
Abstract
Purpose:
To describe the uses and advantages of hybrid vascular grafts (HVGs) for complex iliofemoral revascularization procedures.
Case Report:
We report 3 cases of iliofemoral occlusions repaired with the Gore HVG, used as an alternative technique to standardized common femoral artery (CFA) endarterectomy associated with iliac stenting or open repair. The indication in each of the 3 cases was different: In the first case, there was an absent CFA secondary to a mycotic pseudoaneurysm, in the second case, an iatrogenic lesion of the posterior wall of the CFA during the intervention was performed, and in the third case, the indication was because of thrombosis of a previous iliofemoral revascularization procedure.
Conclusion:
Although we only present 3 cases, the Gore HVG can be useful for complex iliofemoral revascularizations, serving as an alternative to standardized CFA endarterectomy plus iliac stenting in cases where there is a damaged or absent CFA, especially in high-surgical risk patients.
Keywords
Introduction
The Gore hybrid vascular graft (GHVG; W.L. Gore & Associates, Flagstaff, Arizona) is an innovative graft designed for sutureless anastomosis, allowing an easy insertion and deployment into target vessels. It has been used in arteriovenous access grafts for dialysis, 1 visceral revascularization during open thoracoabdominal aortic aneurysm repair, 2 procedures of the supra-aortic trunks, 3–4 and infrainguinal vascular revascularization procedures; however, their use for iliofemoral occlusive disease (IFOD) has yet to be reported. Herein, 3 complex cases of Ilio-Femoral (IF) reconstruction with a GHVG are reported, just representing some of the possible new applications of these conduits.
Materials and Methods
Case 1
A 68-year-old male, former smoker with a medical history including chronic obstructive pulmonary disease, a vagotomy with gastrojejunostomy and a left hemiglossectomy with bilateral lymph node removal, and associated radiotherapy due to an epidermoid oral carcinoma. His prior vascular history included an aortobifemoral bypass (ABF) with a 14 × 7 mm Dacron graft in 2001. Eighteen months later, the patient was admitted with occlusion of the right limb of the ABF and an ischemic foot ulcer: treated with a crossover left to right common femoral artery (CFA) bypass plus a right above-the-knee femoropopliteal bypass. After multiple reinterventions of the right lower limb, a transfemoral amputation was performed in 2009. Three years later, the patient was readmitted with a ruptured pseudoaneurysm of the left CFA. Resection of the pseudoaneurysm with interposition of a cryopreserved arterial homograft from the left limb of the ABF to the deep femoral artery (DFA) was performed. In 2015, the patient presented a left supramalleolar ulcer associated with rest pain and an IF occlusion. A computed tomography angiography (CTA) showed complete occlusion of the ABF graft, with patency of his native aorta and left common iliac artery (CIA), occlusion of the left external iliac artery (EIA) and the CFA, with recanalization into the DFA, and the popliteal artery above the knee. A 6F 90-cm length introducer sheath was inserted through a left brachial artery puncture, and antegrade subintimal recanalization of the left iliac axis was achieved with a 0.035-inch hydrophilic guide wire (Figure 1A). After open dissection of the left groin, the guide wire was retrieved from the distal left EIA. Predilation of the iliac axis was performed with a 7-mm catheter balloon. A 14F peel-away introducer sheath was introduced through the CFA, and the endoluminal portion of an 8 × 100 mm GHVG was released in the EIA, which was then extended proximally with an 8 × 57 mm Omnilink-Elite (Abbott Vascular, Abbott Park, Illinois). The distal portion of the GHVG was anastomosed to the distal DFA (Figure 1B). The completion angiography demonstrated an optimal result (Figure 1C). In order to complete the procedure, a expanded polytetrafluoroethylene (ePTFE) bypass was performed from the GHVG to the above-the-knee popliteal artery . In this case, the use of the GHVG averted the necessity of an abdominal approach, avoiding the need of redissection of the previous graft limb, decreasing both the operative time as well as the surgical risk.
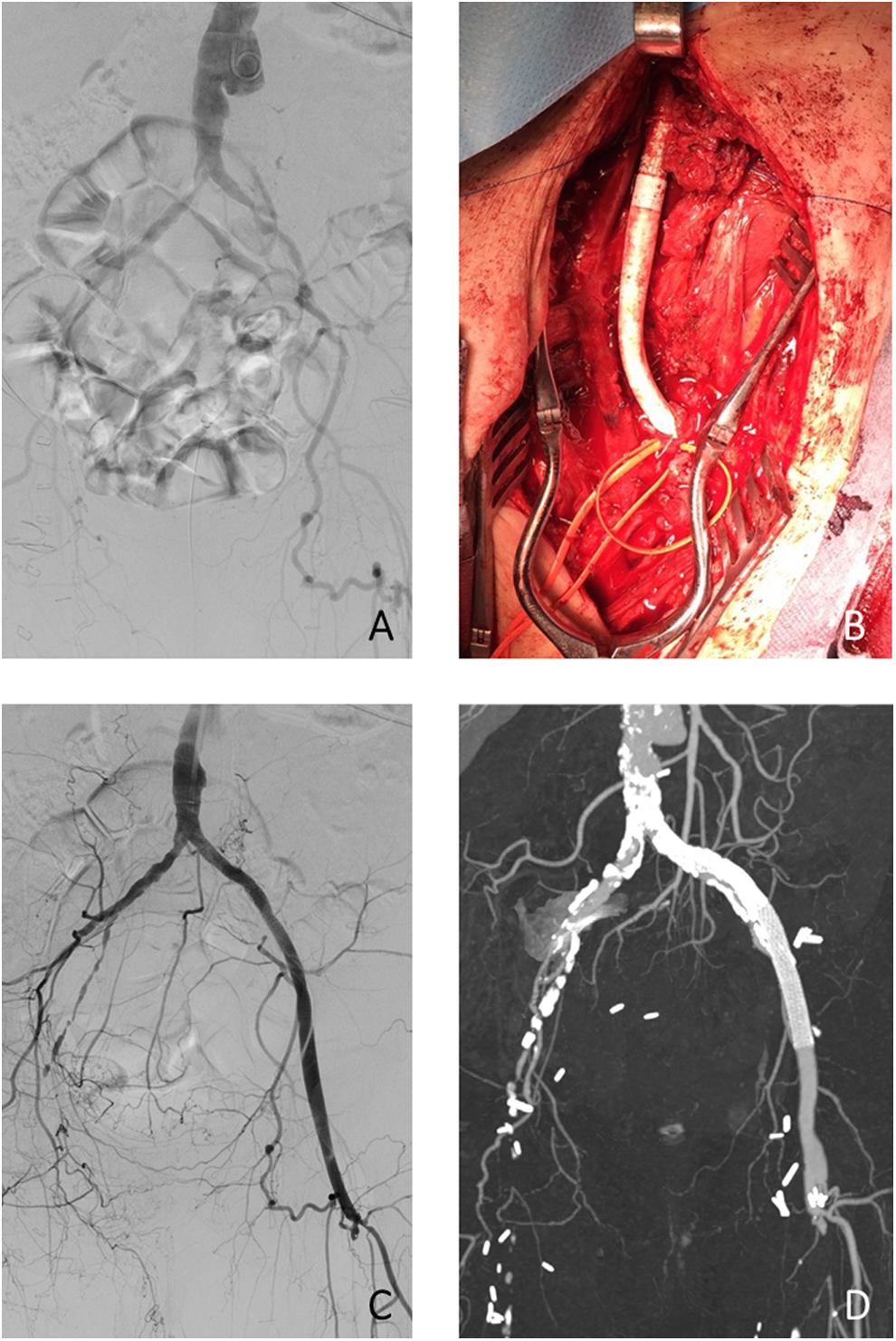
A, Intraoperative diagnostic angiography through a left brachial access. B, Distal anastomosis of the GHVG on the DFA. C, Completion angiography. D, CTA control 1 year after the intervention with patency of the GHVG. DFA indicates deep femoral artery; GHVG, Gore hybrid vascular graft.
The postoperative period was uneventful and the ulcer healed completely. At the 2-year follow-up, patency of the GHVG was confirmed (Figure 1D), with occlusion of the femoropopliteal bypass. Currently, the patient is asymptomatic without new skin lesions.
Case 2
A 74-year-old male with a previous medical history of hypertension and hyperlipidemia. In 2012, he underwent endovascular repair of an abdominal aortic aneurysm with a Zenith (Cook Medical, Inc, Bloomington, Indiana) aorto-bi-iliac endoprosthesis through bilateral groin dissection. He was admitted 4 years later due to right lower limb rest pain. An angio-CTA showed nonocclusive thrombus inside the main body of the endograft with occlusion of the right limb, diffuse atherosclerotic disease of the right iliac axis, occlusion of the right CFA, and the superficial femoral artery (SFA), with patency of the DFA and popliteal artery (Figure 2A and B) and, on the left side, patency of the endograft limb, with atherosclerotic disease of the EIA and CFA, and chronic femoropopliteal occlusion. A redo-dissection of both groins was performed, but an iatrogenic injury of the right CFA occurred, complicating a standard endarterectomy and preservation of the artery. A kissing balloon stenting technique was performed with two 8 × 150 mm Viabahn stentgrafts (W. L. Gore & Associates) on the right side and a 13 × 100 mm on the left. A patch angioplasty of the left CFA was performed. The right CFA was excluded and closed with a running 5/0 polypropylene suture, achieving revascularization with an 8 × 100 mm GHVG from the right EIA (extending distally from the previously implanted Viabahn stentgraft) to the DFA. In this case, the GHVG served as an alternative solution to an IF or crossover bypass graft given the damage to the CFA. The postoperative period was uneventful and at the 8-month follow-up, the grafts remain patent with no procedural related complications (Figure 2C).
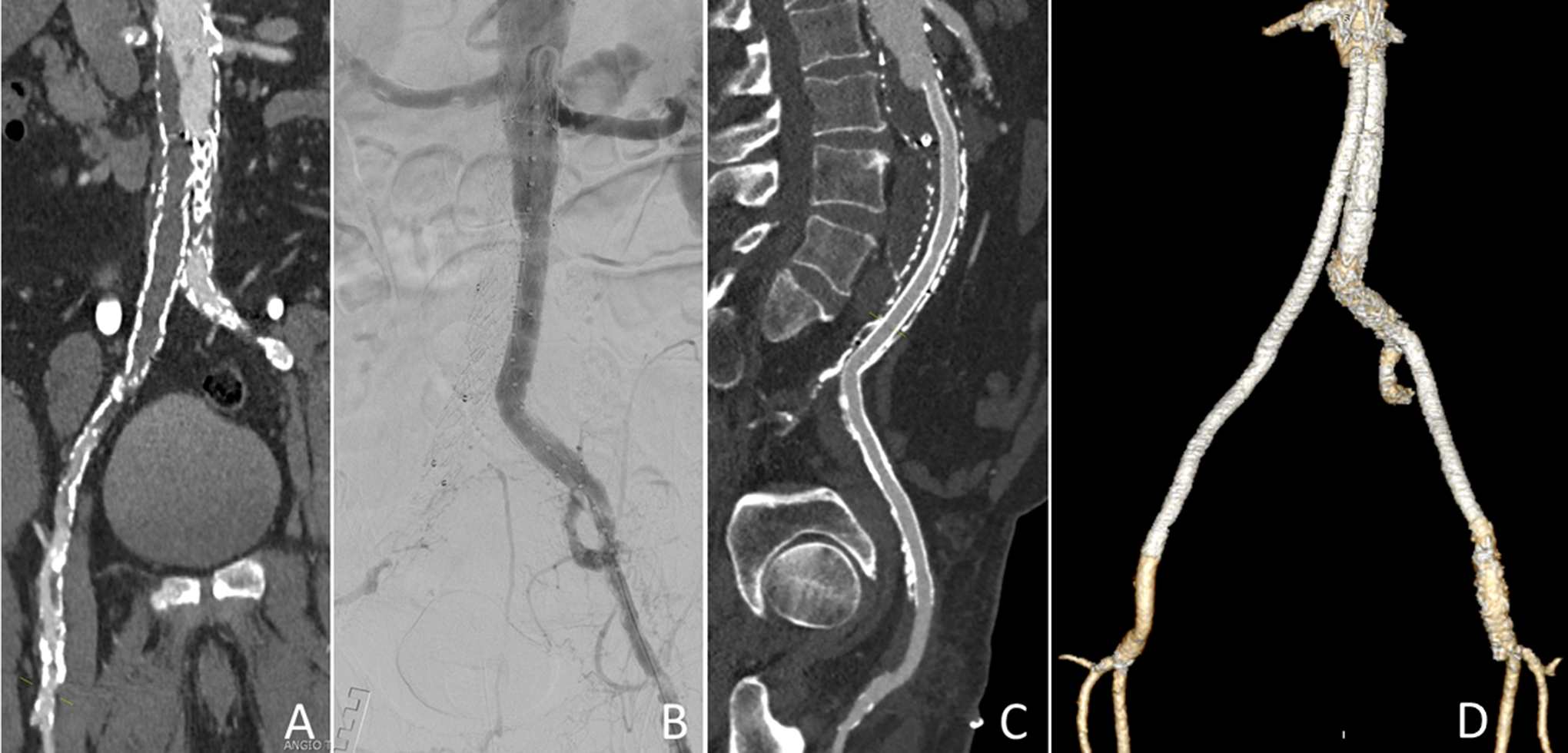
A, CTA showing complete obstruction of the right limb of the endograft. B, Intraoperative diagnostic angiogram. C, Control CTA performed 1 month after the intervention was graft patency, and the distal anastomosis can be seen. D, 3-D reconstruction of control CTA 1 month postintervention.
Case 3
A 54-year-old male with morbid obesity and a past vascular history of a left CIA angioplasty and stenting with an 8 × 40 mm E-Luminexx (C. R. Bard, Inc, Murray Hill, New Jersey) in 2010. In 2012, a new left iliac angioplasty and stenting with an 8 × 100 mm and a 7 × 100 mm Viabahn, plus a short CFA 8-mm Dacron bypass graft was performed. Three years later, the patient referred left intermittent claudication at less than 50 meters due to an IF occlusion and an ankle-brachial index of 0.6 that dropped to 0.25 after treadmill exercise testing. An angio-CTA demonstrated occlusion of the iliac stent grafts as well as of the short CFA bypass graft with patency of both the SFA and the DFA (Figure 3A). Redo-dissection of the left groin with exposure of the occluded bypass, the SFA, and the DFA (both with a minimum diameter) was performed. Through puncture of the previous Dacron graft, recanalization of the left iliac axis was achieved. Percutaneous right access with a 7F introducer sheath was gained. The Dacron bypass graft was opened, and a proximal thrombectomy was performed achieving adequate blood flow. A 16F introducer sheath was left in place, deploying two 8 × 59 mm Atrium Advanta V12 (MAQUET Holding B.V. & Co. KG, Rastatt, Germany) at the aortic bifurcation using the kissing stent technique. An 8 × 100 mm Viabahn was released on the left side, from which an 8 × 100 mm GHVG was extended to the femoral bifurcation. In this case, the GHVG obviated the need for clamping the previously stented EIA. The postoperative period was uneventful and at the 6-month follow-up, the GHVG remains patent without signs of stenosis (Figure 3B).

A, Preoperative CTA where obstruction of the previous iliac stenting and of the short CFA bypass is shown. B, Postoperative control CTA performed 1 month after the intervention. CFA indicates common femoral artery.
Discussion
The GHVG is an innovative, heparin-bonded ePTFE graft with a nitinol-reinforced end. 5 Isolated reports have demonstrated its usefulness in arteriovenous access, visceral arteries, supra-aortic trunks, and infrainguinal vascular disease revascularization. 1 –4 However, many of their potential applications have not been described and their use in the iliac sector has yet to be reported. Herein, we report 3 complex cases of IF revascularization showing some of the potential benefits of using these new vascular conduits.
The current gold standard for the treatment of extensive IFOD continues to be open surgical reconstruction with ABF or IF bypass; however, during the last decade, less invasive endovascular and hybrid procedures have gained popularity as an alternative to open surgery. In 2011, Piazza et al reported their results comparing iliac artery stenting plus open femoral endarterectomy with open surgical reconstruction for severe iliac and common femoral occlusive disease, concluding that this hybrid approach presents a shorter hospitalization and similar early and long-term efficacy when compared to open repair for both Trans-Atlantic Inter-Society Consensus (TASC) A-B and C-D lesions and it should be considered a first-line approach for all patients with IF occlusive disease, particularly for those with high surgical risk. 6
Currently, the first-line approach for the treatment of severe IFOD in our center are hybrid procedures combining a CFA endarterectomy with patch angioplasty plus iliac stenting, with preference for covered stents when long or complex aortoiliac occlusions are present; given their superior patency over bare metal stents. 7 The 3 cases presented in this article have severe and long aortoiliac occlusive lesions associated with either a damaged or absent CFA, without the possibility of performing a standardized CFA endarterectomy. Two other patients with extensive IF occlusive disease, multiple previous vascular interventions, and an inadequate CFA for endarterectomy have also been treated in our center with a GHVG.
The GHVG has 2 main advantages. On one hand, the covered self-expanding proximal end allows for a “sutureless anastomosis,” allowing the achievement of inflow from a distal access, obviating the need for an aortoiliac anastomosis and avoiding an abdominal approach, extensive redo-dissection, clamping…saving time, and reducing the surgical risk. It also serves as an alternative to extra-anatomical crossover bypass. On the other hand, their advantage over covered stents is a distal part that is not stented, allowing for an easy suture. A similar hybrid technique for the treatment of IFOD was reported by Ahanchi et al; however, the authors used the Viabahn stentgraft as the conduit, increasing the difficulty of the distal anastomosis. 8
The use of the GHVG opens up the possibility of performing hybrid repair in complex IF lesions using a covered stent for treatment of the proximal aortoiliac lesion and a direct anastomosis upon the CFA or DFA in patients with an inadequate or absent CFA or in those cases where a standardized CFA endarterectomy cannot be performed. Although just 3 patients are reported here, the postoperative period was uneventful in all of them and after 24, 8, and 6 months of follow-up, respectively; the GHVGs remain patent; and there have been no further complications.
Conclusion
Hybrid vascular grafts are useful for complex IF revascularizations, serving as an alternative to standardized CFA endarterectomy plus iliac stenting in cases with a damaged or absent CFA, especially in high-surgical risk patients.
Footnotes
Authors’ Note
Part of this manuscript has been presented as an oral communication in the “62 Congreso Nacional de la SEACV”, June 7-10 2016, Sitges, Barcelona, Spain. All the authors have read and approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.