
Abstract
Purpose:
Cyanoacrylate closure of the saphenous vein with the VenaSeal system is a new technique just approved on December 2016 in Korea. Therefore, there are seldom reports about postprocedural outcomes of VenaSeal system in Asian countries. We report the initial outcomes of VenaSeal system for the treatment of great saphenous veins (GSVs) and small saphenous veins (SSVs) as a first report in Korea.
Methods:
Thirty-four patients with incompetent saphenous veins (47 GSVs and 16 SSVs) were treated at a single session. Concomitant phlebectomy was performed in 15 (44.1%) of 34 patients. All procedures were started with local anesthesia with music therapy and switched to intravenous sedation if patient requested. Patients revisited the clinic on 10 days, 1 month, and 3 months after surgery. Postprocedural evaluations including numerical pain rating score, revised Venous Clinical Severity Scores (rVCSS), and Aberdeen Varicose Vein Questionnaires were checked. Duplex ultrasound was performed on 10 days, 1 month, and 3 months.
Results:
All treated veins (47 GSVs and 16 SSVs; 100%) had complete closure by duplex ultrasound during the follow-up period. Mean numerical pain rating scale of 6 hours after procedure was 2.7. The rVCSS was improved during the follow-up period. Phlebitis-like “abnormal skin reaction” in the treatment area was occurred in 8 (23.5%) of 34 patients and recovered fully in 2 weeks.
Conclusions:
Cyanoacrylate closure, VenaSeal system, is safe and effective for the treatment of incompetent saphenous veins.
Introduction
Chronic venous disease (CVD) is a common and progressive disease, leading to symptoms that disturb the patient’s quality of life. It was reported that 40% of females and 17% of males had CVD. Despite the high prevalence of CVD, most patients remain untreated. 1,2
Treatment of CVD has undergone wide-scale changes during the past several years. Previously, surgical stripping was the primary choice of treatment. However, it has been largely replaced by endothermal ablation, either with radiofrequency or laser energy. 3
Complications follow surgical stripping, including pain, bruising, paresthesia, and a high neovascularization rate. 4 –6 Endothermal ablation, either with radiofrequency or laser, showed improvements in patient recovery compared to surgical stripping. 7
However, a main disadvantage of these techniques is the requirement of tumescent anesthesia to reduce the risk of thermal injury to the surrounding structures. Tumescent anesthesia requires additional time and is also associated with adverse events (AEs), such as pain, hematoma, and ecchymosis. 6 –9
Recently, a new concept of treatment, cyanoacrylate closure (CAC), for CVD has been approved for treating the incompetent saphenous veins in many countries. The VenaSeal closure system, a new technique using CAC, received Conformité Européene mark in September 2011 and was approved by the Food and Drug Administration for closure of lower extremity superficial truncal veins in February 2015. 10
Several previous studies have demonstrated the safety and effectiveness of the VenaSeal system for the treatment of incompetent saphenous veins. 11 –15 Although other previous reports studied for the treatment of the great saphenous vein (GSV) alone, Gibson and Ferris reported multiple incompetent saphenous vein segments—including the anterior accessory great saphenous vein and small saphenous vein (SSV)—and also commented on the successful treatment of the epifacial GSV. 15
This study includes the patients with refluxing saphenous veins in epifacial GSV, below-knee GSV around ankle level, and SSV. There were no limitations on the vein diameter.
Method
In Korea, CAC for the treatment of incompetent saphenous veins was approved in November 2016 as a new technology and announced by the Ministry of Health and Welfare in December 2016. Between December 2016 and February 2017, 34 patients were enrolled and treated. This study was approved on 24 March 2017 by Korea National Institution for Bioethics Policy (approval number P01-201703-21-017) and conforms to the Declaration of Helsinki (1964, version Hong Kong, 1989).
Patients
Between December 2016 and February 2017, 34 patients with CVD underwent VenaSeal system at our clinic. All targeted veins for treatment needed to demonstrate at least 0.5 seconds of reflux in the standing position with a diameter of at least 3 mm (Table 1). The preoperative Clinical, Etiologic, Anatomic, Pathophysiologic (CEAP) classification was C1-C4 (C1: telangiectasia or reticular veins, C2: varicose veins, C3: edema, C4a: pigmentation or eczema, C4b: lipodermatosclerosis or atrophie blanche), and 5 patients with C1 classification were included who had symptoms such as aching, cramping, heaviness, tingling, and edema.
Baseline Characteristics of the Treated Population.
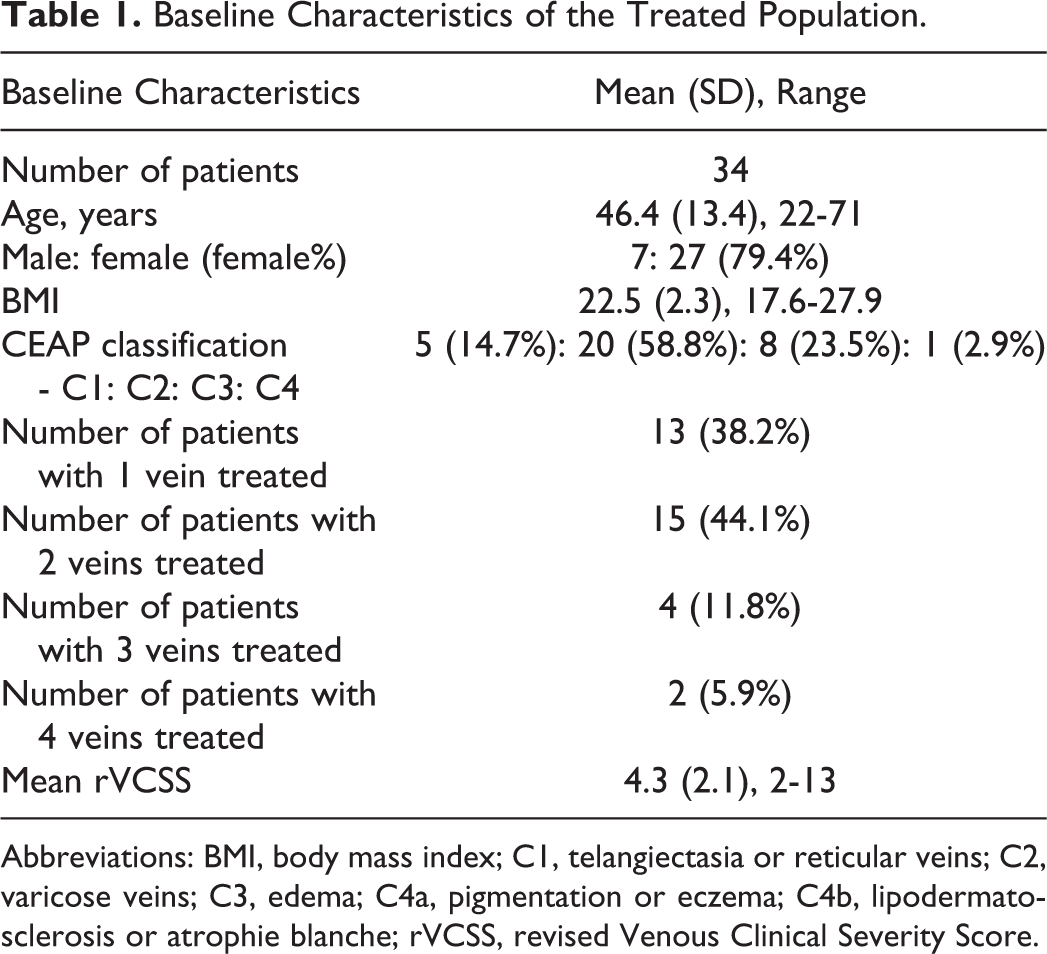
Abbreviations: BMI, body mass index; C1, telangiectasia or reticular veins; C2, varicose veins; C3, edema; C4a, pigmentation or eczema; C4b, lipodermatosclerosis or atrophie blanche; rVCSS, revised Venous Clinical Severity Score.
A total of 47 GSVs and 16 SSVs were treated. The mean size (mm) of the treated veins (TVs) was 8.0 ± 3.7 (3.1-18; Table 2.)
Treated Veins.
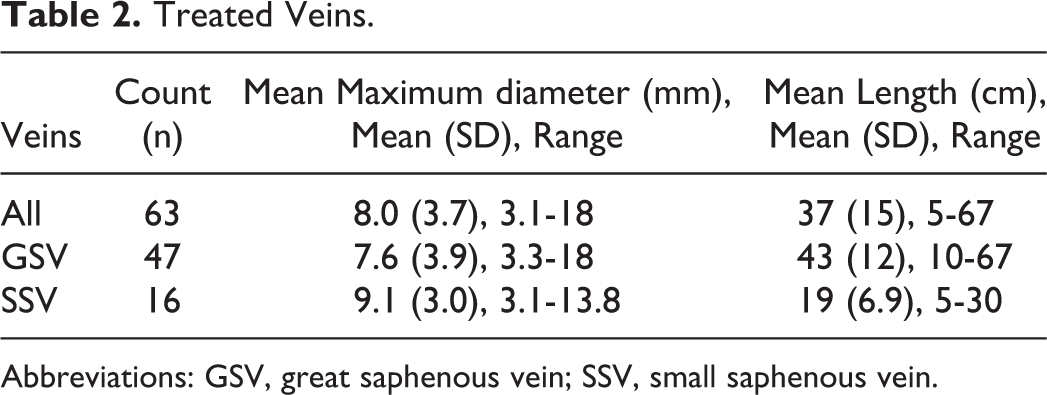
Abbreviations: GSV, great saphenous vein; SSV, small saphenous vein.
The baseline examinations included revised Venous Clinical Severity Scores (rVCSS), Aberdeen Varicose Vein Questionnaires, and numerical pain rating scale (NRS). 16 –19
Procedure
With ultrasound guidance, a 5F delivery catheter in 7F introducer sheath was advanced to the saphenofemoral junction (SFJ) or saphenopopliteal junction (SPJ) and was positioned 5.0 cm distal to the SFJ or SPJ. Saphenous vein was compressed by the ultrasound probe with left hand thoroughly, at 2 cm proximal to the delivery catheter tip. Two injections of approximately 0.10 mL cyanoacrylate glue each were given 1 cm apart at this location, followed by a 3-minute period of local compression with right hand, and then repeated single injection and 30-second compression for every 3 cm apart distally. Additional glue injection was allowed by the author’s discretion for areas with large diameter, areas with communicating vein, or areas with a perforating vein. The sequences were repeated until the entire length of the target vein was treated. The treatment was done throughout even around ankle level if the reflux existed. Finally, the sheath/catheter was removed and compression applied to the entry site until hemostasis was achieved. A small bandage was applied, and occlusion was confirmed by ultrasound.
Concomitant procedures (miniphlebectomy, sclerotherapy) were done after the above sequences were finished. The procedure started under local anesthesia and music of patient’s preference was turned on to provide a calming atmosphere. If patients requested for sedation or complained of pain, anxiety, or fear during the procedure, intravenous (IV) sedation was done in the presence of an anesthetist.
Compression stockings were required for the patients who underwent concomitant procedures: 3 days for those who underwent concomitant phlebectomy and 7 days for those who underwent concomitant sclerotherapy. Patients were instructed to ambulate frequently after procedure and to return to work or normal activities at their own discretion. Routine oral nonsteroidal anti-inflammatory agents (NSAIDs) were given to all patients for 5 days.
Postprocedural Evaluations
Patients stayed several hours more after procedure to recover from IV sedation or to confirm hemostasis. Before discharge, all patients’ legs were checked with duplex ultrasound and asked for NRS pain score also. All patients revisited the clinic for evaluation on postprocedural 10 days, 1 month, and 3 months. At each visit, all patients’ legs were checked with duplex ultrasound and asked for any AEs and NRS. For patients who couldn’t visit our clinic at exact scheduled days, phone calls were made to obtain NRS.
Revised Venous Clinical Severity Scores was collected at 1 month for postprocedural evaluation. Aberdeen Varicose Vein Questionnaire was collected at 3 month for postprocedural evaluation. We defined “abnormal skin reaction,” one of the known AE after CAC, as any of abnormal sudden growing skin findings such as erythema, itching, pain, edema, and tenderness over the TV area. 11 –15
Results
Procedure Characteristics
Table 1 shows patients demographics and clinical staging. The majority of the patients were women (79.4%). The most frequent presenting CEAP class was C2 (58.8%). Thirteen (38.2%) patients had 1 TV and 15 (44.1%) had 2 TVs.
A total of 34 patients with 63 saphenous veins were selected (Table 2). Mean size (mm) of all veins was 8.0 ± 3.7, and 12 (14%) saphenous veins had maximum diameters of more than 12 mm.
Operative and Postoperative Outcomes
A total of 63 TVs were successfully treated in the 34 patients. There were no technical failure or device-related complications during the procedure. Procedural characteristics are summarized in Table 3. Procedure duration calculated from venous access to placing the bandage and includes time for converting to IV sedation during the procedure and does not include time for concomitant procedures.
Procedure Characteristics.
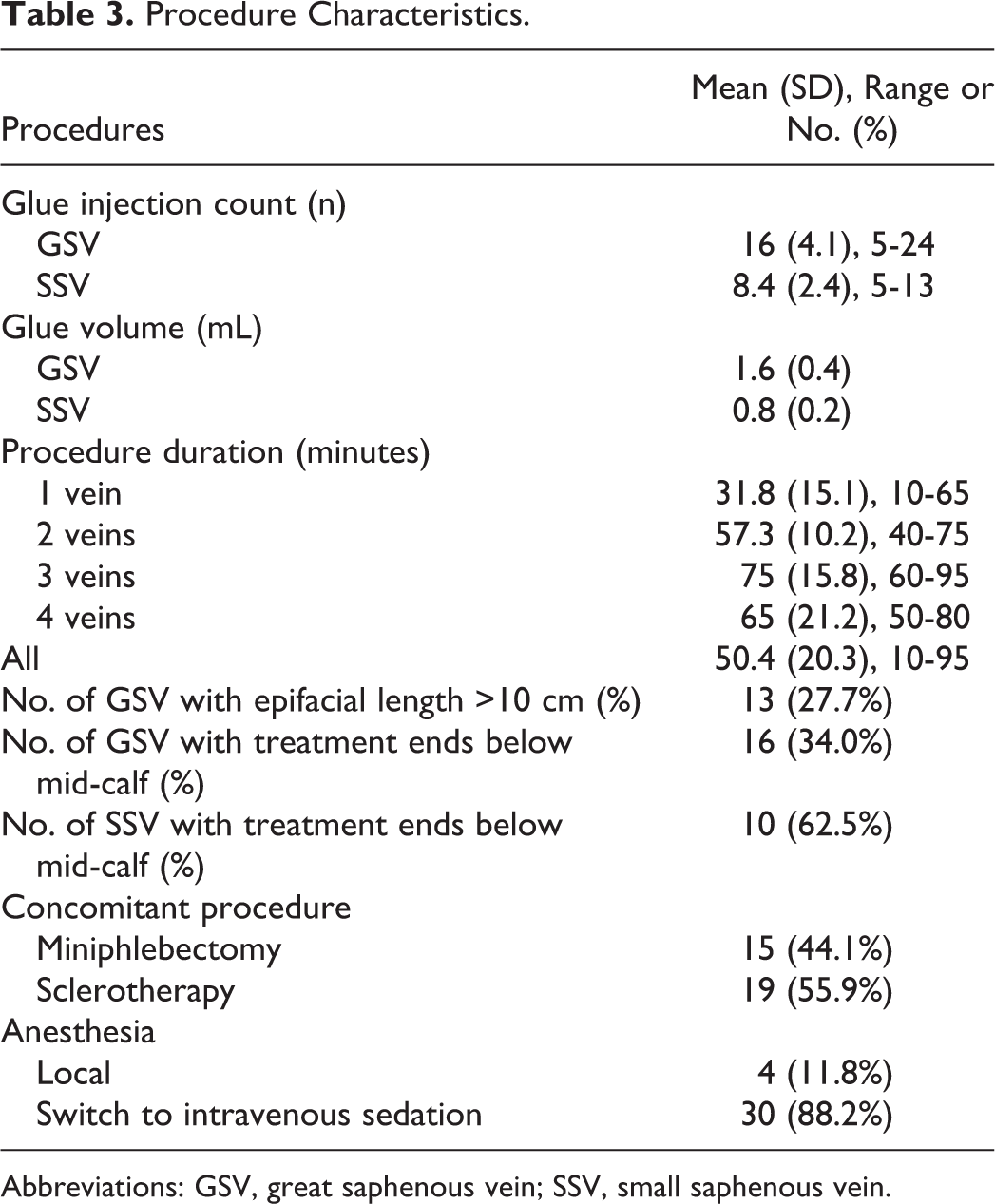
Abbreviations: GSV, great saphenous vein; SSV, small saphenous vein.
All of the 47 treated GSVs were accessed below the knee. Of those, 16 GSV treatments were ended at below mid-calf area, actually just above the ankle area. Ten SSV treatments were ended at below mid-calf area. Thirteen GSVs had epifacial segment of more than 10 cm length (Table 3).
According to the author’s discretion, concomitant miniphlebectomy were done in 15 (44.1%) patients and concomitant sclerotherapy were done in 19 (55.9%) patients . Concomitant miniphlebectomy were done under local anesthesia or IV sedation. Telangiectasia or reticular veins were treated with concomitant sclerotherapy with 0.1% to 0.5% sodium tetradecyl sulfate.
Only 4 (11.8%) patients underwent procedures under whole local anesthesia and other 30 patients (88.2%) underwent procedures under IV sedation. All of TVs showed complete closure (CC) at 6 hours after the procedure, at 10 days, and at 1 month. The mean average follow-up period (days) with 34 patients was 29.6 ± 19.7 (9-95). Twenty-five patients with 42 veins had a follow-up period more than 1 month (Table 4). And only 2 patients with 3 veins had follow-up period of more than 3 months. The definition of complete closure is less than 5 cm length of patency.
One-Month Follow-Up Results: Occlusion.
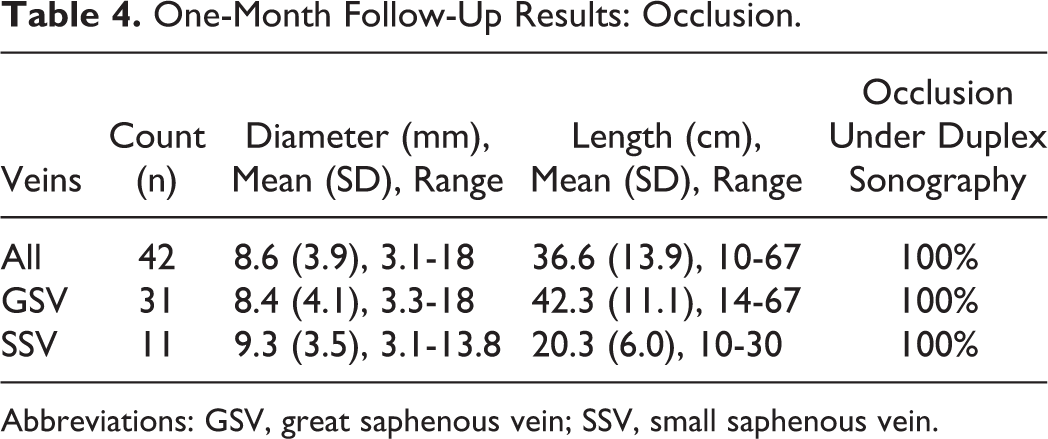
Abbreviations: GSV, great saphenous vein; SSV, small saphenous vein.
Mean NRS pain score at 6 hours, 1 day, 10 days, and 1 month after the procedure was 2.7 ± 1.9 (0-8), 1.7 ± 1.3 (0-5), 1.6 ± 2.1 (0-7), and 0.8 ± 1.1 (0-3), respectively.revised Venous Clinical Severity Scores at 1 month after the procedure decreased to 1.2 ± 1.0 (0-5; P = .024).
There were no life-threatening AEs. Table 5 shows the AE that occurred. There were no deep vein thromboses or thrombus extension detected.
One-Month Follow-Up Results: Adverse Events.
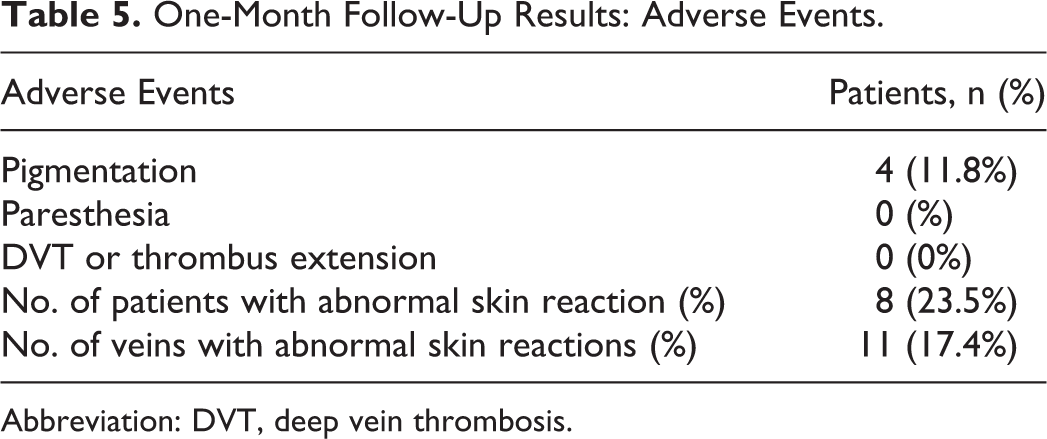
Abbreviation: DVT, deep vein thrombosis.
The most common AE was “abnormal skin reaction,” defined as any abnormal sudden growing skin findings such as erythema, itching, pain, edema, and tenderness over the TV area which occurred in 8 patients with 11 (17.4%) of 63 saphenous veins. It happened at 3, 11, 12, 13, 13, 13, 13, and 17 days after procedure. When this “abnormal skin reaction” occurred, most patients complained abrupt high NRS scores ranging from 5 to 8. When the “abnormal skin reaction” occurred, we prescribed NSAIDs for 5 to 7 days. All phenomenons were recovered fully in 2 weeks. Four patients showed pigmentation over the treated area, which all occurred at the epifacial GSV area (Table 5).
As mentioned above, 13 GSVs had an epifacial portion of more than 10 cm. And 16 GSVs and 10 SSVs were accessed and treated below mid-calf, actually just above ankle level. No paresthesia was detected.
Discussion
This study demonstrates that CAC with VenaSeal system is safe and effective for the treatment of CVD. This is the first Korean study to describe the VenaSeal system and the first report to treat SSV with VenaSeal system in Asian countries.
In previous studies, VenaSeal system reported that CC rate was similar to previous thermal ablation techniques. 11 –15 In our study, initial outcome of CC was 100% with satisfactory postprocedural events.
According to previous reports, the most common AE with VenaSeal system was phlebitis and it ranged from 11.4% to 20%. 12 –15 A precise definition of phlebitis after VenaSeal system is not established yet.
In our study, we used the term “abnormal skin reaction” instead of phlebitis, and it occurred in 8 of 34 (23.5%) patients with 11 of 63 (17.4%) saphenous veins . We defined this as any of unusual sudden growing skin findings such as erythema, itching, pain, edema, and tenderness over the TV area. So it may include not only phlebitis but also other mild events.
We presumed that the “abnormal skin reaction,” mentioned as phlebitis in previous studies, is a little different from the typical phlebitis. 11 –15 Possibly, this phenomenon is more likely to be a “foreign body reaction” or “allergic reaction” to cyanoacrylate rather than phlebitis. However, more studies need to be carried out to investigate this matter.
Interestingly, all “abnormal skin reaction” occurred at GSV area and only in female patients. We could not identify the definite factors associated with this “abnormal skin reaction” yet. We assume this may be a delayed hypersensitivity reaction to “acrylate” in VenaSeal, may be related to patient’s body surface area (BSA) or body mass index, may be due to total glue dose, or may be related to the location of the glue injected. However, we are trying to investigate to identify positive factors and expect to report soon.
As mentioned above, we prescribed routine postprocedural oral NSAIDs for 5 days. And we hoped that this routine oral NSAIDs may help to lower the risk of “abnormal skin reaction.” However, the occurrence rate in our study was quite similar to the previous studies. A precise definition of this phlebitis-like phenomenon should be established.
The most valuable aspect of VenaSeal system is avoidance of thermal injury to adjacent normal tissue. As shown in previous reports, there was no paresthesia after VenaSeal system. 12,13
In our study, all 47 GSVs were accessed at below knee area and the treatment of 16 GSVs and 10 SSVs ended below mid-calf area just above the ankle level. And 13 GSVs had epifacial portion more than 10 cm (Table 3). No patients developed paresthesia. Gibson and Ferris previously reported the outcomes with 8 SSVs. 15 Our study includes 16 SSVs, and we identified the safety and efficacy of the VenaSeal system below the mid-calf area near the ankle, which is to our knowledge the first to be reported.
In contrast to previous studies from Western countries, most of our procedures were carried out under IV sedation. In our experiences, when compared to Western patients, most Asian patients are concerned about the pain and feel anxious during the procedure. As mentioned above, we did concomitant miniphlebectomy for 44.1% of patients. And when patients complained of pain or discomfort during miniphlebectomy, IV sedation was carried out for a moment.
There are many reports about the racial differences with pain threshold. It was commonly reported that Asian populations had a lower pain threshold than Western populations. 18 –20 So as a practical matter, many of endovenous procedures have undergone more intense anesthetic method compared to local anesthesia in Asian countries.
There is no obvious report about the advantage of CAC for the regression of varicosities after procedure. However, in my opinion, the liquid glue flows into the adjacent varicosities during the procedure with compression, for adjacent varicosities seem to have self-regressed more efficiently than expected.
There were 2 patients who underwent 4 saphenous vein treatments. Both patients were with short stature and the sum of 4 veins length was smaller than 100 cm. All of the procedures were performed with 1 bottle of glue efficiently.
Conclusion
Cyanoacrylate closure is a safe and efficacious procedure for the treatment of CVD caused by refluxing saphenous veins. And also it showed good result with the veins located below the knee and near the ankle level and also in epifacial veins without paresthesia. Treatment of multiple veins in a single session with concomitant procedures was well tolerated by patients. Phlebitis-like “abnormal skin lesion” was mild and transient; however, more investigation should be carried out to overcome this phenomenon.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.