
Abstract
Purpose:
To describe the application of uncovered chimney stent grafts with the Nellix endovascular aneurysm sealing technique (ChEVAS) for juxtarenal abdominal aortic aneurysms (JAAAs).
Case Report:
Two patients with JAAA and multiple comorbidities were considered unfit for open surgery and were selected for an endovascular approach. Fenestrated and branched endografts were too expensive, and a chimney endovascular approach was considered inappropriate for the relatively high incidence of proximal type I endoleak and graft migration. ChEVAS was performed successfully with the novel addition of uncovered chimney stents to further reduce costs and possibly improve target vessel patency. JAAA exclusion and visceral vessel patency was confirmed at 18-month follow-up.
Conclusion:
ChEVAS with bare chimney stents is technically less complex, potentially reduces access complications and procedural costs, and may improve long-term patency compared to alternative techniques. Results at 18 months seem promising, but strict follow-up is necessary as the long-term durability is unknown.
Keywords
Introduction
Fenestrated and branched endografts were introduced as an endovascular solution for complex abdominal aortic aneurysms (AAAs) without adequate landing zones (juxtarenal, pararenal, and suprarenal aneurysms) for traditional infrarenal endovascular aneurysm repair (EVAR). Current literature confirms promising results, 1-2 but the techniques usually require custom manufacturing for each patient and are therefore relatively expensive with delayed availability. Chimney techniques (Ch) for EVAR include the delivery of smaller stent grafts running parallel to the main endograft to maintain visceral vessel perfusion. An alternative to fenestrated and branched endografts, ChEVAR is a more cost-effective, is less technically challenging, and is a readily available solution with reserved results. 3 –7 The main risk of ChEVAR, however, is proximal type I endoleak through the “gutters,” which can occur between the main endograft and the chimney stent graft. 6-7 Type I endoleak associated with ChEVAR is not rare and ranges from 7% to 12%. 2,5,8
The endovascular aneurysm sealing (EVAS) technique was developed in response to several limitations of EVAR, specifically endoleaks and secondary intervention. The system consists of 2 long, covered balloon-expandable stent grafts surrounded by 2 endobags, which are filled with polyethylene glycol (PEG). The aneurysm is thereby “filled,” and the endograft is theoretically more stable in the aneurysm sac with promising early to midterm results. 9
Recently, the advantages of the EVAS approach have been adapted with the chimney technique (ChEVAS) for complex AAA unsuitable for standard EVAR, thereby reducing costs and delays often associated with fenestrated and branched endografts. 10 –12 Previous ChEVAS experiences have been reported in the literature with the use of covered chimney stent grafts for visceral vessels. The current case series describes ChEVAS with, for the first time, uncovered chimney stent grafts in 2 patients with juxtarenal AAAs (JAAA), reducing operative complexity, introducer sheath thickness, costs, and possibly offering an advantage in target vessel long-term patency.
Case Report
Two patients presented at our institution with JAAAs documented at preoperative computed tomography angiography (angio-CT). The angio-CT of patient 2 also revealed stenosis of the left renal artery bifurcation. Patient characteristics and comorbidities are summarized in Table 1.
Patient Characteristics and Comorbidities.
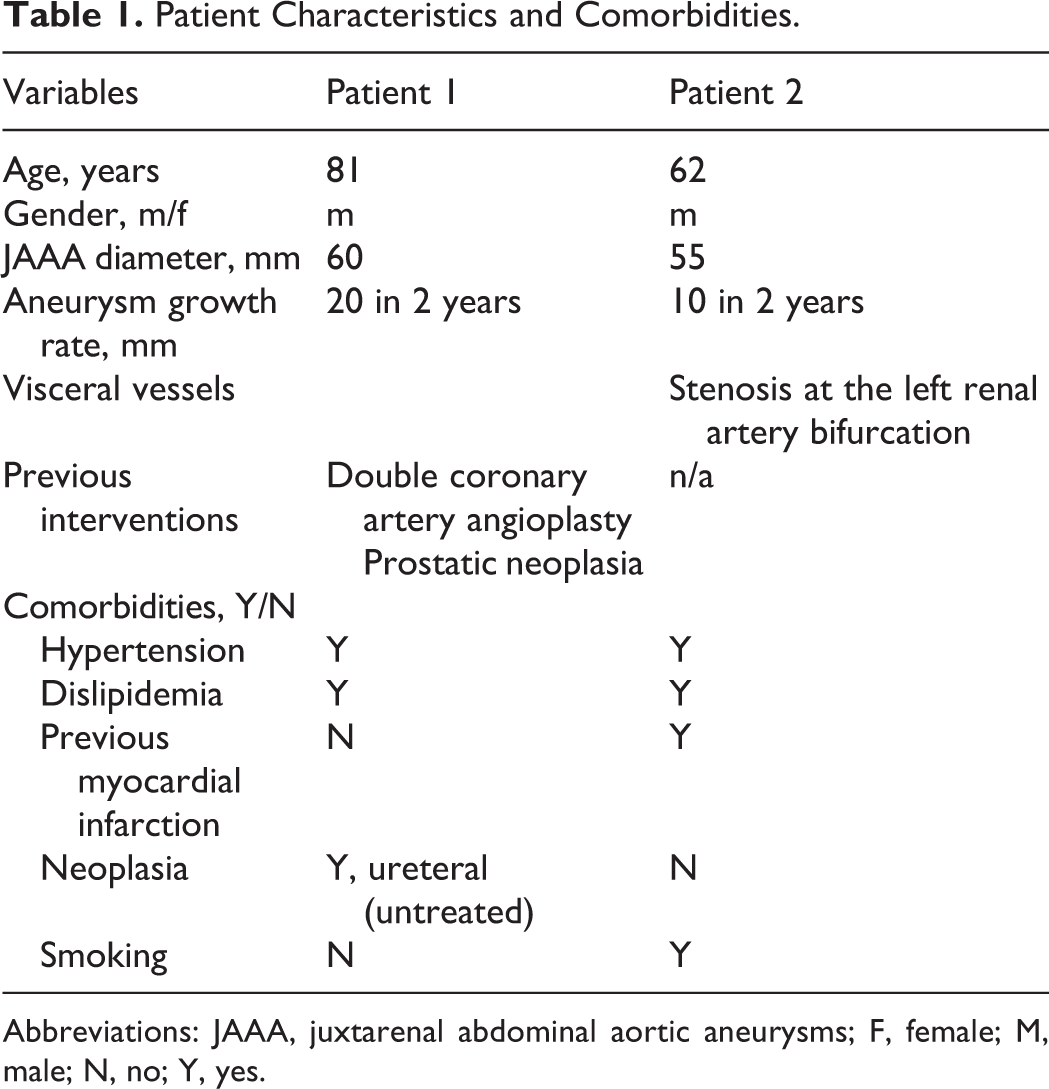
Abbreviations: JAAA, juxtarenal abdominal aortic aneurysms; F, female; M, male; N, no; Y, yes.
Patient 1 was assessed as high risk for open surgery for cardiac comorbidities and patient 2 was still working and sexually active; therefore, an endovascular approach was preferred for both patients. Both patients were anatomically unsuitable for standard EVAR (inadequate landing zone below the renal arteries, with an aortic diameter of 32 and 33 mm, respectively, with a lateral ulceration in patient 2) and given the high costs and time required for the availability of fenestrated and branched endografts (generally the interventionists’ first option), the Nellix EVAS system (Endologix, Irvine, California), along with balloon expandable bare stents for renal arteries, was selected for a chimney approach (ChEVAS) for both patients.
Technical points for the deployment of the Nellix system have been previously described. 5 Briefly, both interventions were performed under general anesthesia in an operating room equipped with an OEC 9900 Elite C-arm (GE OEC Medical Systems, Salt Lake City, Utah). Arterial access was achieved via a percutaneous approach to the common femoral artery, and the left axillary artery for patient 1 and the brachial artery for patient 2 under ultrasound guidance. The distal third of the axillary artery was carefully exposed with a skin incision in the axillary fossa. In order to ease the exposure of the axillary artery and to facilitate movement of the X-ray C-arm, patient 1’s left arm was hyperabducted at 120° with the patient’s hand over his head.
Two 7F sheaths (Flexor Ansel Cook Medical, Bloomington, Indiana) were employed for patient 1, inserted through 2 different puncture sites of the axillary artery, to ensure enough blood supply to the left arm during the intervention (Figure 1). The sheaths were navigated up to the origin of the renal arteries, which were then cannulated and a 6 × 24 mm bare stent (Genesis Blue, Cordis, Miami Lakes, Florida) was placed in each renal artery but not delivered. The proximal 1 cm portion of the bare stent was left in the abdominal aorta. For patient 2, a 6F sheath (Flexor Ansel Cook medical) was advanced percutaneously from the brachial artery to just above the left renal artery. The renal artery was cannulated, and a 7 × 24 mm bare stent (Genesis Blue, Cordis, Miami Lakes, Florida) was positioned over the renal stenosis but not delivered, leaving the proximal 1 cm of the bare stent inside the aorta.
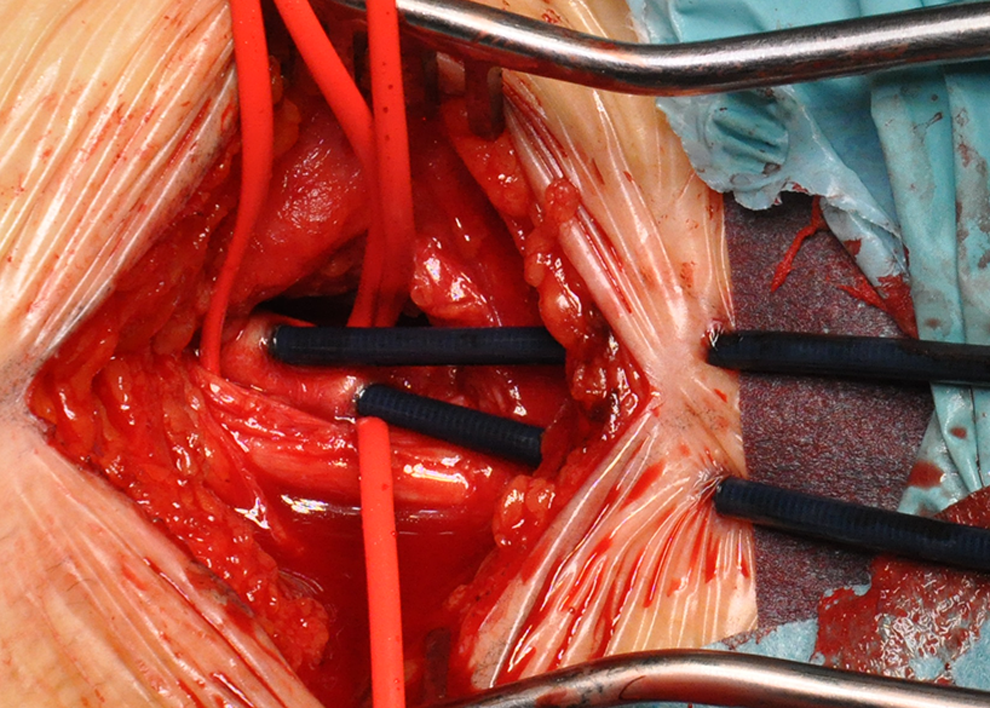
A 7F sheath was inserted through 2 different punctures of the axillary artery to ensure enough blood supply to the left arm during the intervention.
In both patients, the 170-cm length Nellix grafts were advanced from the common femoral arteries to just below the ostium of the mesenteric artery in patient 1 and the right renal artery in patient 2 (Figure 2). After intraoperative angiographic confirmation of the correct positioning of the Nellix and renal chimney bare stent grafts, all stents were simultaneously deployed with their respective balloon inflation devices, up to 8 atm.
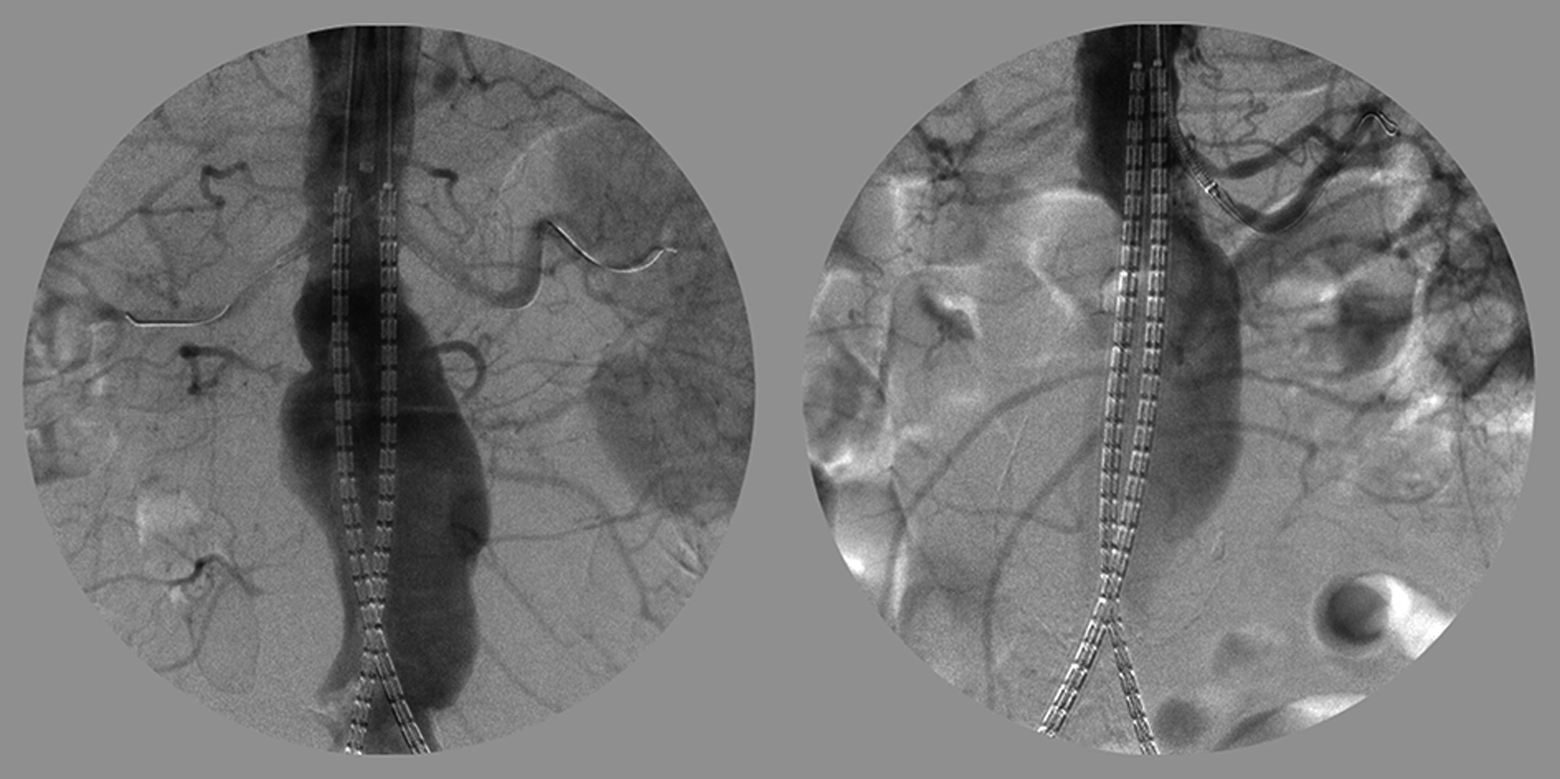
Intraoperative images show the correct positioning of the Nellix graft components and uncovered visceral stent grafts prior to inflation for patients 1 and 2, respectively.
With the balloons still inflated, the Nellix endobags were prefilled with a saline solution to the manufacturer’s recommended target inline pressure monitoring of 200 mm Hg (about 2 minutes up to the complete filling of the bag).
An intraoperative angiography confirmed the absence of types I and II endoleaks and the patency of all visceral vessels, after which the saline solution was replaced with 66 and 50 mL of PEG at a pressure of 200 mm Hg for patients 1 and 2, respectively.
All the balloons were deflated after the prefilling with saline and inflated again during the filling of the endobag up to the polymerization of the polyurethane (less than 5 minutes totally).
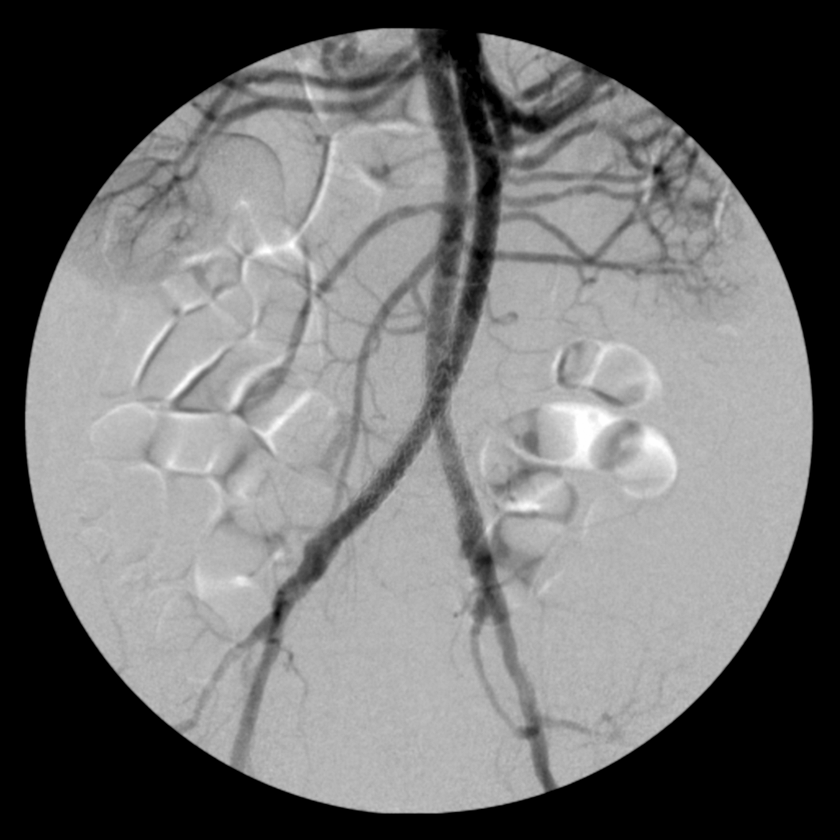
A final intraoperative angiography was performed to demonstrate the complete exclusion of the aneurysm, the absence of any endoleaks and patency of the Nellix endograft and visceral vessels (Figure 3), and in the case of Patient 2, the correction of the left renal stenosis with patency of both the main renal artery branches (Figure 4). Postdilatation of the bare stents was not required.
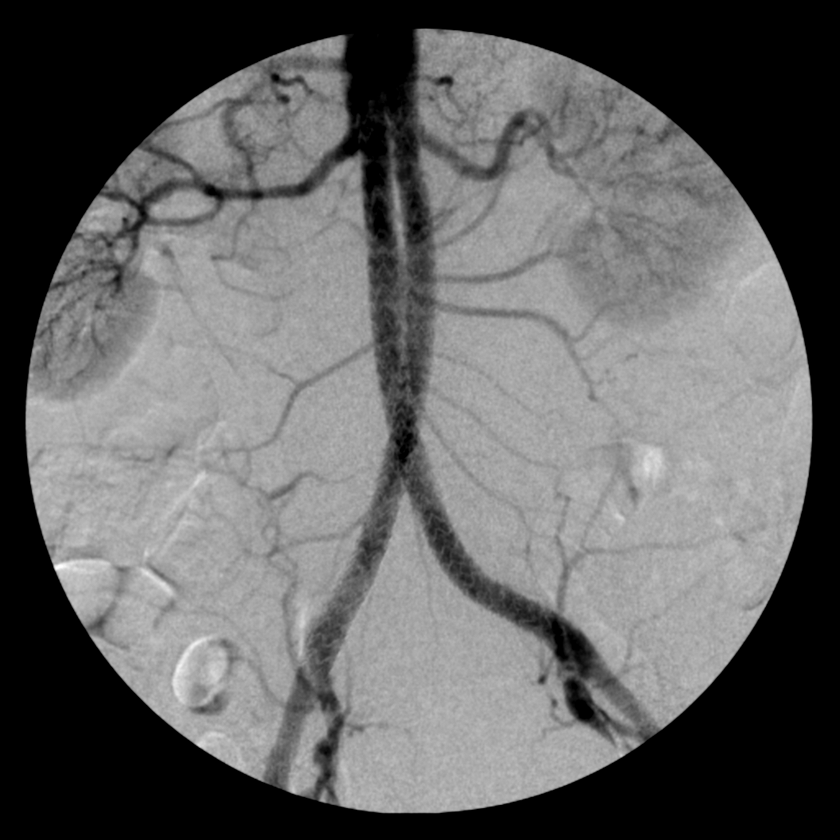
The final intraoperative angiography confirms complete exclusion of the JAAA and the absence of any endoleaks and patency of the Nellix endograft and visceral vessels. JAAA indicates juxtarenal abdominal aortic aneurysms.
The final intraoperative angiography shows complete exclusion of the JAAA and the absence of any endoleaks and patency of the Nellix endograft and visceral vessels and the correction of the renal stenosis with patency of both the main renal artery branches. JAAA indicates juxtarenal abdominal aortic aneurysms.
Total fluoroscopy time was 27.6 minutes and 26.4 minutes, respectively, and 120 mL of iodine contrast medium was used for both patients.
The postoperative course was uneventful in both cases and blood tests prior to discharge evidenced normal renal function, with a creatinine clearance of 60 mL/min and >60 mL/min for patients 1 and 2, respectively.
The patients were discharged with dual antiplatelet therapy for 6 months, after which single-use aspirin was suggested.
A postoperative angio-CT was performed prior to discharge on postoperative day 3 to confirm aneurysm exclusion, the absence of any endoleak or stent kinking, and visceral vessel patency in patient 1 (Figure 5) and additionally, the absence of residual renal artery stenosis in patient 2 (Figure 6).
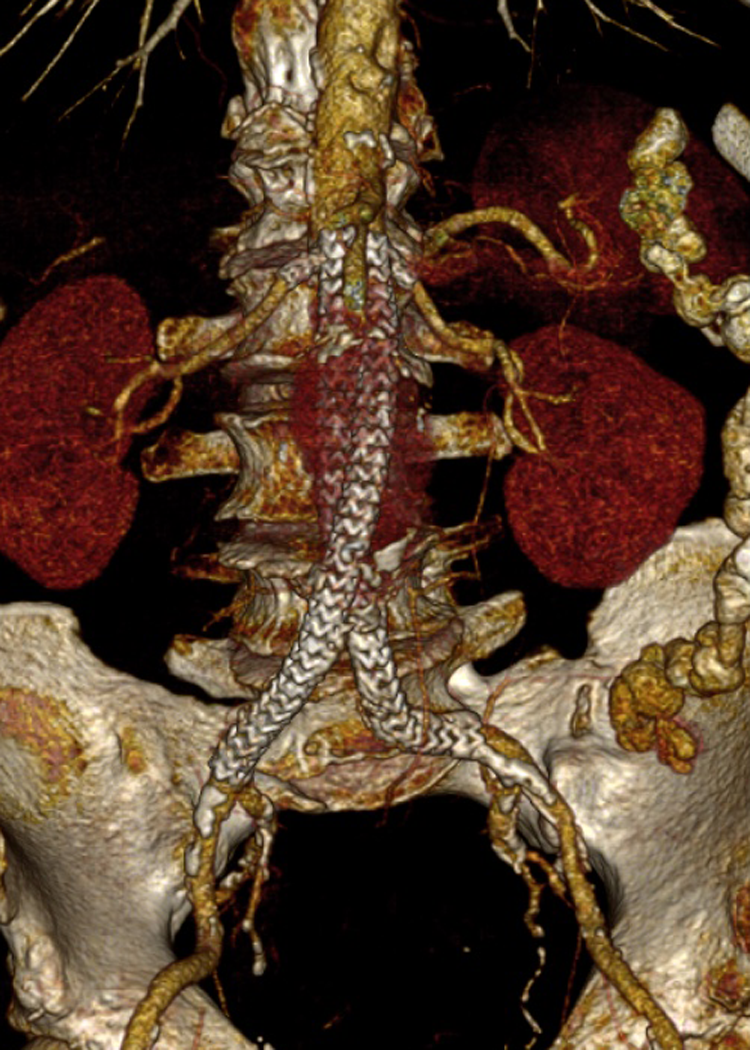
The postoperative angio-CT confirms aneurysm exclusion, the absence of any endoleak or stent kinking, and visceral vessel patency. CT, computed tomography.
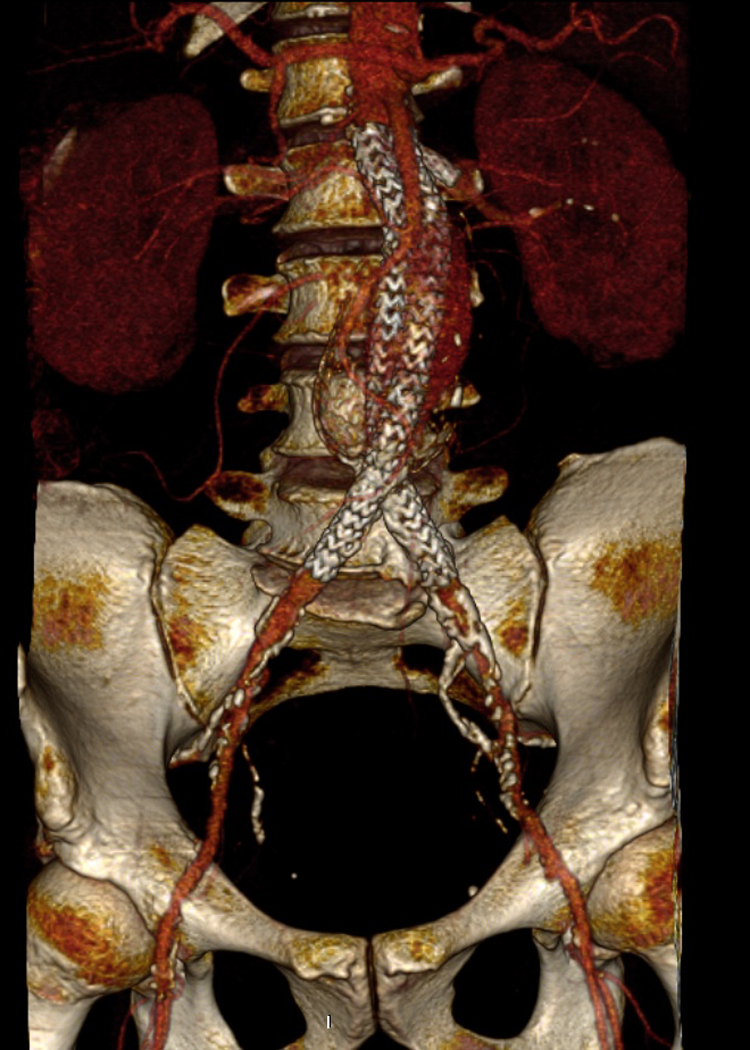
The 1 postoperative angio-CT confirms aneurysm exclusion, the absence of any endoleak or stent kinking, and visceral vessel patency and additionally the absence of residual renal artery stenosis. CT indicates computed tomography.
Computed tomography scan (at 12 months) and ultrasound examinations throughout the follow-up period (at 3, 6, 9, 12, and 18 months) demonstrated the complete exclusion of the aneurysm sac, the absence of any endoleak or stent kinking, and visceral vessel patency for all renal arteries for both patients and the absence of restenosis in patient 2 (Figures 7–9).

Ultrasound examination at 18 months demonstrated the complete exclusion of the aneurysm sac, the absence of any endoleak or stent kinking, and visceral vessel patency.
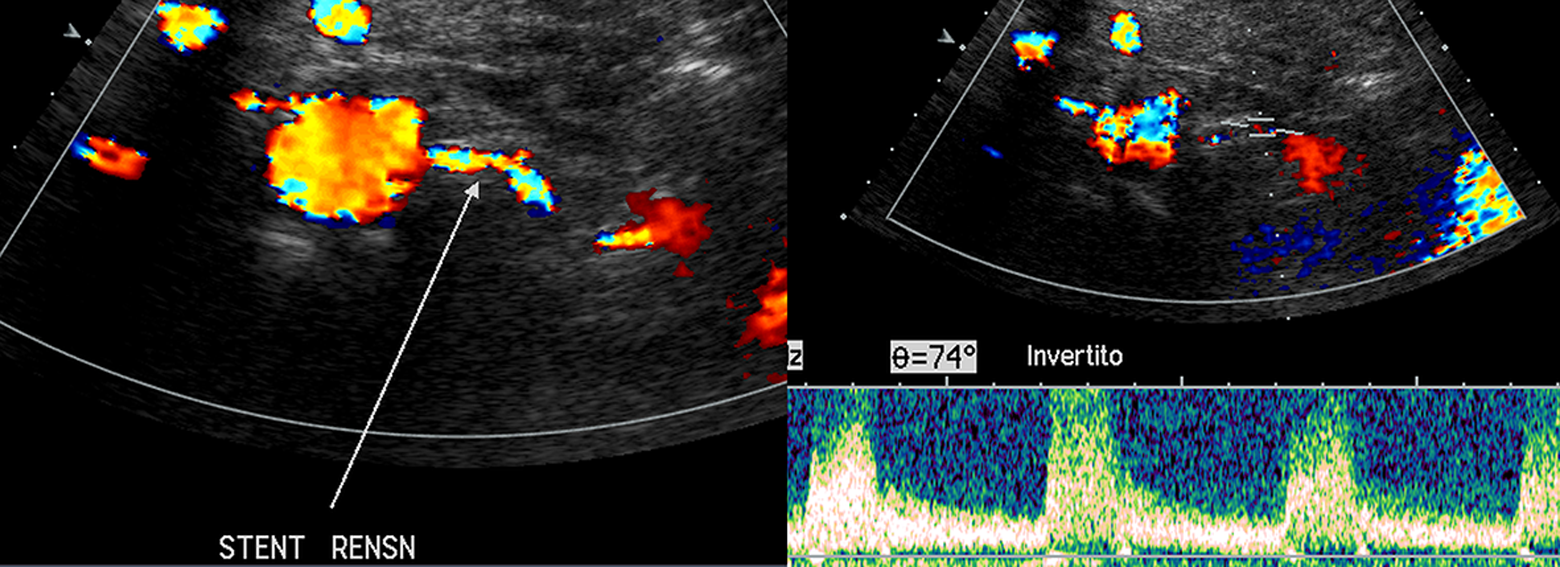
Ultrasound examinations at 18 months demonstrated the complete exclusion of the aneurysm sac, the absence of any endoleak or stent kinking, and visceral vessel patency for the renal artery and the absence of restenosis.
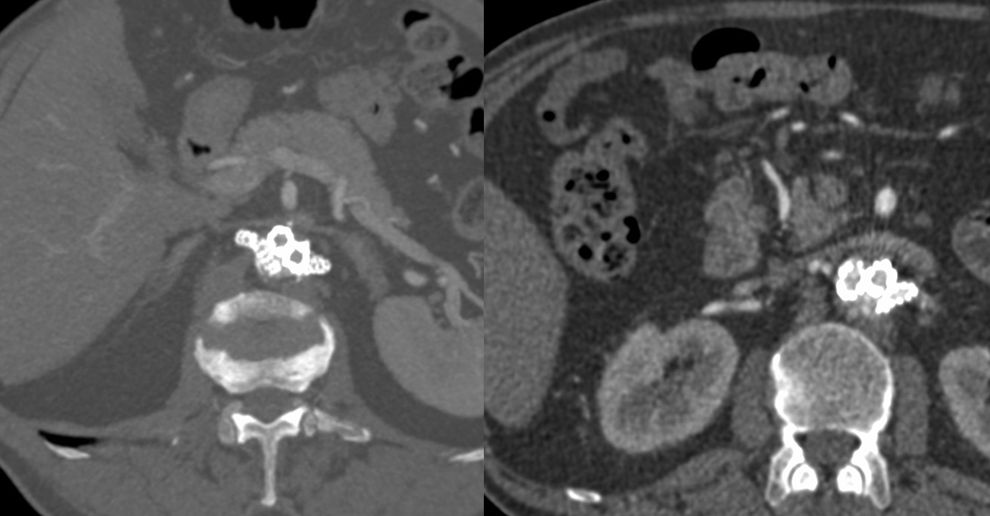
The axial 12 months CT-scan images highlighted the space disposition of the components and their full patency without compression. CT indicates computed tomography.
Discussion
Multiple endovascular options exist for the treatment of juxtarenal aortic aneurysms unsuitable for open surgery, including fenestrated and branched EVAR and ChEVAR. Fenestrated and branched EVAR techniques are technically complex and have high costs and restricted inclusion criteria and/or delay times. The ChEVAR increases the indications for treatment to include broader morphological applicability and is immediately available with off-the-shelf inventory for acute and emergent treatments. Short-term outcomes are questionable, however, mainly due to the incidence of component migration and proximal type I endoleak due to the “gutter” effect between the main endograft, the chimney stent grafts, and the aortic wall. 3 –7
More recently, the ChEVAS technique has been proposed to overcome some of the limitations associated with ChEVAR. The EVAS essentially fills the entire aneurysm and the space between the main graft and the visceral stents (covered or bare), rendering the endograft more stable in the aneurysm sac and theoretically reducing the risk of stent migration, stent kinking, and types I and II endoleak. Early experiences have reported promising early to midterm results when used within the instruction for use, but long-term durability is yet to be established. 9 EVAS associated with the chimney technique has previously been reported in the literature for complex AAA without adequate landing zones and therefore unsuitable for standard EVAR. This treatment reduces costs and immediate availability compared to fenestrated and branched endografts. 10 –12
As in the standard ChEVAR technique, the authors began the Ch-EVAS experience using covered stents for visceral segments. The authors elect to still use covered stents when the distance between the proximal edge of the Nellix stent and the renal artery ostium is >20 mm (the maximum length of a renal stent is 24 mm). For the 2 reported patients, in this series, uncovered stents were chosen to reduce the risk to renal injury, contain costs and for the ability to use shortest length stents available, and in second case, to treat the renal artery stenosis by maintaining the patency of its accessory branch.
The small area of direct contact between the bag’s biostable polyurethane endobag and the peak velocity rate of blood into the renal artery may reduce the risk of thrombosis.
In this case series, due to financial restraints, fenestrated and branched endografts were unable to be used. Both patients were assessed unsuitable for open surgery due to multiple comorbidities, previous interventions, and advanced age for patient 1, and patient 2 was still working and sexually active, and due to the increased risk of sexual dysfunction associated with open surgery, 13 an endovascular solution was preferred.
As ChEVAR has been associated with an incidence of type I endoleak, ranging from 7% to 12%, 2,5,8 ChEVAS, although as yet an unproven solution, was chosen for its promising immediate results reported in literature, in particular due to the absence of reported incidences of type I endoleak or chimney stent graft occlusion in the literature. 10 –12 Niepoth et al 14 demonstrated in an in vitro model that the total gutter volume in bilateral chimneys with the Nellix system is very low and that the risk of endoleak is reduced due to the ability of the endobags to conform to the visceral stents. Furthermore, the endobags essentially fill the aortic neck, keeping the graft metallic structures at a distance, thereby reducing graft compression and friction.
The limited experiences of ChEVAS in the literature have mostly proposed chimney stenting with covered stent grafts. As others authors 10 –12 describe in their initial experience, the polymer is expected to fit perfectly the outcurve of the visceral chimney stent graft while maintaining proximal neck sealing. The conformable polymer-filled endobags may theoretically provide a durable seal around the chimney graft with very low risk of gutters. For the authors, this is true also with bare stents.
In order to diminish the risk of gutters, the simultaneous and prolonged inflation of all the balloons is fundamental during the endobag filling and polyurethane polymerization.
Uncovered stent grafts have recently been used in association with ChEVAR, 15 but this is the first report in the literature to our knowledge where uncovered chimney stent grafts have been associated with ChEVAS. The advantages of the uncovered stent in the renal arteries are several. The smaller and more flexible delivery system potentially reduces access complications, are technically simple to deliver, and are less expensive than covered stent grafts. Ducasse et al 15 further hypothesized that the size reduction of the sheath could decrease cerebrovascular complications and improve blood flow to the stented renal artery, possibly giving an advantage in the target vessel long-term patency.
Moreover, the balloon-expandable uncovered stents are supported by a 0.014-inch guidewire with a very soft tip that can reduce the risk of renal perforation or distal artery dissection.
Furthermore, with EVAR endografts, chimney grafts are usually pushed against the aortic wall. With the EVAS alternative, the final positioning of the chimney stent is unknown, as it is encased by the endobag and it is difficult to predict whether it will go in front of or behind the stent grafts, carrying a risk of occlusion of the ostium of the mesenteric artery and celiac trunk. The authors suggest that with the bare stents, the final positioning of the chimney grafts with respect to the Nellix grafts may be less important.
However, this technique requires relatively high fluoroscopy times and amounts of contrast medium, thereby restricting patient selection to those with uncompromised renal function.
It is important to underline that in the case of type I endoleak, it could be difficult (but not impossible) to extend the stent graft proximally in order to obtain additional sealing zone. For this reason, the authors suggest maintaining guide wire position within the visceral vessels until the completion angiogram confirms complete aneurysm exclusion.
For both patients, the angio-CT at 12 months follow-up confirmed aneurysm sac exclusion, without any signs of endoleak, aneurysm expansion, or stent kinking and chimney stent graft patency evident for all stented renal arteries. Additionally, there were no signs of restenosis for patient 2. The patients’ renal functions were unaffected by the procedure.
Conclusion
The novel addition of the uncovered chimney stent grafts with ChEVAS for renal arteries could present a less technically complex approach to JAAA compared to the use of covered stents with ChEVAS. Potentially reduced access complications and procedural costs might improve long-term patency for patients, with uncompromised renal function. The 18-month follow-up results are promising, as there was no type I endoleak. However, this technique should be associated with a strict follow-up, as long-term durability is unknown.
Footnotes
Acknowledgments
The authors would like to thank Johanna Chester for her editing assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.