
Abstract
Aortocaval fistula (ACF) is a rare complication. Endovascular repair is an option for this fatal condition. However, endoleak and persistent fistula may occur and lead to technical failure. We performed endovascular repair for 3 cases of challenging ACF with hostile anatomy. Patient 1 was an 80-year-old man who complained of abdominal distension and lower limb edema for 15 days. He had renal and cardiac dysfunction. Computed tomography angiography (CTA) showed an ACF and extreme tortuosity of right iliac artery. The super-stiff guidewire could not pass the right iliac artery. We performed endovascular repair and an occluder was used to block the right external iliac artery. Postoperative CTA showed migration of the occluder, and we ligated the right external iliac artery. The patient survived for 5 years. Patient 2 was a 78-year-old man who complained of an acute abdominal pain for 30 hours. Computed tomography angiography showed great neck angulation (63.3°) and a huge aneurysm (9.9 cm in diameter). A type 1A endoleak occurred and an aortic cuff was deployed at the proximal seal zone. Meanwhile, a type 3 endoleak occurred because of the migration and detachment of the left iliac limb. Another stent-graft was deployed to connect the iliac limb. The patient was followed up for 1 year and remained in a good condition. Patient 3 was a 74-year-old man who experienced severe abdominal pain for 1 day. Computed tomography angiography showed great neck angulation (66°) and a huge aneurysm (10.1 cm in diameter). A type 1A endoleak occurred, and an aortic cuff was deployed at the proximal seal zone. The patient was followed up for 6 months. In conclusion, ACF is a rare but a fatal condition. Acute cases and chronic cases with instable hemodynamics need urgent diagnosis and surgical intervention. Endovascular repair is an efficacious alternative to the traditional open repair.
Keywords
Introduction
Spontaneous perforation of aortic aneurysms into the inferior vena cava (IVC) has been reported in 0.2% to 1.3% of patients with abdominal aortic aneurysm (AAA). Its incidence is twice as high in patients with a ruptured AAA. 1 The traditional treatment is open surgical repair. Fistula closure is performed within the aneurysm sac, and the repair is done with either a direct suture or a patch followed by AAA repair. Although venous bleeding can be controlled with sponge sticks, finger pressure, or large balloon catheters, open surgical treatment has been associated with mortality mainly from excessive blood loss. Perioperative mortality of aortocaval fistula (ACF) secondary to ruptured AAA treated with open surgical repair is high and ranges from 20% to 60%. 2,3
With the introduction and development of the aortic stent-graft technique, endovascular repair offers an alternative treatment for this fatal condition. The technical success rate of endovascular treatment is 94%, and intraoperative mortality is 0% with a 90-day mortality of 10%. 4 Successful endovascular repair depends on the anatomy of the aneurysm, such as the length of the attachment site, neck angulation, diameter and tortuosity of the access vessel, aneurysm sac size, and the presence of endoleak and fistula. Meanwhile, this fatal disease is usually complicated and difficult to treat under urgent conditions. We performed emergent endovascular repair for 3 cases with challenging ACF and hostile anatomy, 2 acute cases with ruptured AAA, and 1 chronic case with AAA and unstable hemodynamics. Type 1, type 2, or/and type 3 endoleaks occurred and subsequent endovascular repair, open repair, or conservative treatment was performed, respectively.
Patients and Methods
Patient 1: An 80-year-old man was admitted to our department for abdominal distension and bilateral lower limb edema of 15 days duration (Table 1). Physical examination revealed a pulsatile abdominal mass with continuous abdominal bruit. He had a bilateral lower limb, scrota edema, and congested neck veins. The average amount of urine produced was approximately 400 mL/d and serum creatinine was 210 µmol/L. Echocardiogram showed that the left ventricular ejection fraction (LVEF) was 49% and the pulmonary artery systolic pressure (PASP) was 69 mm Hg with pericardial effusion. The urgent computed tomography angiography (CTA) showed a ruptured right common iliac artery aneurysm into the right common iliac vein and extreme tortuosity of the right iliac artery (Figure 1A and B). Because of hemodynamic instability, the patient underwent emergent endovascular treatment under general anesthesia. The initial aortogram identified a large ACF, but the super-stiff guidewire could not completely pass the right iliac artery because of extreme tortuosity (Figure 1C). Therefore, we performed endovascular repair with an aorto-uni-iliac device (Lifetech Scientific Co, Ltd, Shenzhen, Guangdong) to exclude the aneurysm through the left iliac approach. A patent ductus arteriosus (PDA) occluder (the fixed disc was 24 mm in diameter; Lifetech Scientific Co, Ltd) was used to block the right external iliac artery, and a femoral–femoral bypass was performed simultaneously using a tube (8 mm in diameter) expanded polytetrafluoroethylene (ePTFE) graft (Bard Medical Division, Covington, Georgia; Figure 1D). Postoperative CTA showed a persistent communication between the aortic sac and the right common iliac vein because of a type 2 endoleak from the internal and external iliac artery and a type 1B endoleak due to an inadequate seal of the left common iliac artery. The PDA occluder migrated to the fistula site due to high flow from the distal external iliac artery (Figure 1E and F). To eliminate the high-flow type 2 endoleak, we ligated the right external iliac artery. We suggested using an additional extension to repair the type 1B endoleak, but the patient refused. Postoperative CTA showed partial thrombosis of the sac despite the presence of a persistent fistula due to endoleaks (Figure 1G). The amount of urine produced ranged from 2030 to 4810 mL/d and serum creatinine was 103 µmol/L on the third day. The patient was discharged 5 days later without abdominal pain and lower limb edema and underwent close follow-up. One month later, CTA showed no enlargement of the aneurysm sac and fistula (Figure 1H). At the two and a half-year of follow-up, CTA showed no obvious change of the aneurysm sac and fistula (Figure 1I). However, CTA also showed cardiac enlargement due to the persistent fistula (Figure 1J). Echocardiogram showed that the LVEF was 56% and the PASP was 52 mm Hg without pericardial effusion. The patient had no obvious symptoms and signs and underwent surveillance. At 5 years after the procedure, the patient died of cerebral hemorrhage.
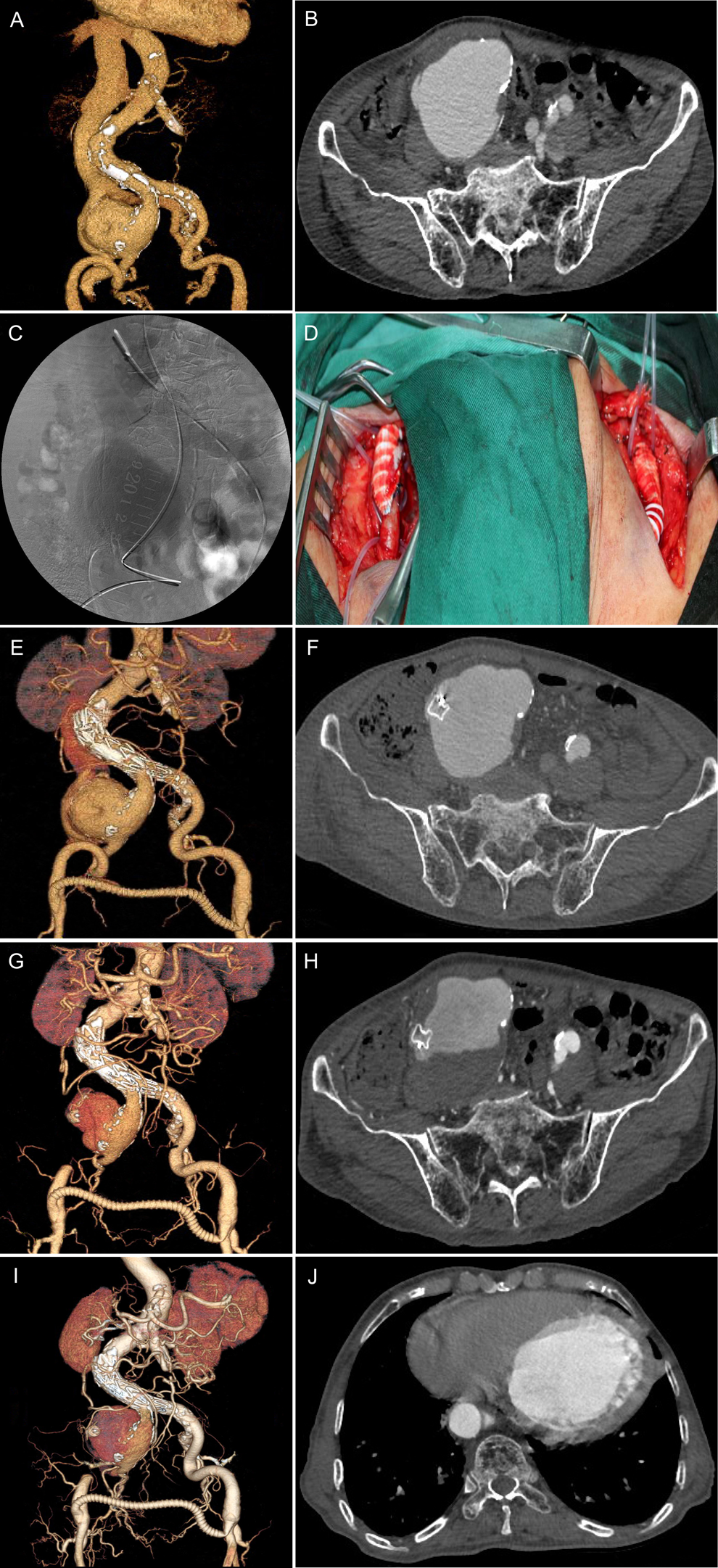
A, Computed tomography angiography (CTA) with three-dimensional reconstruction showing a ruptured right common iliac artery aneurysm with an ACF connecting the sac to the right common iliac vein and extreme tortuosity of right iliac artery. B, The maximum diameter of aortocaval fistula (ACF) was approximately 15 mm. C, The super-stiff guidewire could not completely pass the right iliac artery because of the extreme tortuosity. D, The patient underwent femoral–femoral bypass. E, Postoperative CTA showed a persistent communication between the aortic sac and the right common iliac due to type 2 and type 1A endoleaks. F, The patent ductus arteriosus (PDA) occluder migrated to the fistula. G, Postoperative CTA showed partial thrombosis of the aneurysm sac. H, CTA showed no
Clinical Characteristics of the 3 Cases of Challenging ACF.
Abbreviations: AAA, abdominal aortic aneurysm; ACF, aortocaval fistula; AUI, aorto-uni-iliac; BL, blood loss; CIV, common iliac vein; IVC, inferior vena cava; M, male; OT, operating time.
Patient 2: A 78-year-old man was admitted to the emergency department complaining of acute lower abdominal pain for 30 hours with dyspnea. His medical history included AAA, smoking, and coronary artery disease. On examination, his blood pressure was 85/55 mm Hg, heart rate was 108 beats/min, and respiratory rate was 20 breaths/min. Physical examination also revealed a pulsatile abdominal mass and continuous abdominal bruit. The average amount of urine produced was approximately 350 mL/d and serum creatinine was 322 µmol/L. Urgent CTA showed an infrarenal ruptured AAA and retroperitoneal hematoma with an ACF connecting the sac to the lower part of the IVC (Figure 2A). Computed tomography angiography also showed severe angulation of the proximal neck (63.3°), a large aneurysm (9.9 cm in diameter), extreme tortuosity of left iliac artery, and that the lower part of the IVC was compressed by the aneurysm (Figure 2B). The patient underwent urgent endovascular repair under local anesthesia. Initial angiogram confirmed the large aneurysm with an ACF and a great angle of the proximal neck (Figure 2C). A bifurcated stent-graft (Cook medical, Bloomington, Indiana) was deployed to treat the aneurysm; and a cuff (W. L. Gore and Associates, Flagstaff, Arizona) was deployed to seal the landing zone of the left common iliac artery. However, a type 1A endoleak occurred (Figure 2D). Therefore, an aortic cuff (W. L. Gore and Associates, Inc) was deployed at the proximal seal zone, and the subsequent aortogram no longer showed a type 1A endoleak (Figure 2E). However, a type 3 endoleak occurred because of the migration and detachment of the left iliac limb due to the large aneurism sac (Figure 2E). Another stent-graft (Cook medical) was deployed to connect the iliac limb (Figure 2F). We did not perform a complete angiogram because of renal dysfunction and contrast-induced nephropathy. Postoperatively, the amount of urine produced ranged from 1100 to 3650 mL/d. Serum creatinine was 84 µmol/L on the seventh day. Echocardiogram showed that the LVEF was 58% and the PASP was 36 mm Hg without pericardial effusion. The patient was followed up for 1 year and remained in a good condition.
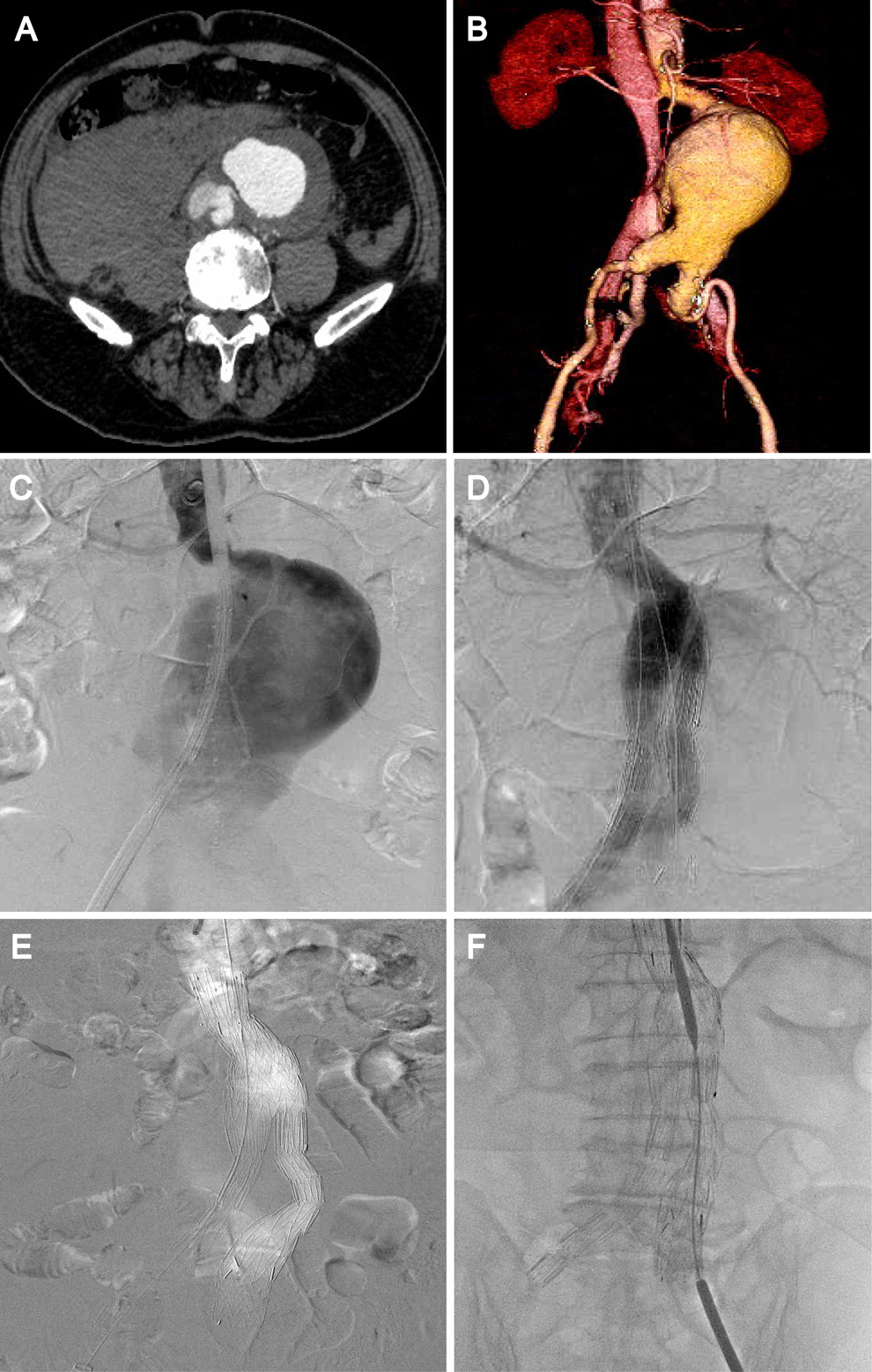
A, Urgent CTA showed an infrarenal ruptured abdominal aortic aneurysm (AAA) and retroperitoneal hematoma with an ACF connecting the sac to the lower part of the inferior vena cava (IVC). The maximum diameter of the ACF was approximately 13.5 mm. B, CTA showed severe angulation of the proximal neck (63.3°), a huge aneurysm, extreme tortuosity of left iliac artery, and that the lower part of the IVC was compressed by the aneurysm. C, Initial angiogram confirmed the large aneurysm with ACF and the great angle of the proximal neck. D, The type 1A endoleak occurred after the urgent endovascular repair. E, A cuff was deployed at the proximal landing zone to repair the type 1A endoleak, and the left limbs migrated and detached. F, A stent-graft was deployed to connect the iliac limbs to repair the type 3 endoleak.
Patient 3: A 74-year-old man was admitted to the hospital for abdominal pain of 3 days duration, which was worsened for 1 day. The patient had a history of hypertension and coronary artery disease. The heart rate and blood pressure were normal. Physical examination revealed a tender and pulsatile abdominal mass without abdominal bruit. No clinical signs of venous hypertension or heart failure were observed. The average amount of urine produced was approximately 500 mL/d and serum creatinine was 202.3 µmol/L. Urgent CTA showed a large ruptured AAA (10.1 cm in diameter) with an ACF connecting the sac to the lower part of the IVC, which was compressed, and the proximal neck was extremely tortuous (66°; Figure 3A and B). The patient underwent urgent endovascular repair under local anesthesia, and a bifurcated stent-graft (Cook Medical) was implanted, but a type 1A endoleak remained (Figure 3C). An aortic cuff (Cook Medical) was deployed at the proximal seal zone to repair the endoleak (Figure 3D). The amount of urine produced ranged from 1960 to 2990 mL/d, and serum creatinine was 75.9 µmol/L on the fifth day postoperatively. Echocardiogram showed that the LVEF was 60% and the PASP was 26 mm Hg. On the tenth day after the operation, CTA showed complete thrombosis of the aneurysm sac and no evidence of the endoleak or the fistula (Figure 3E and F). The patient was discharged uneventfully. The patient was followed up for 6 months and remained in a good condition. Computed tomography angiography showed no evidence of endoleak, fistula, or retroperitoneal hematoma (Figure 3G and H).
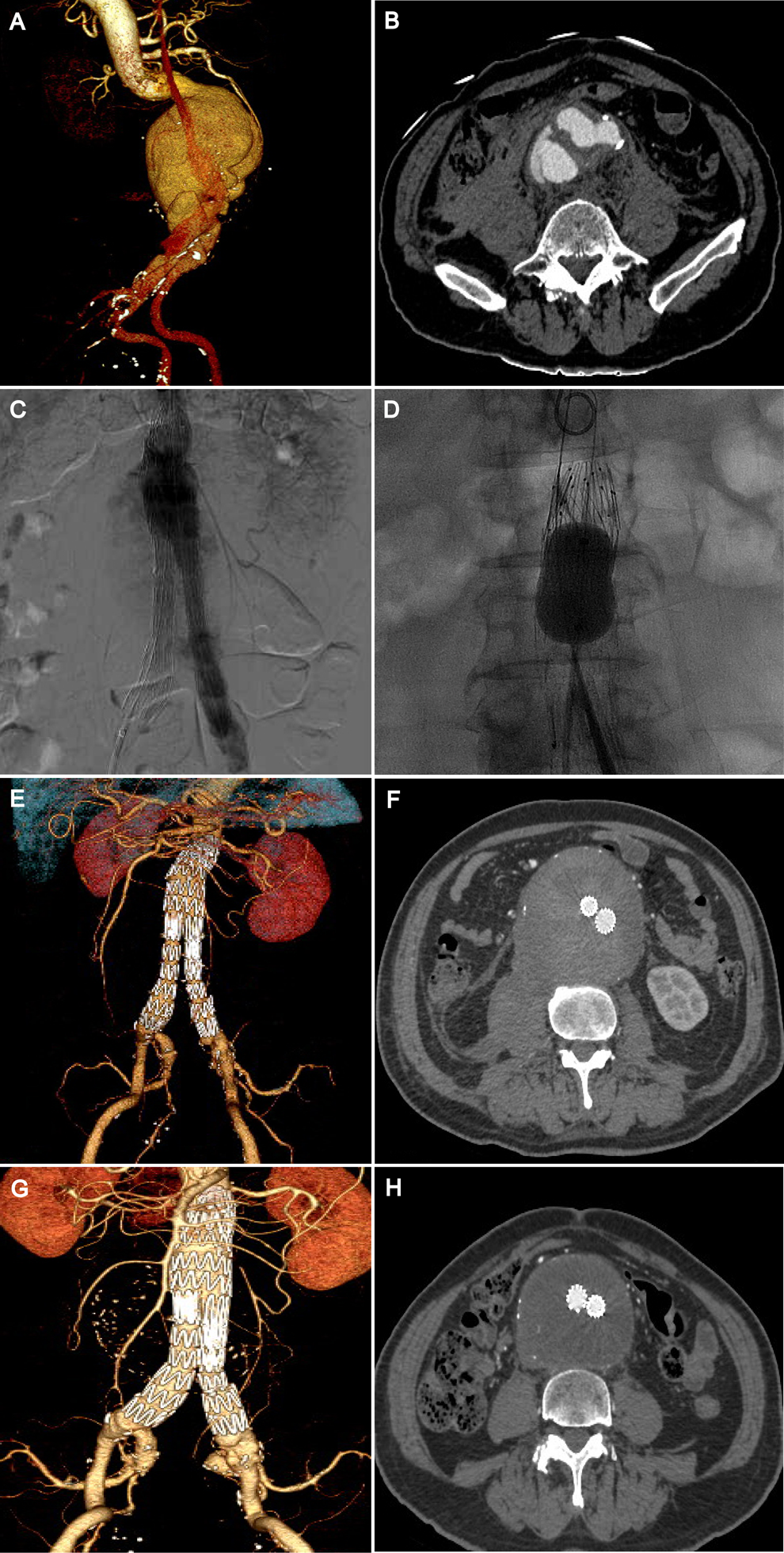
A, Urgent CTA showed a large ruptured AAA with ACF connecting the sac to the lower part of the IVC and showed that the proximal neck was extremely tortuous. B, The maximum diameter of the ACF was approximately 12 mm. C, There was a type 1A endoleak after the endovascular repair. D, A cuff was deployed at the proximal landing zone to repair the endoleak, and balloon dilation was performed. E, Postoperative CTA showed no evidence of the endoleaks or the fistula. F, CTA revealed complete thrombosis of the aneurysm sac. G and H, At the 6-month follow-up, CTA showed no evidence of endoleak, fistula, or retroperitoneal hematoma.
The study was approved by the ethical committee of the Affiliated Hospital of Qingdao University, and informed consent was obtained from the individuals.
Discussion
Aortocaval fistula is a rare but a life-threatening condition with complex clinical presentation. Primary ACF is associated with AAA rupture in 80% of the cases. The most common fistula site is the aortocaval segment. The mortality of ACF is suggested to be associated with AAA rupture and depends largely on blood loss, hemodynamic impairment, and comorbidities. Open surgical repair is associated with high morbidity and mortality.
Since endovascular repair has been adopted as a valid treatment for ruptured AAA, endovascular repair of ruptured AAA provides a less-risky alternative for the management of ACF with the advantages of markedly reduced operative time, blood loss, and postoperative recovery time as well as a superior outcome. However, this fatal disease is usually complicated and difficult to treat. One of the principle reasons for endograft failure is the presence of endoleaks, which are present in 50% of all ACF cases. 5 A great angle at the proximal neck or a short proximal neck is a risk factor for type 1 endoleaks. A large aneurysm sac is another risk factor for type 1 and type 3 endoleaks because of the potential migration of the stent-graft. Type 1 and type 3 endoleaks, if identified intraoperatively, should be treated before leaving the procedure room. The continued presence of endoleaks may result in repressurization of the excluded aneurysm sac, which may cause consequent growth and ultimately rupture. These are often treated with a second endoluminal procedure such as balloon dilation or placement of additional stent-grafts or aortic cuffs. In some instances, staged repair of these endoleaks can be performed because the presence of a fistula causes a pressure gradient that results in the decrease of in-sac pressure. For the first patient, the follow-up CTA showed no enlargement of the aneurysm sac despite the persistent fistula from the type 1B and type 2 endoleaks.
However, the progression of type 2 endoleaks after endovascular repair of ruptured AAA with ACF remains unknown, and there is no clear evidence in the current literature to guide the treatment. We performed a literature review of the published reports to draw some conclusions regarding the treatment of endoleaks. From 1998 to 2015, 17 articles reported on 17 patients presenting with endoleaks after endovascular stent-grafting of ruptured AAA with an ACF (Table 2). 2,6 -21 The site of the fistula was the aortocaval segment in 14 (82%) patients and iliocava segment in 3 (18%) patients. The most common endoleak was type 2 endoleak, which occurred in 12 patients. Seven patients were managed conservatively, and 6 of these endoleaks sealed spontaneously. 9,11,12,16 -18,20 There was a persistent flow over the ACF with shrinkage of the aneurysm sac in 1 patient at the 2-year follow-up. 20 The other 5 patients with type 2 endoleaks underwent intervention. Two patients underwent stent-grafting in the IVC, 1 patient was treated by coiling of the inferior mesenteric artery (IMA), 1 patient was treated by closing the fistula with an occluder, and 1 patient underwent ligation of the hypogastric artery and the IMA. 3,8,14,15,21 In summary, the conservative approach may be preferable for type 2 endoleaks in the absence of systemic manifestations and when there is favorable aneurysm sac remodeling. 18 In the presence of a persistent ACF and type 2 endoleaks, the connection between the aneurysm sac and the low-pressure venous system leads to a pressure gradient, resulting in a decrease of in-sac pressure. Due to the low-pressure, low-flow type 2 endoleaks have a very low probability of aneurysm sac enlargement. Nevertheless, secondary intervention may be performed for patients with a persistent ACF combined with aneurysm sac enlargement or systemic manifestations.
Management of Endoleaks After Endovascular Stent-Graft of Ruptured AAA With ACF.
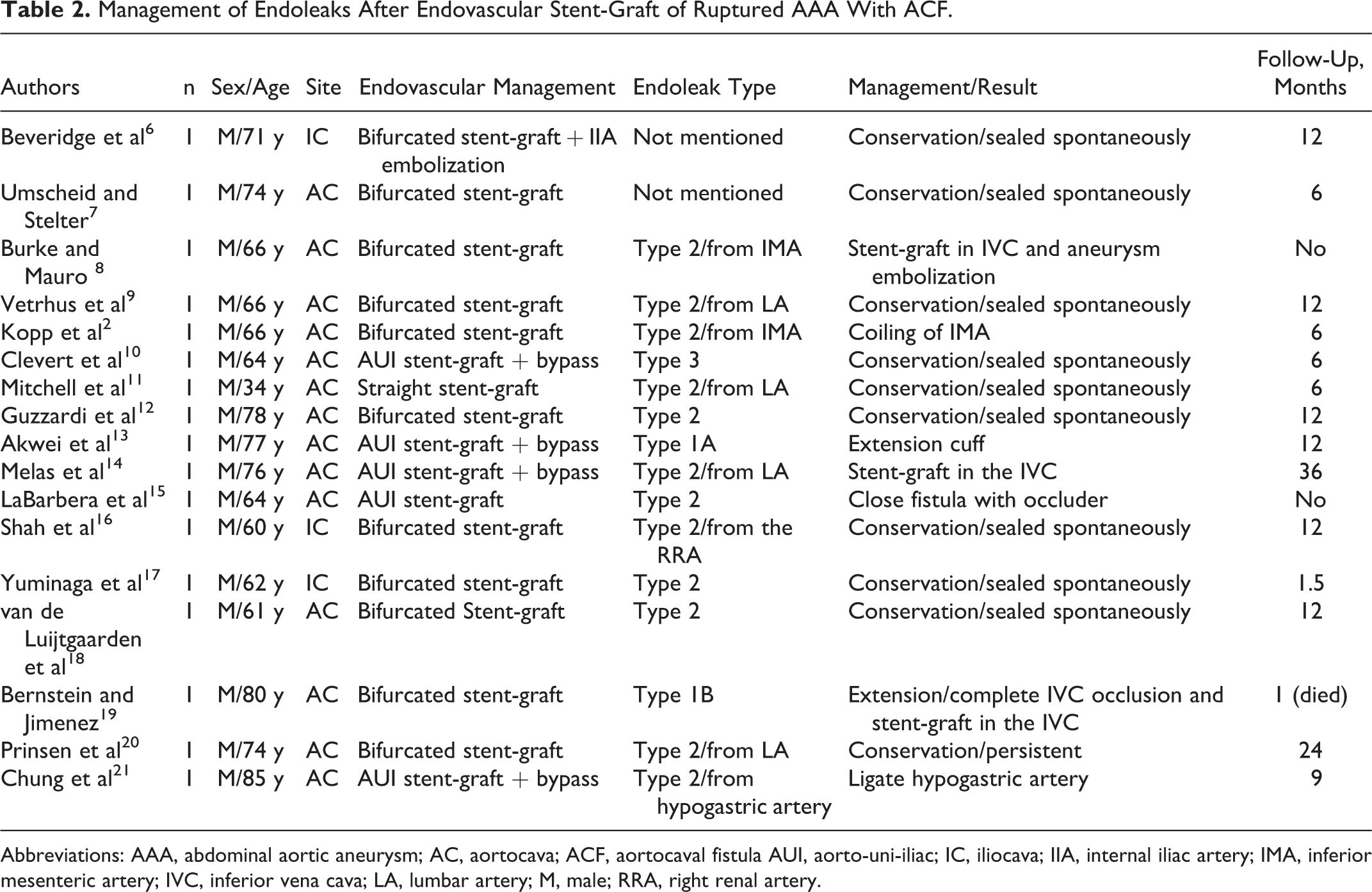
Abbreviations: AAA, abdominal aortic aneurysm; AC, aortocava; ACF, aortocaval fistula AUI, aorto-uni-iliac; IC, iliocava; IIA, internal iliac artery; IMA, inferior mesenteric artery; IVC, inferior vena cava; LA, lumbar artery; M, male; RRA, right renal artery.
Increasing cardiac output and heart failure may develop from persistent fistulas. Early closure of the fistula has been advocated due to concerns about these aneurysm-related complications. The question remains regarding if and how we manage these persistent fistulas. Staged or simultaneous sealing of the fistula was done through the deployment of stent-grafts in the IVC or an occluder in the fistula site to achieve complete control of the ACF. 14,15,19,22 However, stent-graft placement in a significantly compressed IVC may yield suboptimal results with a risk of endograft collapse, acute IVC thrombosis, or both. 19 Therefore, persistent fistulas due to type 2 endoleaks after endovascular abdominal aortic aneurysm rapair (EVAR) may be managed conservatively, and favorable remodeling of the aneurysm sac is possible. Nevertheless, close surveillance is mandatory. In addition, ACF can present with signs of venous hypertension and high-output cardiac failure, such as lower extremity swelling, scrotal edema, hematuria, or even renal dysfunction. Sealing off the ACF can result in an acute reduction of venous pressure and cardiac preload and output. The patient may present with low blood pressure intraoperatively. The patient would subsequently need invasive blood monitoring, timely fluid resuscitation, and diuresis.
Conclusion
Although very rare, ACF requires urgent diagnosis. Acute cases and chronic cases with unstable hemodynamics need emergent surgical intervention. Endovascular repair is an efficacious alternative to traditional methods, especially in elderly patients with multiple comorbidities. However, these cases are often challenging and difficult to treat. Under urgent conditions, endoleaks due to hostile anatomy may result in technical failure and should be treated properly. A conservative approach may be preferable for low-flow type 2 endoleaks, whereas high-flow type 1, type 2, and type 3 endoleaks must be repaired.
Footnotes
Authors’ Note
Y.W., H.W., Y.Z. contributed to conception and design. Y.W. and W.Y. contributed to analysis and interpretation and writing the article. Y.L. contributed to data collection. W.Y., H.W., and Y.Z. contributed to critical revision of the article. Y.W., W.Y., Y.L., H.W., and Y.Z. contributed to final approval of the article. Y.W. contributed to statistical analysis and overall responsibility.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.