
Abstract
Aim:
To evaluate the protective role of routine shunting in patients with acute watershed stroke (WS) undergoing carotid endarterectomy (CEA).
Methods:
A total of 138 patients with symptomatic carotid stenosis (SCS) who underwent CEA after acute ischemic stroke from March 2008 to March 2015 were included in this study. Transient ischemic attacks were excluded. These patients were divided into 2 groups according to the topographic pattern of the stroke on magnetic resonance imaging: group 1, territorial strokes (TS) caused by emboli of carotid origin, and group 2, WS caused by a hemodynamic mechanism related to an SCS. Primary end points were 30-day mortality and postoperative neurological morbidity. The insertion of a Pruitt carotid shunt was performed systematically.
Results:
Ninety (65.2%) patients presented a TS of carotid origin and were included in group 1, and 48 (34.8%) of the 138 patients had a WS related to an SCS and were included in group 2. The median time between clinical onset of the cerebral ischemic event and surgery was 9 days (range: 0-89 days). Postoperative mortality was 0%. Seven (5.1%) patients had an aggravation of the neurological status during the postoperative period, of whom 2 presented a complete regression of the symptoms in less than 1 hour (definitive postoperative neurologic morbidity: 3.6%). Postoperative neurologic morbidity rate was significantly higher in the TS group (7 of 90; 7.8%) compared to the WS group (0 of 48; P = .04). No other independent predictive factor of neurologic morbidity after CEA for an SCS was found.
Conclusions:
Our results suggest that routine shunting should be considered in case of acute WS since it may play a protective role. Further studies are eagerly awaited to better define the timing and the best treatment option for both acute WS and TS related to an SCS in order to reduce postoperative neurologic morbidity.
Keywords
Introduction
The etiopathological mechanism underlying ischemic stroke plays an important role in long-term prognosis, risk of recurrence, and also postoperative risk after carotid endarterectomy (CEA). 1,2 In symptomatic carotid stenosis (SCS), in particular, 2 different mechanisms have been described: artery-to-artery embolism that leads to territorial strokes (TS) 3,4 and low-flow mechanism that causes the so-called border-zone, junctional, or watershed strokes (WS). 5
Watershed strokes constitute between 10% and 64% of all cerebral infarcts 5 -8 and are associated with a high risk of future cardiovascular events and stroke recurrence. 1 A low-flow mechanism is implied when infarcts are located in border-zone areas at the junction between 2 main arterial territories. 1,9 So, the topographic pattern of WS is specific and can be readily differentiated from TS of embolic origin by preoperative diffusion-weighted and perfusion-weighted magnetic resonance imaging (MRI). 10
Early CEA has been shown to be the most effective treatment in preventing cerebrovascular events in symptomatic patients. 11,12 Nevertheless, data from the literature are still scant and the outcome of CEA in relation to the topographic patterns and the etiopathological mechanism of the cerebral ischemia (embolic vs hemodynamic) has been analyzed in only 1 paper so far. 2 In this study, Jean-Baptiste et al showed that WS, compared to TS, were associated with a higher complication rate during the postoperative period of CEA performed after an acute ischemic stroke (AIS). Indeed, it is assumable that a prolonged carotid cross-clamping time may enhance the ischemic damage in border-zone territories. Moving forward from this preliminary report, in the present study, we evaluated the protective role of routine shunting in patients with acute WS undergoing CEA, since shunting may shorten carotid cross-clamping time and protect the so-called watershed territories from additional ischemic damage.
Materials and Methods
Patients and Study Design
Records of all patients with SCS who underwent CEA at our institution during the period from March 2008 to March 2015 were entered into a prospective database. Symptomatic carotid stenosis was defined as a carotid degree of stenosis >50% North American Symptomatic Carotid Endarterectomy (NASCET) 13 associated with ipsilateral hemispheric stroke or transient ischemic attack (TIA) within 90 days before surgery. We enrolled all neurologically stable patients with MRI-documented AIS who underwent ipsilateral CEA. Therefore, TIAs without the evidence of an acute MRI cerebral lesion (hyperintense signal on diffusion-weighted sequences or on fluid-attenuated inversion recovery sequences) were not considered for analysis because of the impossibility to clearly differentiate low-flow TIAs from embolic ones.
According to the updated Society for Vascular Surgery guidelines, 14 patients with an acute fixed deficit of >6 hours’ duration, a mild or moderate deficit, and limited areas of infarct (<30% of hemispheric volume) were considered for carotid intervention after a period of medical stabilization performed by a team of vascular neurologists. Carotid endarterectomy was preferably carried out within the first 2 weeks after the event. 14 -16 Delayed procedures (2 weeks-3 months), in case of initial neurologic instability, were performed as soon as possible, after evaluation by a team composed by vascular neurologists, neuroradiologists, and vascular surgeons. Neurologic instability included patients with unresolved associated brain hemorrhage, associated disabling nonrecuperating neurological deficit, and large volume infarctions on initial imaging.
A college of vascular neurologists and neuroradiologists divided the patients into 2 groups, according to the pathophysiological mechanism of the stroke as shown by its MRI topographic pattern:
Group 1: TS caused by emboli of carotid origin in the middle or anterior cerebral artery (Figure 1).
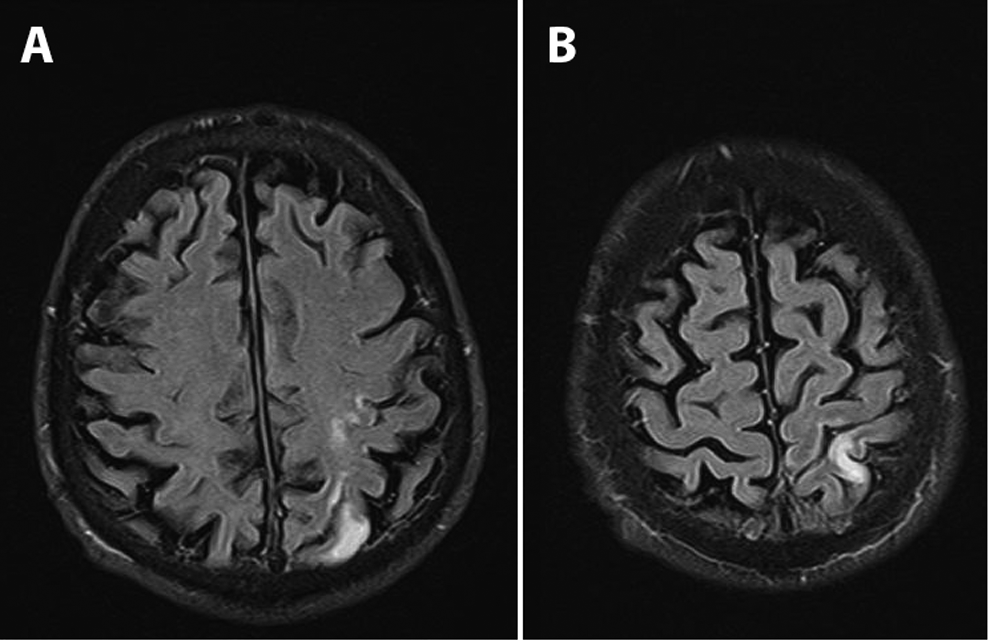
Fluid-attenuated inversion recovery (FLAIR) sequences of cerebral magnetic resonance imaging showing small cortical embolic infarcts in the middle cerebral artery distal territory.
Group 2: Supratentorial WS caused by a hemodynamic mechanism (low-flow) related to an SCS (Figure 2).
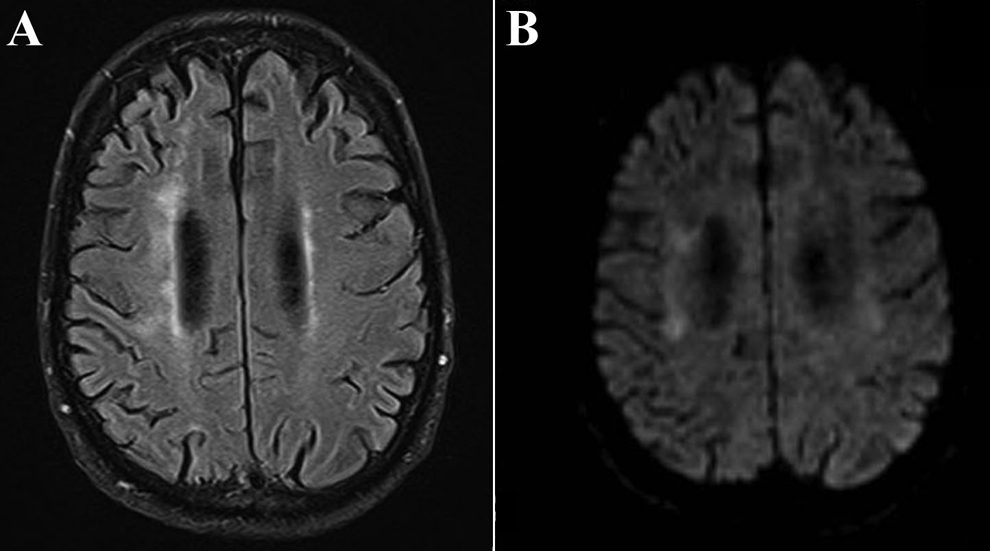
Brain magnetic resonance imaging. A, Axial image showing high-signal lesions on T2 fluid-attenuated inversion recovery in a watershed infarction distribution. B, The same region shows restricted diffusion on diffusion-weighted imaging (DWI) sequences due to continuous ischemia of the border zone.
Specifically, a vascular neurologist and a neuroradiologist blindly evaluated preoperative MRI retrospectively to assign patients to group 1 or 2, according to the criteria indicated in the review by Momjian-Mayor and Baron. 5 In case of disagreement, a third neurologist with more than 20-year experience in vascular cerebral diseases (D.M.B.), who was blinded to the results of the first evaluation, assigned the patient to the TS or WS group.
Clinical, anatomical, and radiological data were collected in a prospective vascular database and analyzed retrospectively. Specifically, patients’ age, gender, cardiovascular risk factors (hypertension, coronary artery disease [CAD], tobacco smoking, atrial fibrillation, diabetes mellitus, and dyslipidemia), ICA degree of stenosis, presence of a contralateral carotid stenosis or occlusion and its association with vertebral artery stenosis/occlusion, presence of a noncompetent circle of Willis, carotid cross-clamping duration, use of antiplatelet drugs, delay between the onset of symptoms and surgery, and preoperative National Institutes of Health Stroke Scale (NIHSS) values were obtained for analysis (Table 1). Vertebral artery disease was considered when the stenosis was >60% in both vertebral arteries or >60% in the dominant vertebral artery if the contralateral one was hypoplastic, ended in a posteroinferior cerebellar artery, or was occluded. A noncompetent circle of Willis was defined as the absence of collateral blood flow via the anterior communicating or the posterior communicating artery, evaluated on preoperative computed tomography angiography (CTA).
Baseline Characteristics of the 2 Groups.
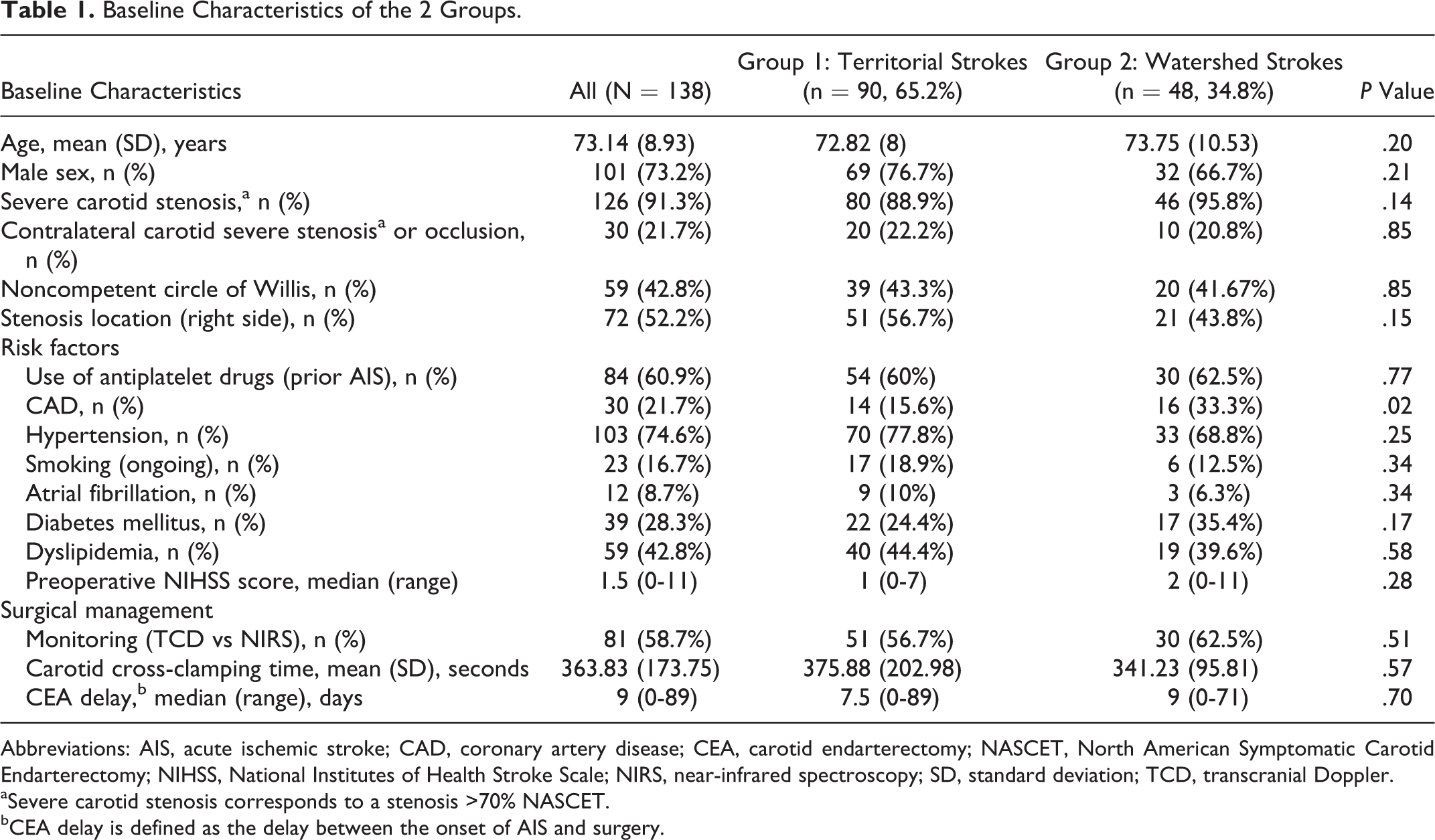
Abbreviations: AIS, acute ischemic stroke; CAD, coronary artery disease; CEA, carotid endarterectomy; NASCET, North American Symptomatic Carotid Endarterectomy; NIHSS, National Institutes of Health Stroke Scale; NIRS, near-infrared spectroscopy; SD, standard deviation; TCD, transcranial Doppler.
aSevere carotid stenosis corresponds to a stenosis >70% NASCET.
bCEA delay is defined as the delay between the onset of AIS and surgery.
Primary end points were 30-day mortality and postoperative neurological morbidity, defined as any deterioration or aggravation of the neurological status of the patients after CEA. Follow-up was undertaken with accurate clinical analysis, performed by the vascular neurologists, at day 0, 1, 2, and weekly thereafter until day 30. The ethical review board of our institution approved this study, and written informed consent was obtained from all patients.
Surgical Management
All CEAs were carried out under general anesthesia, and the insertion of a Pruitt Carotid Shunt (Pruitt F3 Carotid Shunt with T-Port 9F or 8F; LeMaitre Vascular Inc, Burlington, Massachusetts) was performed systematically (Figure 3). All patients underwent preoperative ultrasound examination and CTA for confirmation of the presence of the carotid lesion and preoperative planning (ie, evaluation of the extension of the plaque or the presence of tandem stenosis). We performed CEA when the ipsilateral carotid stenosis was 50% to 99% NASCET. 17 Each patient of this study underwent eversion CEA, as it is customary in our service for the great majority of the patients. Carotid endarterectomies were performed by an experienced surgical team with combined stroke and death rate <3% for neurologically asymptomatic patients. Proper shunt functioning, as well as cerebral perfusion, was verified during each surgical procedure by transcranial Doppler (TCD; MultiDop T2; Compumedics DWL Germany GmbH, Singen, Germany) or near-infrared spectroscopy (NIRS; INVOS 5100C Cerebral/Somatic Oximeter; Covidien, Mansfield, Massachusetts). Transcranial Doppler was the first choice, since it can monitor both cerebral perfusion (by insoning the middle cerebral artery) and microembolic signals. Near-infrared spectroscopy was chosen in case of inadequate temporal bone window for TCD.
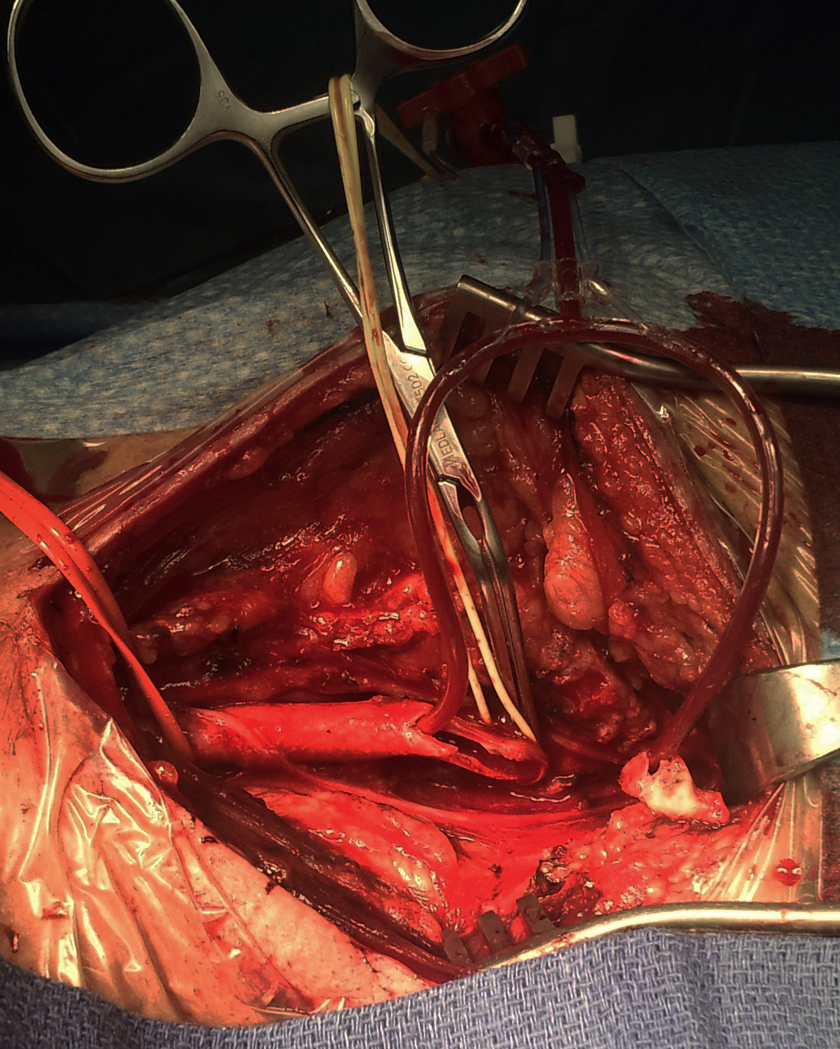
Eversion carotid endarterectomy (CEA) with the insertion of a Pruitt Carotid Shunt.
Statistics
Data were recorded and tabulated in a Microsoft Excel (Microsoft Corporation, Redmond, Washington) database. Preoperative results are presented as mean ± standard deviation (SD) or median with range for continuous variables, while categorical ones are presented as number (percentage). The homogeneity of the 2 groups was evaluated by Mann-Whitney U test or Kruskal-Wallis test (for continuous variables) or by χ2 or Fisher exact test (in case of dichotomous variables). The association between potential medical or surgical risk factors and postoperative neurological morbidity was assessed first by univariate methods and then by stepwise multivariate logistic regression analysis if applicable (≥2 variables with significant P). A P value <.05 was considered statistically significant. Statistical analysis was performed with dedicated software (Epi Info 7.1.5; CDC, Atlanta, Georgia, or StatView 5.0; SAS Institute Inc, Cary, North Carolina).
Results
During the 7-year period of the study, 2029 patients underwent CEA in our center. Among these, 138 consecutive patients who presented with AIS related to an SCS and underwent early CEA in our institution were included into the analysis. Mean age at the time of stroke was 73.14 years (SD: 8.93). Of 138, 101 (73.2%) were male. The median time between clinical onset of the cerebral ischemic event and surgery was 9 days (range: 0-89 days). Eighty-three (60.14%) patients were operated within the first 14 days, whereas 55 (39.86%) of the 138 patients were operated beyond that time frame because of late admission to our institution, neurological instability, associated brain hemorrhage, or large volume cerebral infarcts. One hundred twenty-six (91.3%) patients presented with a severe carotid stenosis >70% NASCET, while 12 (8.7%) had a >50% stenosis. Thirty (21.7%) patients had a contralateral severe >70% NASCET carotid stenosis or occlusion. The presence of a contralateral severe carotid stenosis was never associated with a significant vertebral disease. Fifty-nine (42.8%) patients had a noncompetent circle of Willis. Median preoperative NIHSS was 1.5 (range: 0-11). Proper shunt functioning, as well as cerebral perfusion, was verified during each surgical procedure with TCD in 81 (58.7%) cases and with NIRS in 57 (41.3%). Mean carotid cross-clamping time (obtained by adding the duration of the clamping necessary for the insertion of the shunt + the time required to remove the shunt and to finalize the anastomosis) was 363.83 (173.75) seconds.
Ninety (65.2%) patients presented a TS of carotid origin and were subsequently included in group 1, while 48 (34.8%) of the 138 patients had a WS related to an SCS and were included in group 2. The agreement between the vascular neurologist and the neuroradiologist regarding the classification in group 1 versus group 2 was 91.3%. Thus, a second evaluation performed by a blinded vascular neurologist was needed in 12 (8.7%) of the 138 cases. Clinical baseline characteristics of the 2 groups are presented in Table 1. The 2 groups were statistically homogeneous for age, sex, degree of stenosis, presence of a contralateral severe carotid stenosis or occlusion, presence of a noncompetent circle of Willis, stenosis location (right vs left side), risk factors (use of antiplatelet drugs, hypertension, smoking, atrial fibrillation, diabetes mellitus, and dyslipidemia), preoperative NIHSS score, use of cerebral perfusion monitoring device (TCD vs NIRS), carotid cross-clamping duration, and delay between the onset of symptoms and surgery. The presence of CAD occurred more frequently in the WS group (33.3% vs 15.6%, P = .02). This analysis is summarized in Table 1.
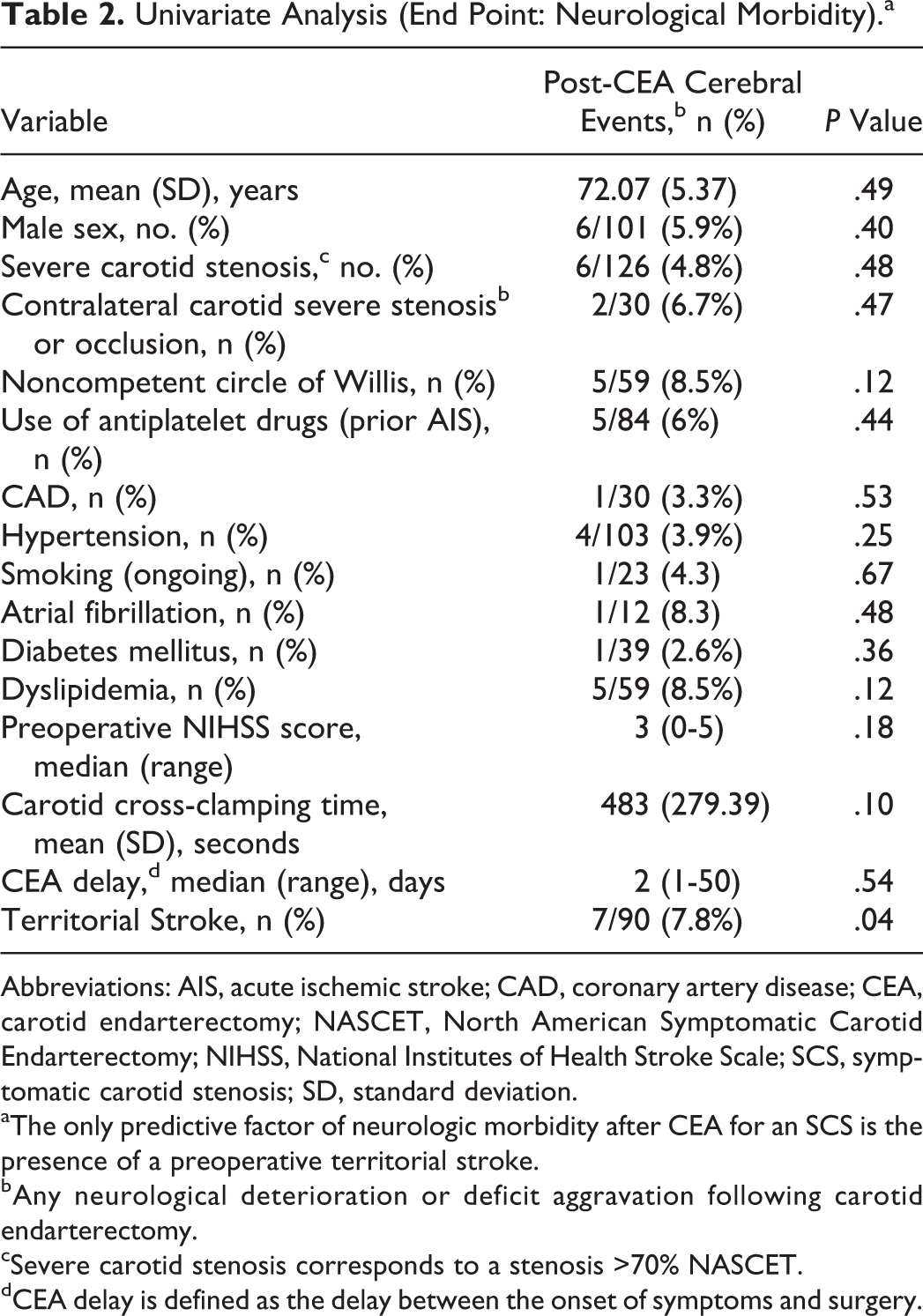
Postoperative mortality was 0%. Seven (5.1%) patients had an aggravation of the neurological status during the postoperative period, of which 2 presented a complete regression of the symptoms in less than 1 hour. So, the definitive postoperative neurological morbidity was 3.6% (5 of the 138). Postoperative neurological morbidity rate was significantly higher in the TS group (7 of 90; 7.8%) compared to the WS group (0 of 48), in which no postoperative aggravation of the neurological status occurred (P = .04). Definitive postoperative neurological morbidity rate in the TS group was 5.6% (5 of 90). No other predictive factor of neurologic morbidity after CEA for an SCS was found in univariate analysis (Table 2). Since only 1 variable (ie, the presence of a preoperative TS) had a P value <.05 on univariate analysis (end point: neurologic morbidity), a multivariate analysis was not performed.
Univariate Analysis (End Point: Neurological Morbidity).a
Abbreviations: AIS, acute ischemic stroke; CAD, coronary artery disease; CEA, carotid endarterectomy; NASCET, North American Symptomatic Carotid Endarterectomy; NIHSS, National Institutes of Health Stroke Scale; SCS, symptomatic carotid stenosis; SD, standard deviation.
aThe only predictive factor of neurologic morbidity after CEA for an SCS is the presence of a preoperative territorial stroke.
bAny neurological deterioration or deficit aggravation following carotid endarterectomy.
cSevere carotid stenosis corresponds to a stenosis >70% NASCET.
dCEA delay is defined as the delay between the onset of symptoms and surgery.
Discussion
Stroke is the fourth leading cause of death in the United States after heart disease, cancer, and chronic lower respiratory diseases. 18,19 However, it represents the principal cause of disability in Western countries. 14
Watershed stroke involve the junction of the distal field of 2 nonanastomosing arterial systems. 20 Their incidence is often underestimated: In autopsy series, WS represents approximately 10% of all ischemic strokes, 6 but more recent imaging studies in patients with internal carotid artery stenosis report an incidence between 19% and 64%. 2,5 While TS have a well-known embolic origin, the pathogenesis of WS remains debated despite numerous studies dedicated to the latter. 5 Several experimental studies have found an association between WS and microemboli arising from unstable carotid plaques, suggesting that small thrombi travel preferentially toward junctional areas. 5,6,20 -23 However, clinical studies supporting this hypothesis remain scarce, so the most consensual mechanism remains the hemodynamic failure due to hypotension in the presence of a severe ipsilateral carotid stenosis (low-flow mechanism). 24 -26
Large randomized control trials have shown that CEA is the most effective treatment in preventing cerebrovascular events in recently symptomatic severe carotid stenosis. 12,27 -29 However, the outcome of CEA in relation to the topographic patterns and the mechanism of the cerebral ischemia (embolic vs hemodynamic) has been analyzed in only 1 paper so far. 2 This French study showed that WS, compared to TS, were associated with a higher complication rate during the postoperative period of CEA performed after an AIS, concluding that it is mandatory to define the best treatment modality for this subgroup of patients in order to reduce associated procedural complications. Specifically, the role of CEA with routine shunting must be evaluated. In fact, this point was a limitation for the study. A very few shunts were inserted (9% rate), and the authors used the stump pressure method for selective shunting, which is known to be have a high false-negative rate, 30 since there may still be cerebral territories relatively hypoperfused.
It is assumable that a prolonged carotid cross-clamping time may enhance the ischemic damage of the so-called watershed territories. This is probably the reason why in the French experience the rate of postoperative strokes in the WS group was higher. In our center, carotid shunting is routinely performed, so we decided to retrospectively analyze our records and compare our experience with the French one. These results are summarized in Table 3. There are 2 main differences, in addition to the carotid cross-clamping time. First, in our center, all cases underwent shunt positioning as compared to only 9% of the French study. 2 Second, having said that—in both studies—WS represented approximately the 35% of the population and postoperative mortality was 0%, the complication rate in the 2 patient groups (WS vs TS) was exactly the opposite. In fact, we recorded a 0% neurological morbidity in the WS group when compared to 22% reported by the French study. By contrast, we experienced a higher rate of neurological complications in the TS group (7.8% vs 2%).
Comparison of the Results of our Experience and the French Experience.
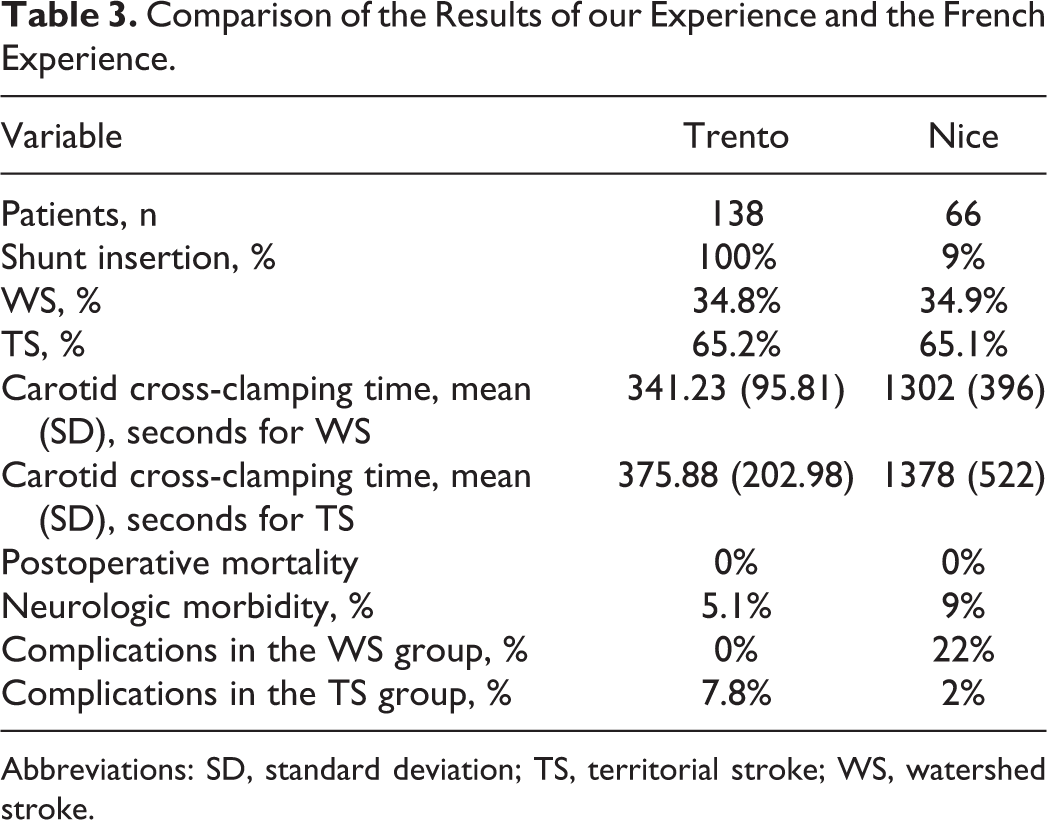
Abbreviations: SD, standard deviation; TS, territorial stroke; WS, watershed stroke.
The low neurological morbidity in our series suggests that routine shunting could play a protective role in acute WS. Although further studies comparing outcomes of patients with and without shunt use are required to better define the best treatment modality for AIS, we suggest to consider shunting in this subset of patients.
In our experience, the insertion of the shunt takes approximately 2 or 3 minutes. After cerebral blood flow is restored, CEA is accurately performed and reimplantation is started. Two to 3 additional minutes of cross-clamping are required to remove the shunt and to finalize the anastomosis, which leads to a mean total carotid cross-clamping time of approximately 6 minutes. The risk of postoperative neurologic deficits is higher after 9 minutes of cerebral ischemia, as reported by some authors. 31 Proper functioning of the shunt was systematically checked with TCD or NIRS in case of unsuccessful insonation of the transtemporal window. 32 Carotid cross-clamping duration was the same in groups 1 and 2, and it did not represent a predictive factor of neurologic morbidity. This, in our opinion, should corroborate the hypothesis that a prolonged cross-clamping time could be a risk factor for patients with acute WS. In fact, mean carotid cross-clamping time was >20 minutes in the French experience (Table 3). 2
According to the recent literature, CEA is recommended within the first 14 days for patients with AIS who presented with regressive or fixed neurologic deficit >6 hours’ duration once their condition has been stabilized, 12,33 while operative risk remains high for emergency endarterectomy for stroke-in-evolution or associated brain hemorrhage. 34 For these reasons, we decided to include in this study only neurologically stable patients, regardless of the time at which they reached a stability. Anyway, more than 60% of this population underwent CEA within 14 days of symptoms. We chose the “90 days” cutoff for considering a carotid stenosis as symptomatic or not and not the 6-month period reported by the European Carotid Surgery Trial Multicentre Randomized Controlled Trial eligibility methods, 35 according to the most recent neurological literature reporting that, after 3 months, the cumulative risk of stroke after a TIA or minor stroke reaches its maximum (17.3% and 18.5%, respectively). 36
Groups 1 and 2 were statistically homogeneous for age, sex, degree of stenosis, presence of a contralateral severe carotid stenosis or occlusion, presence of a noncompetent circle of Willis, cardiovascular risk factors, preoperative NIHSS score, carotid cross-clamping duration, and delay between the onset of symptoms and surgery. Only the presence of CAD occurred more frequently in the WS group than in the TS group (33.3% vs 15.6%, P = .02). This is probably related to the hemodynamic mechanism of this subgroup of strokes.
Despite the potential limitations related to the fact that data were analyzed retrospectively, the present study analyzes for the first time the outcomes of CEA with routine shunting based upon the topographic patterns of the AIS on MRI, paving the way for future, randomized trials. Another potential pitfall is that the role of carotid stenting (CAS) in this patient subgroup was not investigated. This is because CAS for SCS is not customary in our service, and—more relevantly—it is proved to be less cost-effective than CEA. 37 It must be observed that we performed only 1 type of CEA closure technique (eversion endarterectomy), so no data are available on a comparison between different closure approaches; however, in the French experience, the difference in the rate of postoperative neurologic morbidity in the eversion group versus the patch closure technique group was not statistically significant, even according to the topographic pattern of the AIS. 2 Finally, the role of shunting in TS should be better defined in subsequent studies, in order to clarify whether shunt insertion per se is a risk factor in this group of patients or neurologic morbidity is not related to this maneuver.
In this study, TS are associated with a higher post-CEA neurological complication rate when compared to WS (7.8% vs 0%, P < .05). TS was the only predictive factor of neurologic morbidity after CEA for an SCS, while outcomes do not seem to be affected by gender, cardiovascular risk factors, contralateral carotid stenosis/occlusion, presence of a noncompetent circle of Willis, NIHSS score, or age. Although WS are reported to be associated with the occlusion of the contralateral carotid artery or with an incomplete circle of Willis, 38,39 in our study, outcomes do not seem to be affected by these factors, similar to that described by Jean-Baptiste et al. 2
It is reasonable to assume that a personal history of preoperative WS indicates a compromised cerebral vascularization (both anatomic and hemodynamic), and therefore, we suggest to consider systematic carotid shunting during CEA, regardless of the presence of a healthy contralateral carotid artery or competent circle of Willis.
Conclusions
Current literature on acute WS undergoing CEA is extremely scant. In this study, routine shunting during CEA demonstrated to be a safe and efficacious technique associated with low procedural complications in patients with acute WS (0% complications). Postoperative complication rate is still relevant in patients who had acute TS caused by an unstable carotid plaque (7.8% transient and 5.6% definitive postoperative neurologic morbidity).
Our results encourage the use of routine shunting in case of acute WS as it is likely to play a protective role. Further studies are eagerly awaited to better define the timing and the best treatment option for both acute WS and TS related to an SCS in order to reduce postoperative neurologic morbidity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.