
Abstract
Objectives:
Nearly 25% of vascular surgery patients operated on for peripheral vascular disease are readmitted within 30 days. Development of adjuncts to minimize wound complications remains an area of great interest. Here, we present our experience with intraoperative fluorescent angiography (IFA) as a tool to predict skin flap viability following lower extremity amputations (LEAs).
Methods:
Experience with IFA using indocyanine green (ICG) dye was reviewed retrospectively at a single institution. Records of patients undergoing LEA with use of IFA by 2 vascular surgeons from 2013 to 2014 were reviewed. Absolute and relative tissue perfusion values were evaluated for sensitivity and specificity in regard to skin flap viability.
Results:
Thirteen patients with a mean age of 70.5 years (standard deviation [SD] = 12.0, range: 49-93 years) underwent 17 amputations. Indications included rest pain, tissue gangrene, and vascular disease unsuitable for revascularization. Amputation levels included toe (23%), transmetatarsal (18%), below knee (41%), and above knee (18%). Six (35%) amputations required revision with a mean time-to-revision of 26.1 days (SD = 19.9, range: 9-61 days). Of these revisions, 14 (83%) patients proceeded to a proximal-level amputation. Mean follow-up was 235 days (SD = 148, range: 5-448 days), and IFA was used in all cases. Absolute perfusion values (APVs) between 5 and 9 displayed sensitivity and specificity of 50% and 64%, respectively. Additionally, a relative perfusion value (RPV) of ≤31% displayed 100% sensitivity and specificity. Sensitivity and specificity fell to 83% at a relative perfusion of ≤27% and ≤35%, respectively.
Conclusion:
IFA during LEA is safe and easily performed by the vascular surgeon. The RPVs as a predictor of skin flap viability correlate well with those reported in breast reconstructive surgery. Unfortunately, APVs fail to support any predication for flap failure or success. Patient comorbidities and intraoperative variables such as vasopressor use may contribute to this finding.
Introduction
Wound complications following surgery continue to be a significant cause for patient morbidity and a financial burden on the health-care system. Nearly 25% of patients are readmitted within 30 days following surgery for peripheral vascular disease. 1 Despite the fact that vascular surgery patients undergoing lower extremity amputations (LEAs) utilize extensive health-care resources continuing far beyond the perioperative period, readmissions for amputees have been infrequently studied. 2 Recently, multiple investigators have demonstrated that wound complications account for 49% to 52% of unplanned readmissions related to the index LEA in the form of infections, wound healing issues, and hematomas. 2,3 As infection and wound healing problems are linked to lower levels of tissue perfusion, methods to ensure adequate postprocedure perfusion may decrease readmissions related to the index amputation.
Current methods for the assessment of skin flap perfusion, and thus viability, rely almost exclusively on clinical judgment. Subjective assessments of intraoperative skin temperature, color, dermal edge bleeding, and capillary refill time all contribute to this determination. Several adjuncts such as percutaneous oxygen saturation, laser Doppler velocimetry, and fluorescein dye angiography have been utilized to assist in evaluating flap perfusion. However, these techniques can be time-consuming to implement, have potential side effects, or do not allow for repeat measurements. Intraoperative fluorescent angiography (IFA) using indocyanine green dye (ICG) is a novel technology that is increasingly employed in plastic surgery and breast reconstruction due to its ability to overcome the limitations of previous modalities.
Reports in plastic and general surgery have shown anecdotal benefit from IFA use as an adjunct to clinical intraoperative assessments of skin viability. 4,5 Larger studies cite decreased postoperative complication rates for postmastectomy breast reconstruction in the pre- and post-IFA eras. 6,7 Phillips et al compared IFA with fluorescein for their ability to predict skin necrosis following mastectomy with reconstruction. They found that while both modalities exhibit high sensitivity for predicting skin necrosis, IFA was more specific, associated with shorter operative times, and allowed for multiple analyses. 8 However, the literature is sparse in objective data for statistical analysis and offers little insight as to how IFA should be used to guide patient care.
Methods
A retrospective review was performed of IFA use during LEA. Following institutional review board (IRB) approval, medical records were identified for review by querying the hospital system database for LEA procedures with ICG administration. Two vascular surgeons performed 17 LEAs on 13 patients over a 14-month period (June 2013 to August 2014). All operations were performed at a single institution.
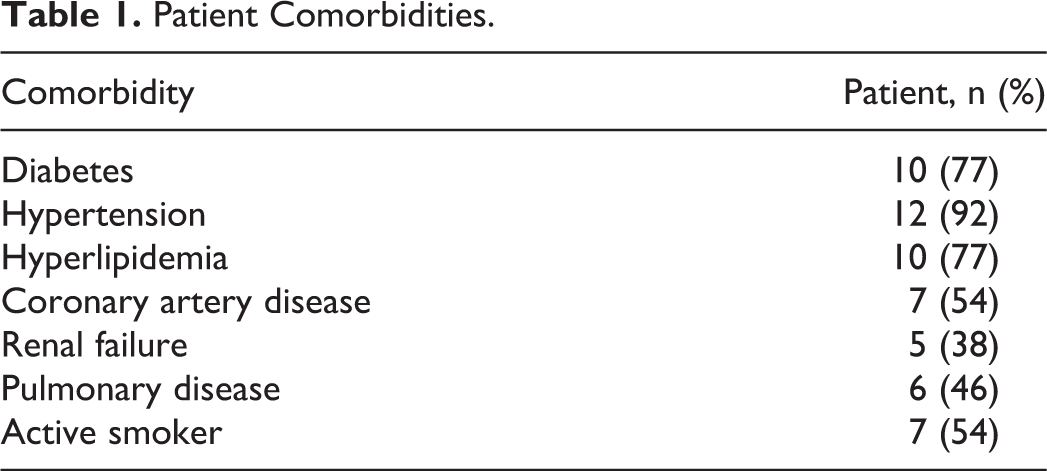
Demographics obtained included age, sex, and race. Comorbidities studied included smoking status, diabetes, hypertension, hyperlipidemia, coronary artery disease, renal failure, and pulmonary disease. Comorbidities were defined as the presence of “active” diagnoses in the medical chart within 6 months from the date of surgery. Postoperative follow-up and wound evaluation included chart review of both inpatient and outpatient encounters. Intraoperative details studied included mean systolic, diastolic, and arterial pressures, vasopressor use, mean temperature, and mean oxygen saturation.
Each patient underwent IFA using the SPY Elite system (NOVADAQ, Bonita Springs, Florida) after a 10-mg dose of ICG dye. The ICG was administered intravenously immediately following the completion of layered closure with either staples or interrupted monofilament suture at the skin level. Video recordings were taken for the 120 seconds immediately following dye administration to document tissue perfusion. Absolute perfusion values (APVs) and relative perfusion values (RPVs) were obtained using SPY-Q quantitative software based on a snapshot image taken at the 90-second time interval. The APVs are based off a fixed gray scale (0-255) consistent from patient to patient. The RPVs differ as SPY software assigns a “100% flow” reference point to which all other points for that image are compared. This point is not equivalent from case to case but rather serves as a patient-specific control. The SPY device was operated in a fixed baseline mode (−2) under manufacturer default settings. No drains were utilized, and all patients received, at minimum, 24 hours of perioperative antibiotics. Patients were followed through their hospital admission and seen in office 2 weeks following surgery. Additional postoperative follow-up visits were determined by the surgeon on an as-needed basis.
Based on chart review and documentation, areas known to have become necrotic postoperatively and those areas known to be viable were further characterized by the creation of “contour islands.” These contour islands were created by annotating the perfusion snapshot in comparison against the patient’s wound. Ten APV data points were taken within known necrotic areas and were averaged to provide an adjusted APV for necrosis. The APV data points for contour islands of viable cases were adjusted in a similar fashion; however, data points were averaged across the entire field of viable tissue.
The RPV analysis was performed in similar fashion. However, as RPV varies from case to case, comparisons of viable to necrotic skin were performed within each case rather than across the study population. Again, 10 data points within known necrotic areas (Figure 1) and within known surrounding viable contours were averaged (Figure 2). Using the data collected for adjusted RPVs and adjusted APVs, we were able to calculate sensitivity and specificity of each value (Figures 3 and 4).
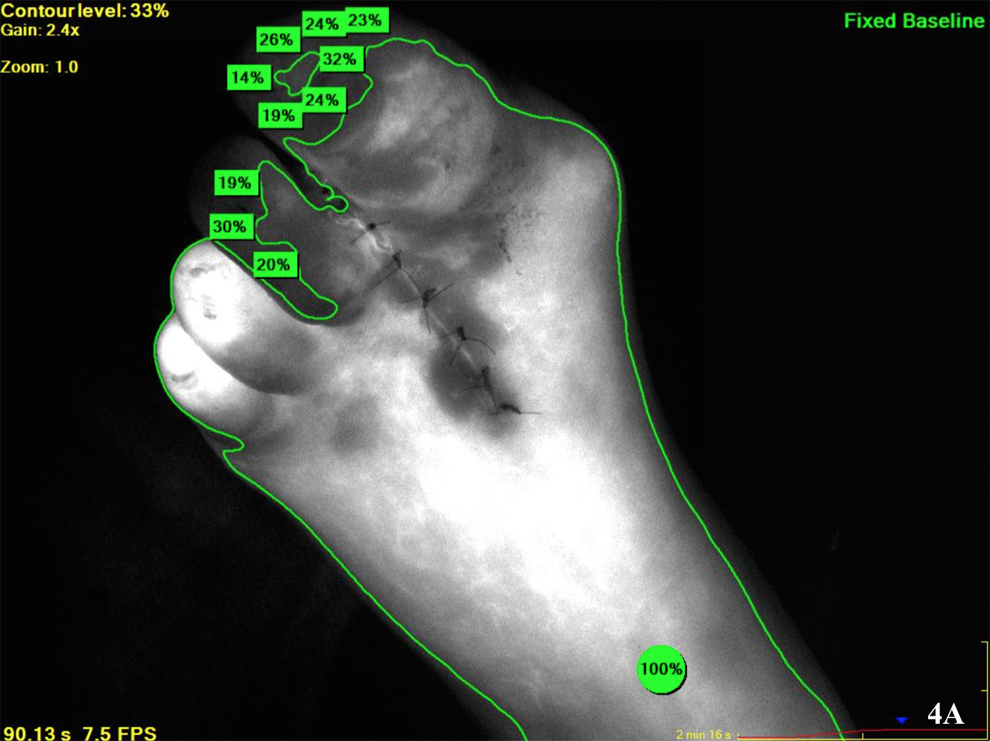
Relative perfusion value data points within known necrotic area.

Relative perfusion value data points within known viable area.
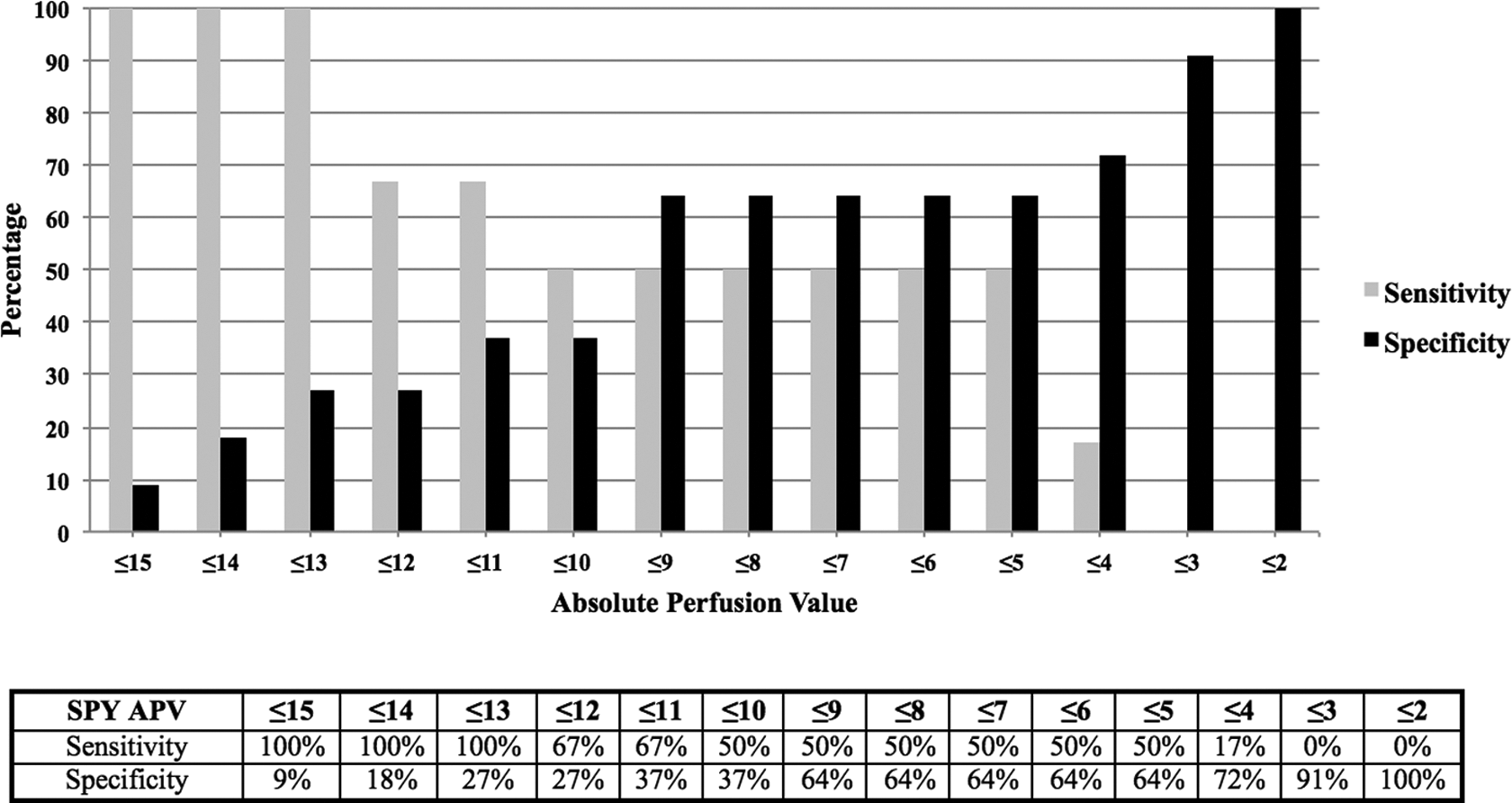
Sensitivities and specificities for adjusted absolute perfusion values.
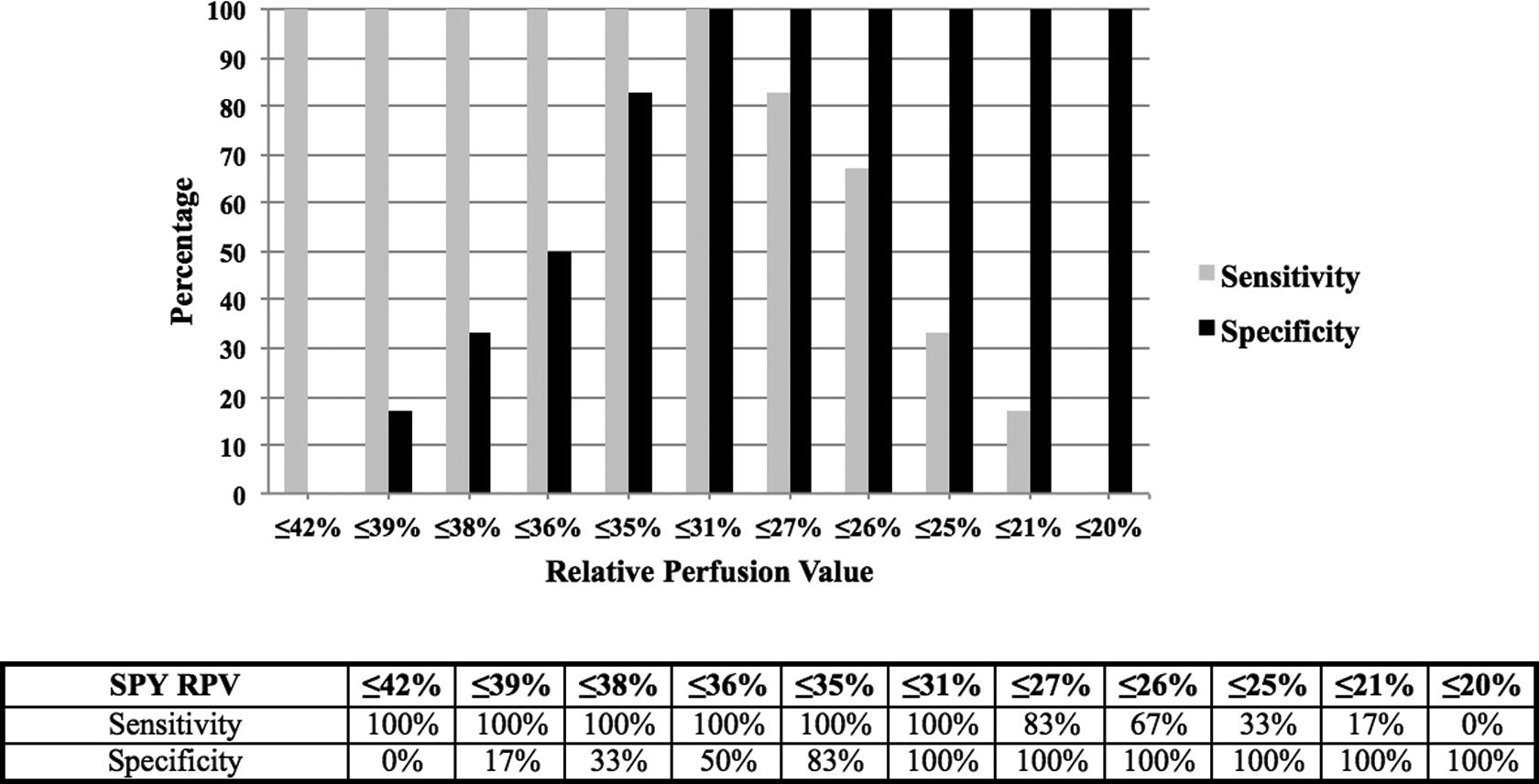
Sensitivities and specificities for adjusted relative perfusion values.
Demographics and comorbidities were descriptively characterized with arithmetic means and percentages, while standard deviation (SD) was calculated for continuous measures. Frequency and percentages were reported for categorical measures. Finally, calculations and analyses were performed using Microsoft Excel and Minitab 15 software.
Results
From June 2013 to August 2014, 13 patients underwent a total of 17 LEAs, where IFA using ICG was performed to study skin flap viability. The mean follow-up period was 235 days (SD = 148, range: 5-448 days). One patient died 5 days after his surgery due to causes unrelated to his surgery. The study population consisted of 11 men and 2 women with a mean age of 70.5 years (SD = 12.0, range: 49-93 years). Nine Caucasians and 4 African Americans accounted for race. Study population comorbidities are provided in Table 1 and vascular history in Table 2.
Patient Comorbidities.
Vascular History.
Study candidates were recruited from both the inpatient and the outpatient settings. Each patient underwent a detailed history and physical evaluation. Angiography was performed on each patient to establish their anatomy and extent of their vascular disease; 12 patients underwent aortograms with bilateral lower extremity run-off and 1 patient underwent a computed tomography (CT) angiogram of the aorta and bilateral lower extremities. Indications for index amputation included rest pain and tissue gangrene secondary to peripheral arterial disease deemed “unable to bypass” or with “nonrestorable flow” by the surgeon. No amputations were related to trauma. Each patient underwent counseling regarding prognosis and recovery associated with each anatomical amputation option.
Intraoperative parameters recorded are displayed in Table 3. Of note, 29% of patients received intraoperative vasopressors. Amputation levels were as follows: toe (23%), transmetatarsal (18%), below knee (41%), and above knee (18%).
Intraoperative Parameters.
Six LEAs (35%) required revision due to skin flap necrosis with a mean time to revision of 26.1 days (SD = 19.9, range: 9-61 days). The index amputation for these cases was 2 transmetatarsal amputations, 3 below-knee amputations, and 1 above-knee amputation. Of these revisions, 83% proceeded to a proximal-level amputation. In addition to the 6 revisions, 1 patient required reoperation for evacuation of a wound hematoma. This patient’s skin flap was deemed viable at the time of reoperation and, thus, was not considered a revision.
Adjusted APV for areas of necrosis was found to range from 4 to 14, while adjusted RPV for the same areas ranged from 21% to 31%. Adjusted APV for areas of viable tissue ranged from 3 to 16 and adjusted RPV ranged from 35% to 42%.
Based on current data in breast reconstructive literature, an APV of ≤7 was initially assessed for sensitivity and specificity in regard to skin flap viability. Our data demonstrated sensitivity and specificity of 50% and 64%, respectively, with an APV of 7. This correlated with a positive predictive value (PPV) and negative predictive value (NPV) of 43% and 70%. When using absolute perfusion scores between 5 and 9, our results for sensitivity and specificity remained consistent at 50% and 64%, respectively (Figure 3).
Upon analysis of our RPV data, we found that an RPV of ≤31% had 100% sensitivity and specificity for tissue necrosis. Sensitivity fell to 83% at RPV of ≤27%, while specificity was 83% at an RPV of ≤35% (Figure 4).
Discussion
Skin flap necrosis with resultant infection following LEA continues to be a problem leading to hospital readmissions. The morbidity, mortality, and cost of complications are felt by patients, physicians, and the health-care system as a whole.
Clinical estimators of skin viability such as dermal edge bleeding, capillary refill, and skin temperature are imperfect at best. In an effort to decrease wound complications and readmissions following LEA, we chose to retrospectively analyze IFA use to assess its potential to predict skin flap viability. Evidence from breast reconstructive and plastic surgery studies has found utility in its use to decrease wound complications. However, IFA as a modality to predict skin flap viability is unstudied in the vascular literature. Unfortunately, patient demographics and comorbidities in these previously studied patient populations are vastly different from those encountered in vascular surgery. High rates of diabetes, hypertension, and advanced age account for microcirculatory changes frequently found in our study population.
Current literature is divided on the superiority of absolute perfusion in predicting flap viability. Some sources advocate utilizing APVs due to the fact that relative perfusion units vary from individual to individual and cannot be extrapolated across patients. Recent prospective trials evaluating postmastectomy skin flap necrosis address the quantification of objective data from IFA use. Munabi et al achieved a sensitivity and specificity for necrosis of 88% and 83%, respectively, with an APV of
In our study, we found relative perfusion to be the better predictor of skin flap viability. Based on our results, we found that sensitivity and specificity remained constant for a wide range of APVs with a low sensitivity of 50% for flap viability. In contrast, RPVs had maximal sensitivity and specificity converge at a RPV of 31%. These values were consistent with the findings of Moyer and Losken as described earlier, 10 suggesting that larger prospective studies in vascular patients should focus on RPVs rather than absolute fluorescence. Vascular patients have significantly different comorbidities from patients undergoing mastectomies and reconstructive surgery. As a result, they may have changes in their microcirculatory anatomy that favors relative perfusion as an assessment of flap viability. Additionally, they are already known to have compromised tissue perfusion. Thus, the APVs would be expected to be lower at the surgical site, and it is unclear if same degree of perfusion is required between patients. Lastly, the nature of the flaps created for mastectomies and amputations differ significantly. Mastectomy flaps are essentially random flaps that rely on the subdermal vasculature for perfusion. In contrast, amputations often leave the interface between well-vascularized muscle and subcutaneous tissue relatively untouched.
Use of IFA currently functions as an adjunct to surgeon clinical judgment. Our goal with this study is to evaluate the feasibility of utilizing IFA in the realm of vascular surgery. It is not the intention of this study to suggest patients should undergo a more proximal amputation if RPVs suggest the likelihood of a nonhealing stump. With image capture times of roughly 2 minutes, we feel that IFA use can be accomplished quickly as well as safely without an undue increase in operative times. We only performed IFA once to obtain perfusion data for postoperative comparison. Our operative revision rate was 35%, which was in part due to our patients electing for less aggressive surgical management in hopes of maintaining greater mobility. However, our findings suggest that RPVs, at a minimum, may aid the surgeon intraoperatively in deciding if revision of the flaps is necessary or if staged wound closure may decrease wound complications postoperatively. This is especially true in cases where a patient wishes to pursue a more distal amputation that the surgeon feels would be at higher risk of nonhealing.
Obvious limitations to this pilot study include the small sample size and retrospective nature of the review. Furthermore, variable postoperative follow-up and incomplete chart documentation limit the ability to precisely study necrotic and viable areas, which could alter APVs and RPVs obtained. We feel that this could be improved with intraoperative stenciling of contour islands and comparison of these templates to wound photographs taken during structured follow-up in the outpatient setting. Further study is needed to establish specific RPVs or APVs which can predict necrosis intraoperatively.
Conclusion
While the use of IFA has been reported frequently in the breast reconstructive and plastic surgery literature, experience of IFA in vascular patients has been undocumented. Despite the significant presence of patient comorbidities such as diabetes, nicotine use, and hypertension that alter the microvasculature of the dermis, our study demonstrates that the utility of IFA seen in a healthier patient population remains applicable to our patient subset. However, it appears that RPVs are more indicative and predictive of skin viability or necrosis than APVs. We strongly believe that our data support the use of IFA in the vascular surgery patient as a safe and feasible adjunct to the clinical assessment of skin perfusion. Our findings also suggest that an RPV ≥31% is a predictor of flap viability. We feel that the use of IFA with RPVs warrants further large-scale investigation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.