
Abstract
Chronic mesenteric ischemia most commonly occurs secondary to atherosclerotic disease of the mesenteric arteries. Patients are often older than 60 years and can present with postprandial abdominal pain, nausea, diarrhea, and significant weight loss. Symptomatic disease has traditionally been managed with open surgical repair, but endovascular strategies, such as percutaneous angioplasty and stenting, have emerged as the mainstays of therapy. Complications from stenting include plaque embolization, thrombosis, perforation, or dissection of the mesenteric arteries. We present a patient with symptomatic acute aortic dissection 18 months after celiac and superior mesenteric artery stent placement for chronic mesenteric ischemia.
Keywords
Introduction
Chronic mesenteric ischemia (CMI) is an important cause of abdominal pain and most commonly occurs secondary to atherosclerotic disease of the mesenteric arteries. Patients are typically older than 60 years and can present with postprandial abdominal pain, nausea, diarrhea, and significant weight loss. 1 Symptomatic disease has traditionally been managed with open surgical repair, but endovascular strategies, such as percutaneous angioplasty and stenting, have emerged as the mainstays of therapy. These less invasive endovascular procedures have proven to be invaluable in high-operative risk patients with multiple comorbidities. 2,3 Complications from stenting include plaque embolization, thrombosis, perforation, or dissection of the mesenteric arteries, which may require additional salvage procedures. Previous reports of mesenteric artery dissection have occurred immediately during or in the perioperative period after stent deployment for CMI. 4 We present a patient with symptomatic aortic dissection 18 months after celiac artery and superior mesenteric artery (SMA) stent placement for CMI. Consent was obtained from next of kin, and institutional review board approval was not required from our institution for the case report submission.
Case Report
History and Examination
An 89-year-old woman with a history of medically controlled hypertension, renal artery stenosis, congestive heart failure (CHF), and right hemicolectomy for cecal cancer 4 years previously, presented with abdominal discomfort after eating, food fear, diarrhea, and 20-pound weight loss. Computed tomography imaging demonstrated high-grade stenosis of both the celiac and superior mesenteric arteries.
Intervention and Postintervention Course
The patient underwent selective angiography of the celiac and superior mesenteric arteries via a percutaneous brachial approach, which demonstrated 80% to 90% stenosis at the origin of the celiac artery and at least a 70% to 80% stenosis of the origin of the SMA. Superior mesenteric artery was cannulated first without complication using a 0.014 ProWater wire (Abbott Laboratories, Abbott Park, Illinois), and percutaneous angioplasty of the SMA was performed using a 6-mm × 40-mm Sterling balloon (Boston Scientific, Marlborough, Massachusetts), with mild angiographic improvement in stenosis to 60%. A 7-mm × 19-mm Express SD stent (Boston Scientific) was placed and postdilated, with satisfactory correction of the SMA stenosis. The celiac artery was heavily calcified and more difficult to cannulate than the SMA, and the stenosis was initially dilated with a 6-mm × 40-mm Sterling balloon with no residual angiographic improvement. Subsequently, a 6-mm × 18-mm Express SD stent (Boston Scientific) was deployed and postdilated with an 8-mm × 40-mm noncompliant Sterling balloon (Boston Scientific). There appeared to be full recanalization of the origin of the celiac artery, and completion angiography confirmed satisfactory positioning of the stents (Figure 1).
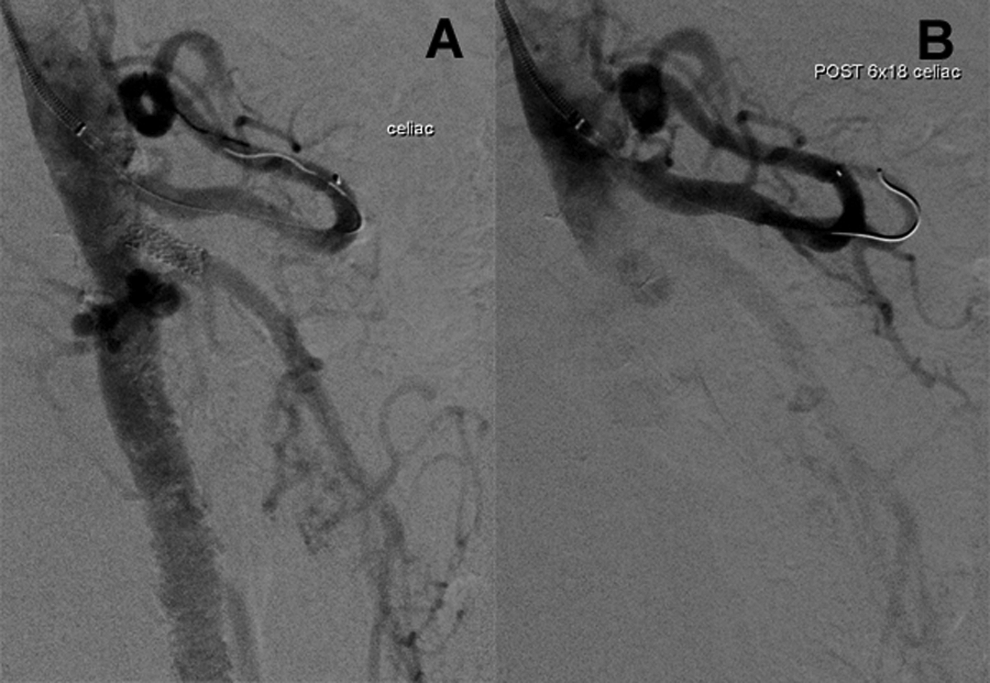
Completion angiography confirms satisfactory positioning and patency of the superior mesenteric artery (SMA; A) and celiac artery (B) stents.
The patient’s blood pressure remained medically controlled during her preoperative, perioperative, and postoperative course, with systolic blood pressures ranging from 110 to 120 mm Hg. Eighteen months later, the patient returned with complaints of new-onset abdominal pain. Computed tomography imaging revealed an acute aortic dissection measuring approximately 5-cm × 4-cm, with a dissection flap at the level of the SMA extending to the infrarenal aorta (Figures 2 and 3). She declined any further intervention and died 1 month later from a CHF exacerbation.

Axial computed tomography (CT) images before (A) and after (B) superior mesenteric artery stent placement, demonstrating the development of an acute aortic dissection flap at the superior mesenteric artery (SMA).

Acute aortic dissection is seen on coronal computed tomography (CT) imaging 18 months following placement of celiac and superior mesenteric artery stents.
Discussion
Atherosclerotic disease of the mesenteric arteries occurs in 17% of patients older than 65 years, although most are asymptomatic due to collateral blood supply. 1 Patients present with abdominal pain, nausea, and weight loss, and usually with at least 2 mesenteric arteries affected. Treatment is mandatory for symptomatic patients, although management of asymptomatic patients remains controversial. With the evolution of new and lower profile technologies, endovascular repair is often preferred in selected patients and provides a minimally invasive approach that can serve as definitive therapy or as a bridge to open surgery until the patient stabilizes and nutritional status improves. 5
Alternatively, open surgery may be prioritized for patients who can tolerate the procedure, with endovascular therapy reserved for patients who are at increased risk of operative mortality due to advanced age and other comorbidities. 6 –9 There appears to be a decrease in the length of hospital stay and an overall reduction in morbidity and mortality with endovascular management. 10 However, long-term patency is higher with open surgery, and patients who undergo endovascular repair have higher rates of restenosis requiring subsequent reinterventions. 11 –13 Several complications unique to endovascular interventions can occur, including thrombosis, perforation, plaque embolization, rupture, and dissection of the mesenteric vessels. 4 These issues are typically recognized during the procedure or in the immediate postintervention recovery period and can increase the length of hospitalization, risk of death, and morbidity. Salvage procedures including additional stent placement, thrombolysis, or conversion to open repair may be needed. 4
In the case of an acute dissection after an endovascular procedure, stent placement may be required once it is identified in order to avoid distal propagation and arterial occlusion. If inadequately treated, dissection may result in bowel ischemia. 10 One case of a dissecting pseudoaneurysm of the SMA developing after angiography in a patient with acute mesenteric ischemia has been reported, which was successfully managed with bare-metal stent placement. 14 However, dissection of the aorta itself has not been reported previously. Our patient presented with an unusual complication of a symptomatic acute aortic dissection, 18 months after celiac artery and SMA stent placement for CMI; this may have been caused by a small injury to the wall of the aorta during her initial intervention, leading to weakening of the intima that developed into an acute aortic dissection over time. Continued follow-up in these patients, with clinical assessment of symptoms including abdominal pain, nausea, vomiting, as well as duplex ultrasound scans at 1, 3, and 6 months, and then every 6 months, could potentially identify patients in need of further intervention before more severe complications develop. 13
Conclusion
Endovascular mesenteric artery stenting is a safe and effective approach for the treatment of CMI and is often the preferable option for revascularization in patients with symptomatic disease. Continued clinical and radiological follow-up is necessary, and although complications such as aortic dissection after intervention for CMI can occur in the postoperative period, delayed presentation should be considered in the management of patients with a history of endovascular interventions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partly supported by National Institutes of Health grant T32 HL007734.