
Abstract
Vascular blowout syndrome (VBOS) secondary to neoplastic erosion is a dreadful complication of advanced stage malignancies that can compromise quality of life and overall prognosis in a fragile patient population. Endovascular therapy can offer minimally invasive, life-saving maneuvers both acutely and prophylactically. Four patients with end-stage malignancies eroding into various peripheral vascular beds with impending, threatened, and acute VBOS underwent successful endovascular management. Technical success was achieved in all patients with no perioperative morbidity or mortality. In all patients, endovascular intervention controlled life-threatening hemorrhage and facilitated adjunctive therapeutic modalities such as surgical tumor debulking and/or chemoradiation. In conclusion, our small case series demonstrates that endovascular therapy can offer safe and effective palliation of peripheral VBOS secondary to neoplastic erosion.
Introduction
Vascular blowout syndrome (VBOS) is a well-known, life-threatening condition most commonly reported in advanced-stage head and neck malignancies abutting the cervical carotid circulation. 1 –10 Three primary categories of VBOS exist depending on the extent of tumor invasion. The classifications include threatened, impending, and acute vascular blowout. 5 Threatened blowout is defined as tumor encasement of a vessel; impending blowout includes bleeds that can be controlled by conservative nonoperative measures; and acute blowout describes cases with life-threatening hemorrhage. 6
Within current literature, therapeutic techniques described have mostly included salvage urgent or emergent surgery to control life-threatening hemorrhage with or without extra-anatomic vascular reconstruction. These are major undertakings in a frail, often moribund patient population with poor wound healing potential. 9 Surgical intervention may also delay initiation of adjunctive palliative chemoradiation until surgical wound healing is achieved. Furthermore, the invasive nature of these operations prompts the surgeon to defer intervention until an emergent, life-threatening situation arises which further complicates the operation and increases complication risks. Prophylactic measures are, therefore, rarely taken to minimize or eliminate VBOS-related life-threatening hemorrhage. Endovascular therapy can offer a safe, effective, durable, and less invasive treatment option that not only offers emergent treatment of life-threatening hemorrhage and end-organ malperfusion but can also serve as an important prophylactic measure in threatened and impending blowout. 6,11,12 Herein, we describe four unique cases of peripheral VBOS associated with advanced-stage malignancies that showcase the versatility and efficacy of endovascular therapy as an important palliative measure in this high-risk patient population. Verbal consent was obtained from all patients.
Case Reports
Case 1
A 50-year-old man with a history of pleomorphic, undifferentiated sarcoma of the neck initially underwent surgical tumor resection and external beam radiation. Three years later, local recurrence with lung metastases was detected, which were surgically excised. Follow-up imaging revealed recurrent lung and thyroid metastases and circumferential tumor encasement of the left common carotid artery (CCA) with complete occlusion of the external carotid circulation with delayed transcollateral contrast enhancement. The patient did not report any neurologic symptoms at this time. Palliative care was recommended, and vascular surgery was consulted for management of a threatened carotid blowout syndrome. The patient presented to the hospital with multiple bouts of life-threatening hemorrhage from the tumor requiring massive transfusion and nonoperative compressive measures for temporary hemostasis. Vascular surgery consult was obtained as the oncological surgical team deemed the tumor inoperable and recommended palliative end-of-life measures. Computed-tomography angiography was performed demonstrating impending blowout of the left CCA (Figure 1A and B). Furthermore, selective left subclavian angiography demonstrated hemorrhagic source from the ascending pharyngeal branch of the left thyrocervical trunk (Figure 1C). The left carotid blowout was addressed by deployment of a Gore Viabahn self-expanding covered stent across the involved segment. Superselective microcatheterization of the ascending pharyngeal source of hemorrhage was performed with embolization using N-butyl cyanoacrylate (Figure 1D). Prompt cessation of hemorrhage was obtained with no further bleeding or neurological complication. Patient was discharged to hospice care and expired 6 months thereafter from neoplastic burden with no further hemorrhagic episodes or hospitalization.
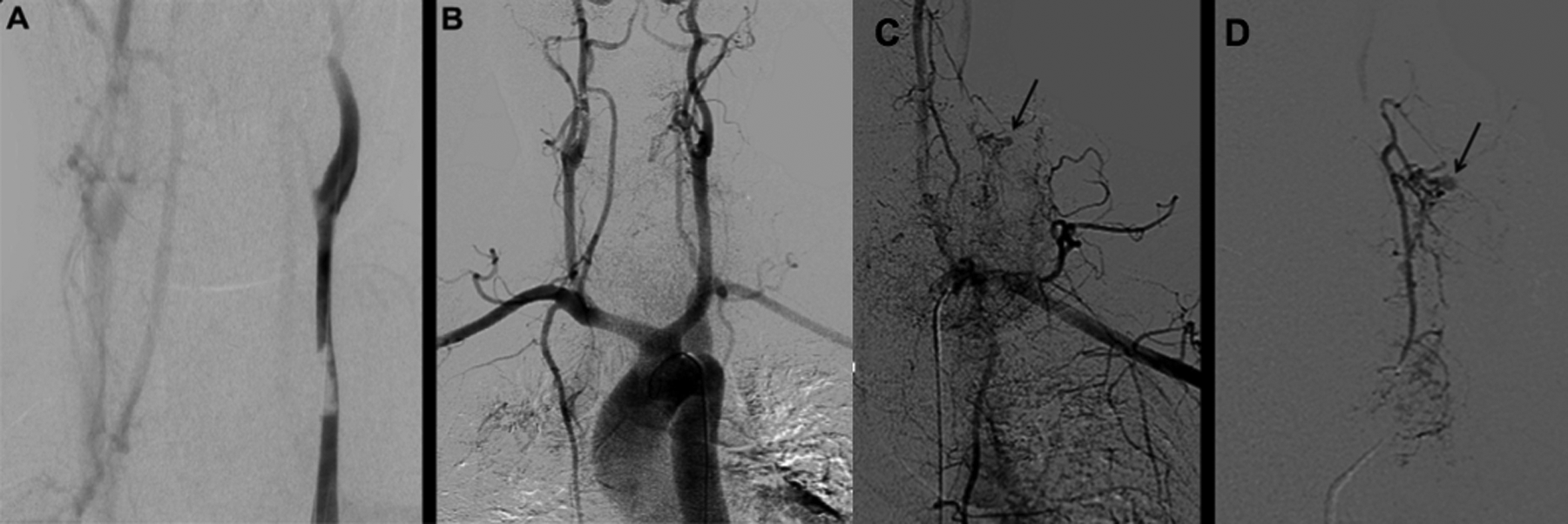
A, Venous-phase cervicocerebral angiography showing delayed clearance of contrast through a threatened left common carotid artery, with near occlusion from tumor encroachment. Note the absence of ipsilateral internal jugular vein filling. B, Completion arch aortography after common carotid artery stent deployment showing improved antegrade flow with no evidence of tumor encroachment. C and D, Selective left subclavian arteriography reveals tumor location, as well as a 3-mm pseudoaneurysm identified and marked by arrows on superselective angiography of the subclavian artery (C) and the thyrocervical trunk (D).
Case 2
A 50-year-old woman with a history of recurrent malignant vulvar squamous cell carcinoma, status post her third cycle of palliative chemotherapy, was referred to vascular surgery for evaluation concerning an exophytic, fungating, neoplastic mass (Figure 2A) in the left groin region with complete encasement of the common femoral artery (CFA), superficial femoral artery (SFA), and profunda femoral artery (PFA) on computed tomography. The mass was hypervascular on contrast-enhanced imaging, and extensive metastatic spread to regional lymph nodes was noted. The mass was complicated by recurrent bouts of hemorrhage requiring multiple hospital admissions and frequent blood transfusions. Given the juxtaposition to adjacent major vessels, palliative surgical excision would have required extensive dissection and major vascular reconstruction. Furthermore, patient was due to undergo palliative chemoradiation which would have been delayed had major surgical intervention been offered to minimize wound-related complications. Therefore, decision was made to proceed with angiographic evaluation of the lesion with plans for concomitant palliative therapy if amenable. Selective angiography revealed a hypervascular tumor with multiple feeding branches from the anterior branches of the ipsilateral internal iliac artery (Figure 2B). These were superselectively catheterized with a coaxial microcatheter system and bland embolization with embospheres performed with significant devascularization of the tumor (Figure 2C). Next, 2 ATRIUM iCAST balloon expandable covered stents (ATRIUM Maquet Getinge Group, Hudson, New Hampshire) (5 × 16 mm and 6 × 22 mm) were deployed in the PFA and SFA (Figure 2D). The CFA was stented with a Gore Viabahn self-expanding covered stent, the distal end of which was flowered open into the femoral bifurcation so as to accommodate flow into the stented PFA and SFA.
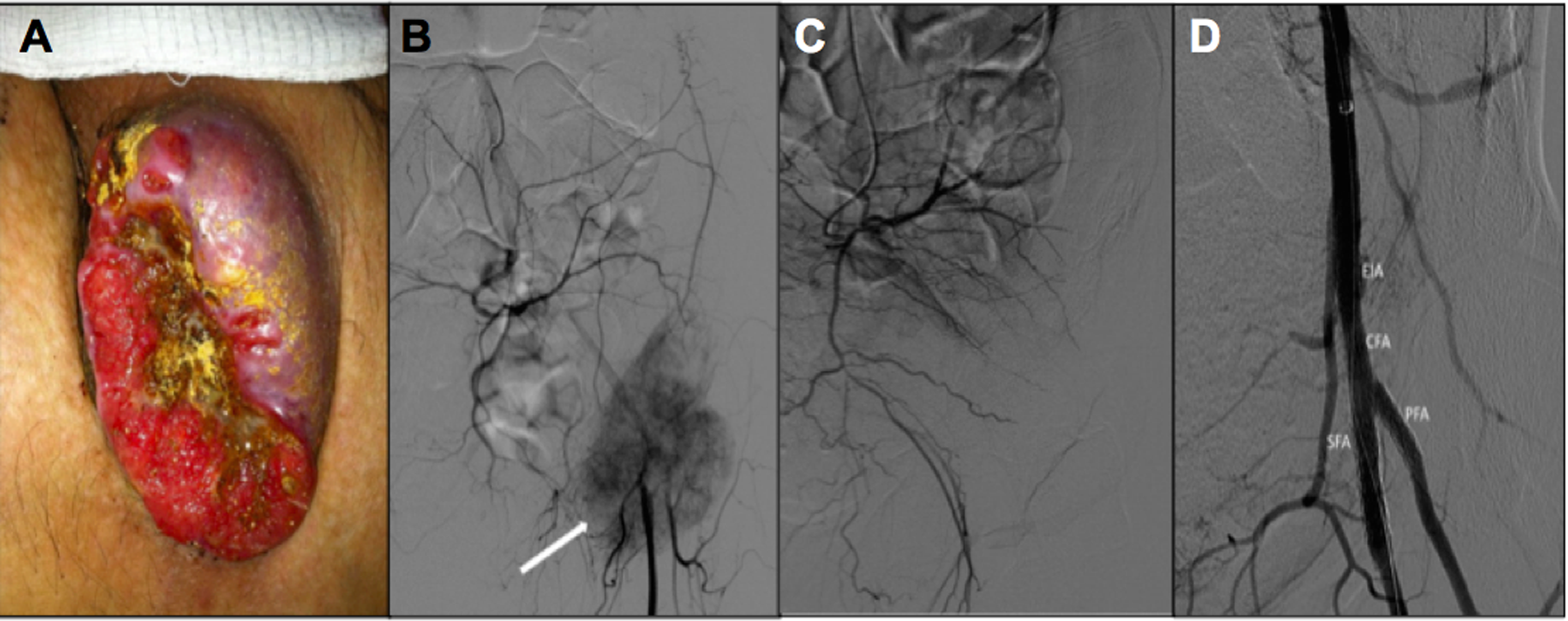
A, Fungating, exophytic neoplastic mass of the left groin complicated by recurrent bouts of hemorrhage requiring hospitalization and transfusion. B, Diagnostic left lower extremity angiogram demonstrating a hypervascular mass abutting the left femoral bifurcation. Note circumferential encasement of the femoral bifurcation with impingement on the arterial lumen. C, Postembolization angiography reveals excellent devascularization of the tumor without evidence of nontarget embolization. D, Poststent angiography reveals excellent revascularization of compromised femoral arterial patency with no evidence of arterial injury and excellent tumor devascularization.
There were no perioperative complications. All hemorrhage ceased postoperatively. There were no further blood transfusion requirements, and patient was successfully initiated on adjunctive chemoradiation on postoperative day one. At 1-year follow-up, she had maintained patency of the vascular stents with no hemorrhagic recurrence.
Case 3
A 57-year-old male with an unremarkable past medical history significant presented to the emergency department with complaints of acute onset left lateral thigh and buttock claudication and paresthesias in the setting of acute kidney injury. Magnetic resonance imaging revealed a large mass extending into the left psoas with complete encasement of the left distal common iliac artery with possible hematoma and ureteral obstruction causing postrenal azotemia (Figure 3A–C). An impending vascular blowout was suspected secondary to a large retroperitoneal sarcoma. Vascular surgery consult was obtained. A decision was made to proceed with angiographic interrogation. Aortoiliac angiography revealed blowout of the left distal common iliac artery with active hemorrhage and pseudoaneurysm formation (Figure 3D). Retrograde wire and catheter access was obtained, and a self-expanding covered stent was deployed from the aortic bifurcation into the proximal external iliac artery with complete cessation of hemorrhage and control of the pseudoaneurysm (Figure 3E). Ankle brachial indices and pulse examination had normalized postoperatively with alleviation of presenting symptoms. Patient subsequently underwent decompressive ureteral stenting and staged exploratory laparotomy for palliative surgical debulking of what turned out to be a large retroperitoneal spindle cell carcinoma. The presence of previously deployed covered stent facilitated identification of eroded vasculature during the debulking procedure and prevented further vascular compromise. Patient expired 3 months after surgery from neoplastic burden without any further hemorrhagic or ischemic episodes.
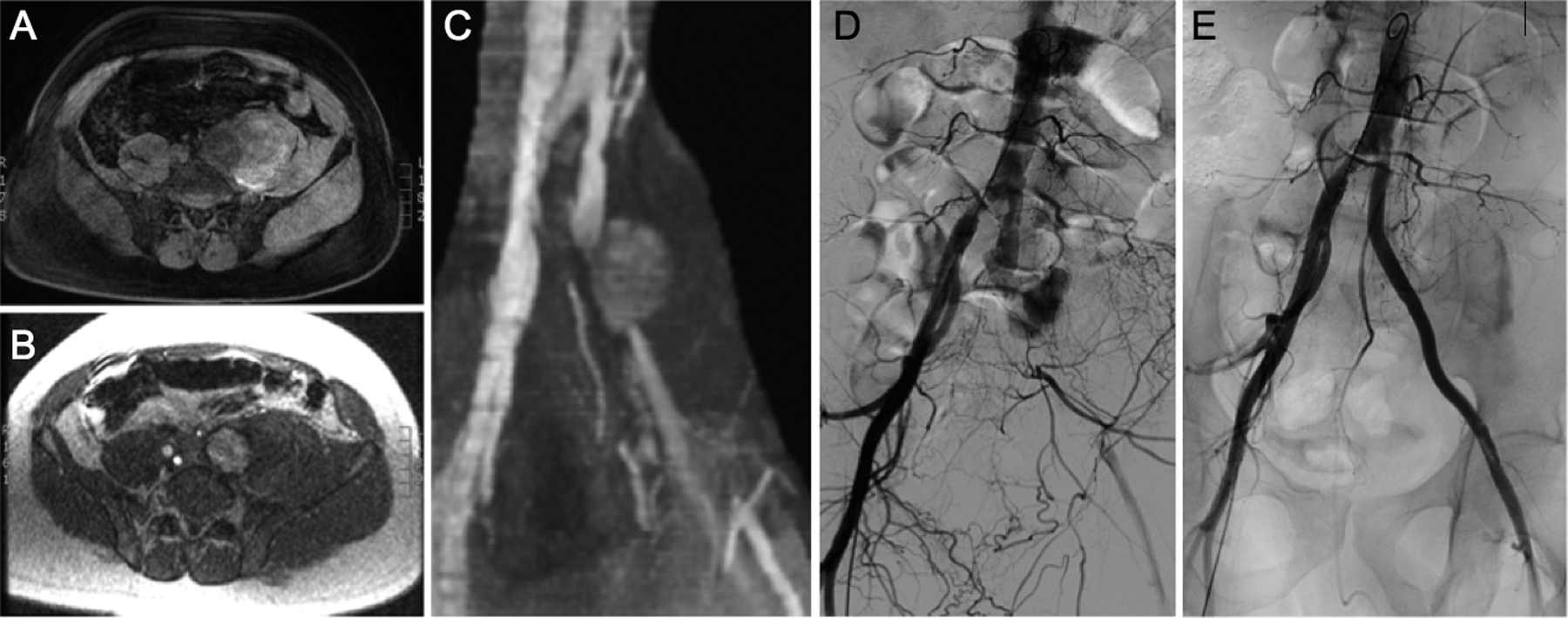
A-E, Retroperitoneal sarcoma causing acute blowout of the left common iliac artery with distal ischemia. Diagnostic angiogram shows tamponaded pseudoaneurysm, which was crossed and re-lined with a self-expanding covered stent with reinstitution of unobstructed distal flow and arterial integrity.
Case 4
A 62-year-old male with an aggressive basal cell carcinoma of the left supraclavicular region status post prior surgical excision with major pedicled myocutaneous reconstruction was recommended to undergo local palliative radiation for management of local recurrence. The recurrent tumor had completely encased the left subclavian artery and caused chronic brachial plexopathy with profound ipsilateral upper extremity motor and sensory deficits. The oncology team had deferred further radiation secondary to concerns regarding subclavian artery blowout and life-threatening hemorrhage. Patient presented to the emergency room with new onset hemorrhage requiring blood transfusion. A CT scan was obtained confirming impending blowout of the left subclavian artery (Figure 4A). Extensive postradiation local anatomical distortion was present. Retrograde percutaneous catheterization of the left proximal subclavian artery was performed, and tumor encasement of the subclavian artery was confirmed from just distal to the left vertebral artery extending into the dorsal scapular branches. The affected region was stented with a self-expanding covered stent and angioplasty to desired diameter (Figure 4B and C). There were no perioperative complications. All hemorrhage ceased postoperatively and patient was now able to undergo adjunctive local radiation for tumor palliation. He subsequently presented 3 months following stenting with an exposed covered stent and septicemia (Figure 4D). The stent had nevertheless prevented life-threatening blowout of the subclavian artery during radiation and had proven a life-saving maneuver. Patient underwent successful resection of the exposed stent with ligation of the subclavian artery. Revascularization was not offered, given the chronic motor and sensory deficit from prior brachial plexopathy. Patient eventually required forearm amputation secondary to ischemia, which he tolerated well, and is currently undergoing supraclavicular wound care (Figure 4E).
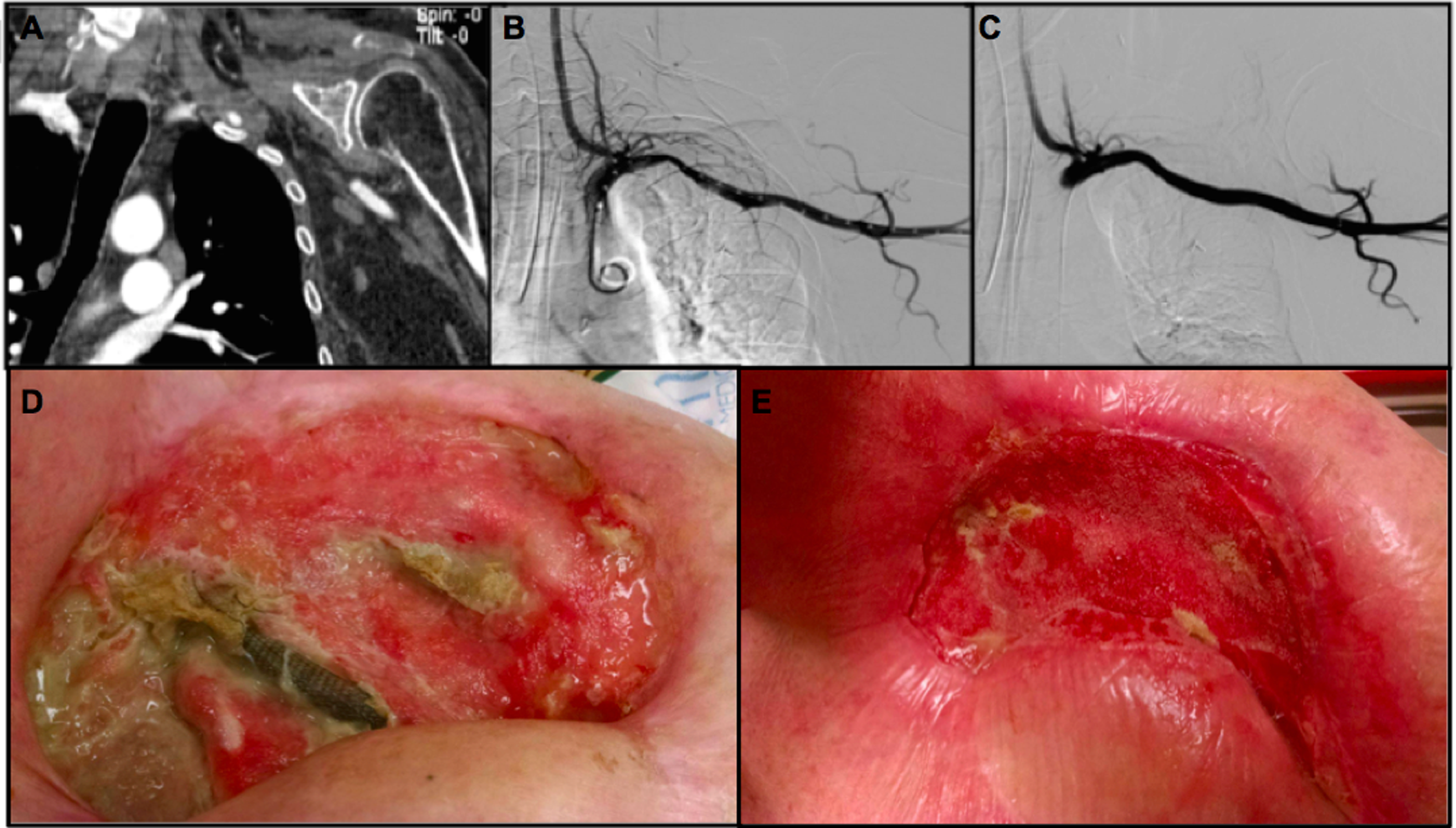
A-E, Supraclavicular tumor with threatened blowout of the subclavian artery. Retrograde transbrachial approach confirms tumor encasement. The artery was re-lined with self-expanding covered stent and integrity was restored. This allowed the patient to undergo adjunctive local radiotherapy, which led to further erosion. However, presence of a covered stent previously placed prevented life-threatening blowout. The exposed stent was removed, and wound healing locally was achieved over the course of the subsequent 3 months.
Discussion
First described by Borsany in 1962, VBOS of the carotid circulation is a dreaded and well-described complication of end-stage head and neck malignancies. 2,13,14 Estimates of cumulative mortality reach 40% with an associated major neurological morbidity of approximately 60%. 5 This entity, however, is rarely reported in the peripheral circulation. In a few case reports encountered, management has been mostly surgical and consisted of direct reconstruction with autogenous or synthetic interposition grafting or bypass with or without flap coverage. 8 These procedures have proven extremely difficult with limited success owing to a hostile anatomy from previous radiation and/or radical dissections. 3
Endovascular techniques have been rarely reported as the primary palliative option in management of VBOS despite a low-risk profile and the precise diagnostic and therapeutic options they provide. 15 –17 The significantly reduced perioperative morbidity associated with a purely endovascular approach is highly desirable and preferred over complex surgical reconstruction, especially within this frail patient population. Techniques such as superselective tumor embolization and refined stenting techniques via low-profile, balloon-expandable, and self-expanding covered stents offer durable, life-saving benefits to this frail and moribund patient population with minimal perioperative morbidity.
The first case presented describes an impending carotid VBOS in the setting of an inoperable neck sarcoma deemed unsuitable for surgical debulking. Covered stenting of the carotid artery halted further erosion and prevented life-threatening hemorrhage and stroke-related morbidity. Furthermore, superselective tumor embolization provided a minimally invasive means for acute control of life-threatening hemorrhage.
In the second case described, a purely endovascular approach minimized postoperative wound burden that would have delayed adjunctive chemoradiation secondary to concerns for wound-related complications. Tumor embolization controlled recurrent, life-threatening hemorrhage and prevented future hospital readmissions and transfusion requirements—a cost-lowering benefit. Furthermore, covered stent revascularization of a threatened VBOS of the femoral bifurcation halted further tumor erosion and likely prevented major limb amputation.
Case 3 presents an impending blowout of the left iliac artery with ipsilateral limb ischemia, both of which were immediately addressed in a minimally invasive fashion via covered stent revascularization. This procedure served as a bridge to more definitive surgical debulking therapy. Furthermore, presence of a covered stent served as a useful intraoperative landmark, which helped minimize further vascular injury, given the tumor-mediated local anatomical distortion. This resembles preoperative ureteral stent placement in major abdominal or pelvic surgeries.
In the last case, a minimally invasive endovascular revascularization of an impending left subclavian artery blowout facilitated adjunctive palliative radiation and prevented life-threatening hemorrhage secondary to radiation-induced erosion. It eventually required excision due to infectious complications but proved to be a life-saving maneuver that maximized the prognosis in this terminal cancer patient.
When employing these palliative techniques, the surgeon must be aware of the temporizing nature and related infectious complications inherent to the process of continued tumor erosion. It is worth emphasizing that the main goal of these techniques is to prevent life-threatening, blowout-related hemorrhage. The patient’s clinical status and prognosis permitting, one may consider explant of the exposed grafts if a severe infectious burden is encountered. Revascularization of the affected organ may or may not be indicated, depending on patient’s quality of life and risks of bypass surgery. A tailored approach to each patient’s unique condition and close collaboration with oncologic colleagues is advisable.
Conclusion
Awareness of VBOS as a life-threatening condition associated with advanced stage malignancies and the availability of safe, effective, and minimally invasive endovascular techniques is important for palliation and overall quality-of-life improvement in this fragile patient population. Multiple transcatheter techniques are available and should be within the arsenal of all vascular surgeons managing these difficult clinical scenarios.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.