
Abstract
Background:
Neurological adverse events with spinal cord ischemia (SCI) remain one of the most feared complications in patients undergoing thoracic endovascular aortic repair (TEVAR). These patients can develop irreversible paraplegia with lifelong consequences with physical and psychological agony.
Case Presentation:
We herein present a patient who developed SCI with bilateral lower leg paraplegia on the third postoperative day following TEVAR. Spinal catheter was inserted for spinal fluid drainage. A hyperbaric oxygen therapy was initiated for 90 minutes for 2 days, which was followed by therapeutic hypothermia for 24 hours with a target temperature of 33°C. The patient exhibited significant neurological recovery following these treatments, and he ultimately regained full neurological function without spinal deficit.
Discussion:
This represents the first reported case of full neurological recovery of a patient who developed complete SCI following TEVAR procedure. The neurological recovery was due in part to immediate therapeutic hypothermia and hyperbaric oxygen therapy which reversed the spinal ischemia.
Keywords
Introduction
Spinal cord ischemia (SCI) is one of the most feared complications in patients undergoing open surgical repair for thoracic aortic aneurysm. Although recent advances in endovascular technology have demonstrated the efficacy and durability of thoracic endovascular aortic aneurysm repair (TEVAR), the incidence of SCI following TEVAR remains a poorly predicted complication, with incidence ranging from 2% to 6%. 1 –3 For patients who had SCI following thoracic aneurysm repair, they are confronted with a lifelong challenge of disability and increased fatality. The present report describes a patient who underwent TEVAR and developed a delayed onset of SCI with lower extremity paralysis. Prompt interventions including hyperbaric oxygen (HBO) therapy and therapeutic hypothermia were instituted, which resulted in complete neurological recovery.
Case Report
A 73-year-old male with a surgical history of aortobifemoral bypass for aortoiliac artery aneurysm disease 15 years ago developed a 3-month history of back pain. Computed tomography angiogram revealed an 8.4-cm aortic aneurysm in the mid-descending thoracic aorta (Figure 1). Pertinent aortic morphology revealed a favorable anatomy for TEVAR as the aortic aneurysm originates 5 cm distal to the left subclavian and ends 3 cm above the celiac artery. An elective TEVAR was planned. Under general anesthesia, a spinal catheter for cerebrospinal fluid (CSF) drainage was inserted to maintain a pressure <10 cm H2O with no restriction on CSF drainage volume. Using a percutaneous technique, 2 Gore TAG endoprostheses (WL Gore, Flagstaff, Arizona) were deployed via a right femoral access, which successfully excluded the thoracic aortic aneurysm. The left subclavian artery and celiac artery were not covered by the thoracic endograft. Two intercostal arteries at the T8 and T9 levels were covered by the endograft. Completion angiogram showed successful exclusion of the aortic aneurysm without endoleak (Figure 2). The procedure was performed uneventfully with a total procedure time of 64 minutes and an estimated blood loss of 20 mL.
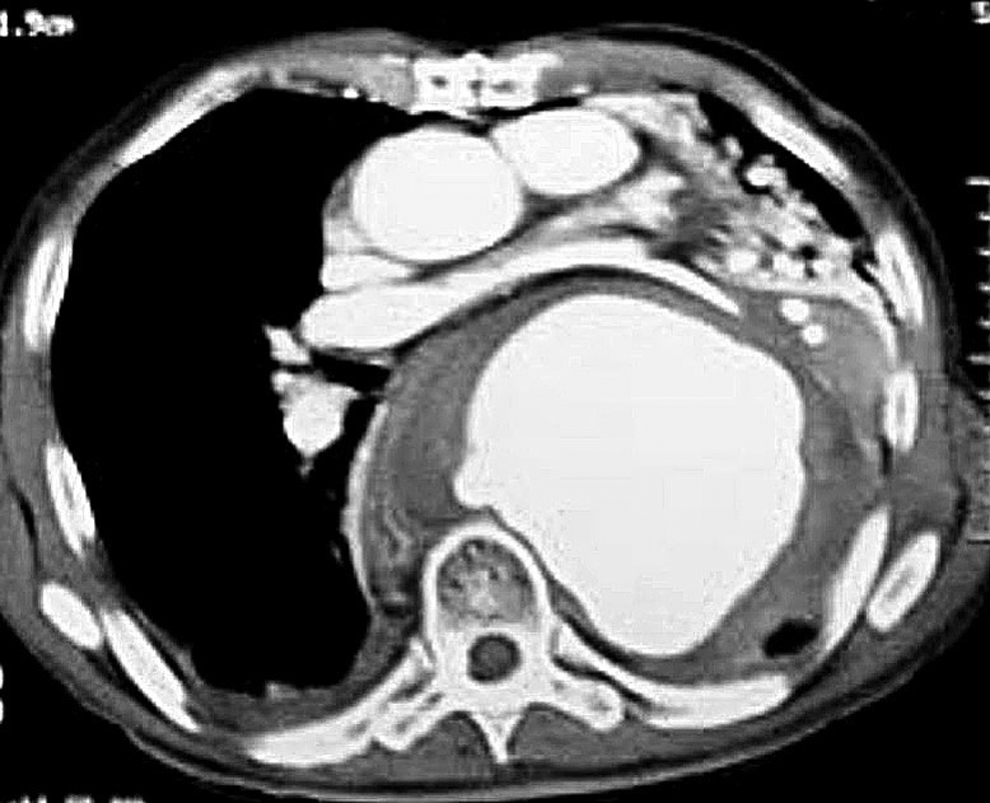
A preoperative computed tomography (CT) scan of the chest revealed an 8.4-cm descending thoracic aortic aneurysm.
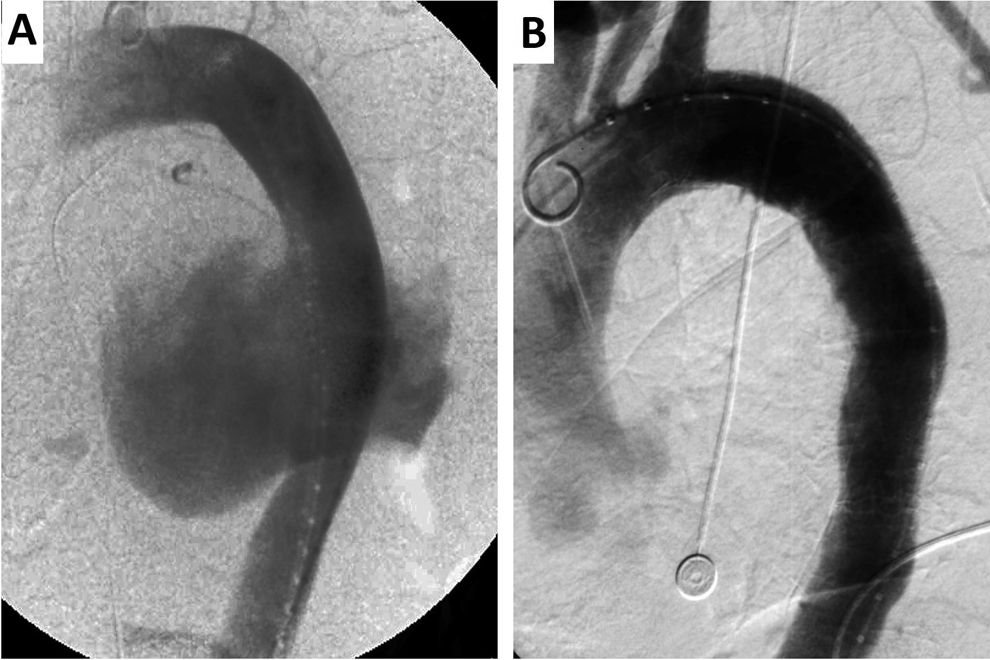
A, The descending thoracic aortic aneurysm was identified in an aortogram at the time of the thoracic endovascular aortic repair (TEVAR) procedure. B, Completion angiogram demonstrated successful endograft exclusion of the thoracic aortic aneurysm.
The patient remained both hemodynamically and neurologically stable following extubation. The spinal drain was removed on the morning of postoperative day 3, and he was able to ambulate without difficulty. On the evening of postoperative day 3, the patient developed bilateral lower leg paraplegia. With a diagnosis of SCI, a spinal catheter was inserted immediately for CSF drainage, which revealed an initial opening pressure of 23 cm H2O. Drainage of the CSF was maintained at a pressure of less than 10 cm H2O, while resuscitation efforts for blood pressure augmentation were kept to a mean arterial pressure of greater than 110 mm Hg. Immediate neurological consultations by 2 neurologists confirmed bilateral lower extremity paralysis, loss of pinprick and vibratory sensation caudal from the T7 level, and absence of the anal sphincter. Despite CSF drainage and hypertensive resuscitative efforts, the patient had minimal improvement with slight toe movement of the left leg. An urgent institutional review board approval was granted for HBO and therapeutic hypothermia treatment. Within 5 hours of the onset of SCI, HBO treatment was initiated for 90 minutes (monochamber unit with chamber pressure of 2.0 atmosphere and F
Discussion
Neurological complications such as SCI following TEVAR is a well-recognized and highly feared complication. Several risk factors have been identified for the development of SCI after TEVAR, which include intentional coverage of the left subclavian artery, preoperative renal failure, perioperative hypotension, prior abdominal aortic aneurysm repair, and greater proportion of aorta coverage (>20 cm). 1 –3 In our patient, his history of an aortobifemoral bypass represents a significant risk factor for SCI following TEVAR, a finding which we have validated previously. 2,4,5 Despite our efforts to reduce TEVAR-related neurological complications with preemptive CSF drainage catheter placement and blood pressure augmentation, our patient still developed SCI with paraplegia. Our report is notable because it represents the first case of SCI with eventual full neurological recovery using conventional resuscitative modalities plus HBO and therapeutic hypothermia.
Postsurgical SCI can be categorized as either acute onset (immediate or upon wakening) or delayed onset (occurring following a period of intact neurologic function). The etiology of the former category is likely due to hypoxic injury with hypoperfusion of the spinal cord, whereas the latter type of SCI is believed to be caused by either reperfusion injury after hypoperfusion or edema formation in the spinal cord. 6,7 The delayed onset of SCI in our patient may be caused in part by combined factors including his prior aortic reconstruction, hypoxic injury due to coverage of critical intercostal arteries, and possibly an exaggerated inflammatory insult manifested by his recent back pain.
Once neurological deficits occur due to SCI, treatments are primarily supportive with the aim to increase spinal perfusion pressure. This is generally achieved with CSF drainage to lower the spinal pressure while augmenting mean arterial pressure. The benefit of immediate systemic steroid to reduce spinal cord swelling has been advocated by some researchers, but its role remains controversial. 8,9 Clinical evidence of HBO or hypothermia in the management of SCI remains scarce. A recent report described a patient who underwent coil embolization of a vertebral artery due to cervical vertebral body metastasis, and the patient developed postprocedural stroke with lower extremity paralysis. 10 The patient underwent immediate arterial thrombolytic therapy to reestablish vertebral perfusion, which was followed by HBO and therapeutic hypothermic treatment. At 1-year follow-up, this patient had complete neurological recovery without residual deficit.
In both clinical literatures and animal studies, HBO therapy has sporadically demonstrated a beneficial role by decreasing the size of neurological ischemic region and cerebral infarcts. 11 –14 However, a recent randomized trial showed mixed outcome without improvement after the use of HBO in acute ischemic stroke. 15 In a feline cerebral stroke model, the benefit conferred by HBO treatment in neurological recovery was lost after 4 hours of middle cerebral artery occlusion. 16 The current literature provides little information regarding the utility of HBO as these reports were done with relatively small sample sizes and variable times from symptom onset of neurological deficit to treatment.
In a randomized study of 124 patients with acute ischemic stroke who were treated with either HBO or placebo control, the regression of neurological symptoms was markedly apparent in patients treated with HBO. 17 Additional benefit of poststroke pulmonary complications was noted in those patients exposed to HBO compared to the placebo control group. The benefit of HBO was also reported in a recent study by Lin and colleagues who evaluated 80 patients with spinal cord injury and found that HBO therapy resulted in a significant improvement in hypermyotonia and paralysis compared to the control group. 18 Similar benefit has also been reported in patients with acute traumatic spinal cord injury who experienced neurological improvement following HBO therapy. 19
Therapeutic hypothermia, in contrast, has received greater focus with proven benefits in improved outcome following cardiac arrest and neuroprotective role after acute ischemic injuries in both animal model and clinical investigations. 20 –23 Although the exact mechanism of how hypothermia may render a neuroprotective role remains to be elucidated in humans, investigation using animal models has suggested that hypothermia may suppress excitatory synaptic transmission and reduce neuronal inflammation and injury. 24 –27 In our patient, HBO and therapeutic hypothermia were instituted due in part to the lack of neurological improvement following the initial resuscitative effort. The decision of this multimodality treatment using HBO and therapeutic hypothermia was also based on the historically poor outcome of SCI. His immediate response to this treatment may be attributable to HBO and hypothermic treatment. His continual neurological improvement may be explained by the possibilities of neuronal reorganization, such as increased activation in secondary motor brain areas and spatial shift in neural plasticity or progenitor cell–induced spinal cord regeneration. These neuronal regenerative activities have been shown to occur in patients with SCI treated with intense rehabilitation program. 28,29
In conclusion, the remarkable recovery of our patient who exhibited a complete neurological function at 9 months following a devastating spinal cord ischemic injury underscores a potential therapeutic role of HBO and hypothermia in patients with SCI. Further investigation is warranted to validate the therapeutic role of these treatment modalities in the management of SCI.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.