
Abstract
Objective:
To determine whether rehearsal using patient-specific information loaded onto an endovascular simulator prior to carotid stenting improves procedural efficiency and outcomes.
Methods:
Patients scheduled for carotid artery stenting who had adequate preoperative computed tomography (CT) imaging were considered for enrollment. After obtaining informed consent, patients were randomized to control versus rehearsal groups. Those in the rehearsal group had their CT scans loaded into an endovascular simulator (Angio Mentor) followed by case rehearsal by the attending on the simulator within 24 hours prior to the procedure; control patients underwent routine carotid stenting without rehearsal. Contrast usage, fluoroscopy time, and timing of procedural steps were recorded by a blinded observer during the actual case to determine benefit.
Results:
Fifteen patients were enrolled, with 6 patients randomized to the rehearsal group and 9 to the control. All measures showed improvement in the rehearsal group: Mean contrast volume (59.2 vs 76.9 mL), fluoroscopy time (11.4 vs 19.4 minutes), overall operative time (31.9 vs 42.5 minutes), time to common carotid sheath placement (17.0 vs 23.3 minutes), and total carotid sheath dwell time (14.9 vs 19.2 minutes) were all lower (more favorable) in the rehearsal group. The study was terminated early due to the lack of simulator access, and all P values were thus greater than .05 due to the lack of power. No strokes or other adverse events occurred in either group.
Conclusion:
Case-specific simulator rehearsal using patient-specific imaging prior to carotid stenting is associated with numerically less contrast usage, operative time, and radiation exposure, although this study was underpowered.
Introduction
High-fidelity simulation has been used for surgical education over the past decade or more. In general, simulation allows training without any chance of patient harm and allows repetition, error recovery, experimentation, and other such factors that cannot be accomplished clinically. Until recently, simulators presented preloaded scenarios and allowed performance of generic tasks (carotid stenting, renal and other vessel intervention, endograft placement) only.
For the past 5 years or more, some simulators have been produced that allow uploading of actual patient data derived from conventional imaging (most commonly, CT scanning). Considerable postprocessing is usually required, but this allows an actual patient’s data, rather than a generic procedure, to be available for use. This technique has been shown to be able to predict the endograft sizing prior to endovascular aneurysm repair. 1 Carotid stenting is a technically challenging procedure with several important decisions involved (common carotid artery [CCA] cannulation, embolic protection, stent, and balloon sizing) and clear advantages to short procedure times and efficient technique. Such a procedure seems ideal to test the hypothesis that rehearsal of the actual case, using patient-specific data, will improve technical performance of the real procedure.
Methods
Institutional review board (IRB) approval was obtained at both the University of Rochester, where the study was started, and the University of South Florida (USF), where it continued after 2011. Patients undergoing carotid stenting for high-risk lesions who had computed tomography (CT) scans adequate for both carotid imaging itself and to meet the technical requirements of the simulator were offered enrollment. Those enrolled were randomized by computer to either the rehearsal or control groups.
Patients in the rehearsal group had their CT scans uploaded into an endovascular simulator (Angio Mentor; Simbionix, Airport City, Israel) available at both locations. The scans underwent postprocessing to adequately identify each vessel and allow the simulator software to recognize the procedural steps. The operating surgeons (K.A.I., M.J.S., P.A.) then performed the simulated carotid stent, if possible with the planned first assistant, within 24 hours of the procedure. No specific records were kept at this point, but the surgeon was free to “experiment” with different catheters for CCA access, embolic protection device (EPD), stent, and balloon sizes and anything else needed for the actual procedure. Patients then underwent carotid stenting, and an observer blinded to the group recorded subjective evaluation of the flow of the procedure as well as objective data points including contrast usage, fluoroscopy time, and timing of procedural steps. Control patients simply underwent stenting, without prior rehearsal. Continuous variables were analyzed using Student t test.
Results
The study was started in Rochester, New York, in July 2010; 13 procedures (11 patients) were performed by 2 authors (K.A.I. and M.J.S.). After the senior author’s relocation to the USF in 2011 and IRB approval there, the study continued in Tampa, Florida, with 5 procedures (4 patients) again performed by 2 authors (K.A.I. and P.A.). Identical equipment and techniques were used. Access to the rehearsal module of our simulator was terminated for financial reasons in July 2013, after 15 patients had been enrolled.
Six patients were randomized to the rehearsal arm and 9 to the control. Contrast volume, fluoroscopy time, and total operative time, as well as time to CCA cannulation and CCA total sheath time were all lower in the rehearsal group; although due to the small number of patients enrolled, statistical significance could not be demonstrated (Table 1). Subjective input from the blinded observer did note improved efficiency and procedural flow in the rehearsal group. Surgeons uniformly felt that the rehearsed procedure had excellent predictive value (anatomy and tools needed for CCA cannulation) for the real procedure and uniformly rated the simulated procedure as extremely helpful.
Procedural Details for the 2 Procedural Arms.a
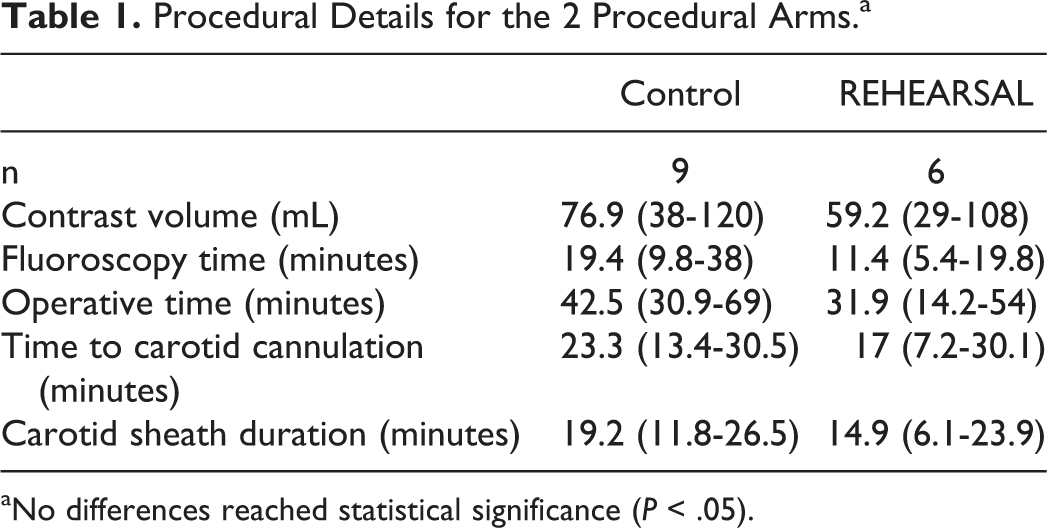
aNo differences reached statistical significance (P < .05).
Discussion
Rehearsing an actual carotid stenting case on a simulator using patient-specific data just prior to the case itself was associated with reduced contrast and radiation doses and decreased procedure time. The only other study published to date using patient-specific carotid artery stenting rehearsal found similar subjective benefits to rehearsal based on physician response to questionnaires of procedural flow and challenge but was not designed to compare to nonrehearsed procedures. 2
The flaw of this study is obvious—it was underpowered enough that significance was not reached for any comparison. Enrollment was extremely difficult (15 patients in 3 years), due to multiple factors. First, after the initial burst of activity in this area, the number of carotid stents we perform has declined due to data showing less of a benefit than initially postulated 3 -5 as well as reimbursement limitations. Second, the majority of our patients were stented within various clinical trials and/or registries, which prohibit enrollment in other trials. Third, we did not feel (nor did we have funding or sought IRB permission for) CT scans should be obtained solely for this trial, so patients could only be enrolled if they had a CT scan done for a specific reason. Having said this, the CT scan had to have imaged low enough to resolve the aorta into both ascending and descending segments (ie, below the lesser curve) or the simulator could not recognize the arch. Finally, we experienced a lull of 30 months due to the senior author’s relocation and IRB approval process required at the USF. The trial ultimately was halted when our rehearsal module license at USF expired and the financial burden of maintaining this solely for this trial (see Discussion below) was not judged worthwhile. Our decision was to analyze and disseminate these results as hopefully helpful and provocative, while acknowledging that we cannot claim to have “proved” or “discovered” anything.
Simulation has become a part of the curriculum in most training programs but has typically been used for relatively generic purposes. As mentioned in the Introduction, they typically offer training in procedures by means of preset scenarios. These allow procedural training at all levels without harm to the patient and allow us to do things we cannot do in real life, such as repetition, recovery from errors, experimentation, and so on. They have not typically been used for training in specific situations, although endograft sizing has been explored, as above. 1 Calatayud and colleagues were able to demonstrate a significant reduction in operative time for performance of laparoscopic cholecystectomy when “warming up” by performing a simulated laparoscopic cholecystectomy on a simulator right before entering the operating room compared to those who did not simulate ahead of time, 6 but again this “warming up” was generic. Similarly, endovascular skills have been specifically shown to improve with reduced procedure times and contrast volume for thoracic endograft placement, endovascular abdominal aortic aneurysm repair, and carotid artery stenting. 7 -10 Unfortunately, the shortcoming of each of these studies continues to be the lack of translation to real-world procedural assessment as they all rely upon cohort comparison from initial simulator trial to later simulator trials. 11
Carotid stenting seems to be an ideal situation where patient-specific rehearsal prior to the procedure would be of benefit. Carotid stenting is a procedure with several relatively stereotypical steps and has the complimentary dichotomy of requiring significant decision-making on the fly (catheter choice for CCA access, EPD, stent, and balloon size) while needed to reduce procedure time, at least with regard to CCA sheath and catheter dwell time. Our experience, although highly subjective, was strongly favorable. The simulated anatomy was strikingly predictive of the actual anatomy, and in many cases, the surgeon could choose the right catheter to use (eg, forward angled vs recurve) for CCA cannulation based on the simulated case.
Two other barriers to implementing this technique (patient-specific rehearsal prior to carotid stenting) should also be discussed. First is the logistics of uploading the images. Specific techniques must be used (although Digital Imaging and Communications in Medicine data are generically recognized), and approximately 20 or 30 minutes of postprocessing time by a trained operator are needed to allow the simulator to recognize the relevant anatomy. Second, simulators are usually not in the operating room but rather are typically off-site in a simulation laboratory making daily use impractical.
Could we correct these factors? First, our findings should be confirmed in a more rigorous fashion, and ideally, it should be shown that actual clinical outcomes are improved by preoperative rehearsal. Two things are needed to make this technique clinically useful. First will be a more streamlined uploading process. In the ideal setting, the simulator should “talk” to the radiology computer and uploading should be automatic, without (human) postprocessing or other effort required. Secondly, such a simulator should be located in the operating suite. These are both difficult to accomplish, but think of the possibilities. Instead of grabbing an extra cup of coffee between cases, the surgeon and/or assistants could migrate to the simulator and practice their next case once or twice to warm up. Or, the resident could call the surgeon over and say “watch me do this”—and if he or she demonstrates that they can properly perform the case on the simulator, the surgeon would be much more comfortable allowing them to act as the primary surgeon. Perhaps the arch is difficult—the surgeon could experiment with several catheters, picking the one that seems to work best prior to the case, thus saving money and time by doing it right the first time. We studied carotid stenting, but this concept would seem to be applicable to any nontrivial endovascular procedure, including fenestrated and complex endografts, renal intervention, branch aneurysm treatment, and so on.
Conclusion
Due to logistical and financial pressures, we could not enroll enough patients in this trial to achieve statistical significance. However, rehearsing a carotid stenting procedure on an endovascular simulator using actual imaging from the specific patient prior to performing the actual procedure was associated with lower radiation doses, lower contrast doses, and shorter procedure times relative to control. We present our experience in the hopes that others will be able to expand upon this concept in order to determine whether this is a cost-effective and truly beneficial strategy to pursue.
Footnotes
Authors’ Note
This study was presented at the Association of Program Directors in Vascular Surgery Spring Meeting; Chicago, Illinois; April 2016.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.