to AX imaging technology, and this finding held true for all BMI groups.
Despite the challenges of comparing different imaging technologies within different settings, CIQ was previously shown to reduce radiation dose for no significant loss of image quality when compared to AX. 9,10,15,16 However, Soderman et al were the only one performing a 1:1 direct comparison of the image quality in an interventional neuroradiology setting. 9 In each patient, imaging was obtained using the CIQ and AX technologies. The images were reviewed in a randomized and blinded manner by 3 neuroradiologists and thereby, no loss of image quality was observed but the CIQ images were acquired using 25% of the AX radiation dose only.
Thereafter, multiple single-center series evaluated the potential of CIQ in reducing radiation dose for various types of procedures. Overall, a radiation dose reduction of >40% was achieved in all. 10 -13,15,16 However, there was a wide range of radiation dose reduction indicating that the benefit of CIQ varies according to the procedure type and patients’ habitus.
In order to properly generalize and to compare both imaging technologies in this study, the assessment of fluoroscopy time and the amount of contrast media utilized served as indirect parameters to assess procedural complexity between the 2 groups. The relatively large number of patients in both the groups is also important to help compare the groups. Fluoroscopy time and the amount of contrast media used were similar in both the groups (Table 2). Therefore, we suggest that the procedural complexity was comparable as indicated by the fluoroscopy time and the amount of contrast used, which we account as objective parameters.
The present study has several limitations. First, the current analysis is based on a retrospective evaluation of a deidentified data set. Therefore, it was not possible to review specific procedural protocols and angiograms. Nevertheless, the heterogeneous patient population and procedural complexity in this large study population allows for indirect comparison of the 2 imaging modalities. In addition, it was not possible to systematically compare the image quality of CIQ and AX technology.
Second, there were a variety of different visceral embolization procedures included within the present study limiting the interpretation of procedure time and radiation dose.
Conclusion
The present study demonstrated that radiation dose can be significantly reduced in patients undergoing visceral embolization procedures by the use of CIQ. As expected, the results show an increase in radiation dose correlating with patient size. Despite the variability in procedure complexity, a consistent dose reduction was identified across the range of patient BMI. The need to understand the amount of radiation dose reduction possible with new technological advances is important, as we attempt to determine which changes are truly significant while maintaining image and procedural quality. Further study of these technological advances is warranted especially for different acquisition protocols, as the number and complexity of angiographic interventional procedures continue to increase.
Footnotes
Authors’ Note
Barry T. Katzen is a member of the Advisory Board of Philips and has no direct conflict of interest to report with this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.